

Subscribe to RSS
DOI: 10.1055/s-0038-1636934
An Unexpected Donor Site Complication after Aesthetic Rhinoplasty: Arteriovenous Fistula of the Superficial Temporal Artery
Authors
Publication History
Publication Date:
09 April 2018 (online)

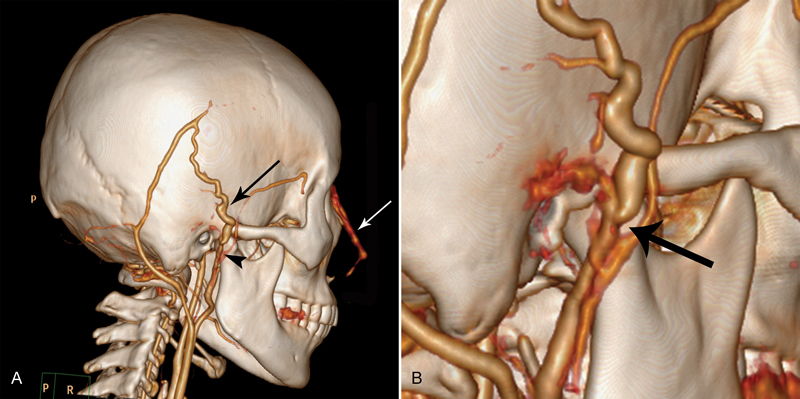
A 36-year-old woman presented with a painless, slowly growing pulsating mass and pulsatile tinnitus in the right superior preauricular region. Two months prior to the visit, she underwent primary rhinoplasty with dorsum augmentation using a silicone implant and tip graft using autologous cartilage harvested from the right concha via an anterior approach. Two days after surgery, a pulsating mass and accompanying pulsatile tinnitus were noticed in the right superior preauricular region. These conditions were not present prior to the surgery. Physical examination revealed a compressible, painless, pulsatile mass ∼1 cm in diameter in the right preauricular region. A faint linear scar ∼2 cm in length was detected in the anterior auricular skin 2 mm inside the rim of the conchal bow ([Fig. 1]). Computed tomography angiography delineated an arteriovenous fistula (AVF) between the trunk of the right superficial temporal artery and the superficial temporal vein ([Fig. 2]). Surgical resection of the lesion was achieved and there was no sign of recurrence after 6 months follow-up.

Rhinoplasty remains one of the most commonly performed and popular aesthetic surgical procedures. Served as a versatile cartilage source for both basic and more sophisticated reconstructive procedures, the ear is considered to be an optimal donor site with an inconspicuous complication rate, and most complications are minor. However, an AVF as a donor site complication of aesthetic rhinoplasty is unexpected and has not been reported previously. Furthermore, it requires intervention and should not be ranked as a minor complication.
Since the first case following hair transplantation was published in 1970, only 15 cases of AVF have been reported that developed after cosmetic surgical procedures. In the present case, the AVF was thought to be caused by an inadvertent penetrating trauma of the adjacent arteries and veins during dissection of the superior part of the cymba concha by the tissue scissor rather than a blunt trauma by the retractor, as the condition presented only 2 days after the surgery. Moreover, the location of the fistula was well adjacent to the anterosuperior part of the cymba concha, making the causal relationship between the harvesting and AVF more convincing.
Although chances of superficial temporal vessels injury through conchal cartilage harvesting are slim, the dissection has to be well beyond the conchal fossa to get to the preauricular position of the superficial temporal vessels. However, taking into account the present case, when the harvesting was performed with an anterior approach, there might be a higher risk of iatrogenic trauma to the superficial temporal vessels compared with a posterior approach given that the dissection is more adjacent to the vessels. Therefore, a meticulous dissection, bleeding control for a clear surgical field, and avoiding rough vessel injury by retractor should be emphasized. Furthermore, care must be taken to avoid injury of the superficial temporal vessels when the dissection is in the region between the inferior crus of antihelix and the superior border of the root of helix. The present case widens the complication spectrum of conchal cartilage harvesting.