

Subscribe to RSS
DOI: 10.1055/s-0033-1350298
Diffusion-Weighted MR Imaging of Benign and Malignant Breast Lesions Before and After Contrast Enhancement
Diffusiongewichtete MR-Bildgebung von benignen und malignen Brustläsionen vor und nach KontrastmittelgabeAuthors

Abstract
Purpose: Many publications describe the use of diffusion-weighted imaging (DWI) in breast MRI. This article addresses the question of when to apply the DWI sequence in the course of the scan protocol. The effect of T1-shortening contrast media (CM) on the ADC values of breast lesions is investigated.
Materials and Methods: Data were acquired on a 1.5 T scanner. 60 patients with 79 lesions (20 benign, 59 malignant) were included. The DWI sequence (4 mm slice thickness, b-values: 50, 400, 800) was applied before and after CM administration. Before calculating the ADC map, the b50, b400 and b800 series were analyzed concerning lesion displacement. ADC values before and after CM application were compared.
Results: The mean lesion size was 1.5 ± 0.8 cm. On the basis of the b50 and b400 measurements, the mean ADC value of benign lesions was 1.89 ± 0.30 × 10-3 mm2/s before and 1.85 ± 0.28 ×10-3 mm2/s after CM administration. The consecutive values for two pure mucinous carcinomas were 1.88 × 10-3 mm2/s and 1.81 × 103 mm2/s and for the remaining malignant lesions 1.00 ± 0.18 × 10-3 mm2/s and 0.88 ± 0.21 × 10-3 mm2. On the basis of the b50, b400 and b800 measurements, the mean ADC value of benign lesions was 1.99 ± 0.37 × 10-3 mm2/s before and 1.97 ± 0.30 × 10-3 mm2/s after CM application, whereas the mean ADC value of the malignant lesions was 0.90 ± 0.14 × 10-3 mm2/s before and 0.80 ± 0.14 × 10-3 mm2/s after CM application. While there was no significant change for benign lesions, the ADC value decrease in post-contrast malignant lesions was highly significant.
Conclusion: DWI after CM is possible and even leads to slightly better lesion discrimination between benign and malignant. However, further studies need to be performed to verify this.
Citation Format:
• Janka R, Hammon M, Geppert C et al. Diffusion-Weighted MR Imaging of Benign and Malignant Breast Lesions Before and After Contrast Enhancement. Fortschr Röntgenstr 2014; 186: 130 – 135
Zusammenfassung
Ziel: In vielen Publikationen werden diffusionsgewichtete Sequenzen für die MRT der Brust beschrieben. In dieser Arbeit soll die Frage beantwortet werden, wann die diffusionsgewichtete Sequenz im Scanprotokoll gemessen werden soll, wobei ein Effekt von T1-Zeit verkürzendem Kontrastmittel (KM) auf den ADC-Wert von Brustläsionen untersucht wird.
Material und Methoden: Die Untersuchungen wurden an einem 1,5 T-MRT durchgeführt. Eingeschlossen wurden 60 Patientinnen mit 79 Brustläsionen (20 benigne, 59 maligne). Die diffusionsgewichtete Sequenz (4 mm Schichtdicke, b-Werte: 50, 400 und 800) wurde vor und nach KM-Gabe gemessen und die entsprechenden ADC-Werte der Läsionen verglichen. Vor der Berechnung der ADC-Werte wurden die Läsionen bezüglich ihrer konstanten Lokalisation in den diffusionsgewichteten Sequenzen analysiert.
Ergebnisse: Die mittlere Größe der Läsionen war 1,5 ± 0,8 cm. Auf der Basis der b50- und b400- Messung betrug der durchschnittliche ADC-Wert der benignen Läsionen 1,89 ± 0,30 × 10-3 mm2/s vor und 1,85 ± 0,28 × 10-3 mm2/s nach KM-Gabe. Die entsprechenden Werte für zwei muzinöse Karzinome betrugen 1,88 × 10-3 mm2/s und 1,81 × 103 mm2/s und für die übrigen malignen Läsionen 1,00 ± 0,18 × 10-3 mm2/s und 0,88 ± 0,21 × 10-3 mm2. Auf der Basis der b50-, b400- und b800-Messung betrug der durchschnittliche ADC-Wert der benignen Läsionen 1,99 ± 0,37 × 10-3 mm2/s vor und 1,97 ± 0,30 × 10-3 mm2/s nach KM-Gabe. Der mittlere ADC-Wert der malignen Läsionen betrug 0,90 ± 0,14 × 10-3 mm2/s vor und 0,80 ± 0,14 × 10-3 mm2/s nach KM-Gabe. Während der ADC- Wert der gutartigen Läsionen durch das Kontrastmittel nicht signifikant beinflusst wurde, war er bei den malignen Läsionen nach Kontrastmittelgabe signifikant niedriger.
Schlussfolgerung: Die Messung der diffusionsgewichteten Sequenz ist auch nach KM-Gabe möglich und führt zu einer besseren Differenzierbarkeit von malignen zu benignen Läsionen. Um dieses Ergebnis zu verifizieren sind weitere Studien nötig.
Introduction
Magnetic resonance imaging (MRI) of the breast has a high sensitivity for the detection of malignant beast lesions of 94 – 100 % [1] [2] [3]. Despite several criteria for malignant breast lesions such as morphology and signal characteristics in T2-weighted and dynamic sequences [4] [5], there is a wide range of reported specificities of 77 – 96 % [1] [2] [3]. Recent publications describe an increase in specificity with the use of diffusion-weighted imaging (DWI) [6] [7] [8]. Moreover, DWI can be useful for the detection [9], assessment [10] [11] [12] [13] [14] or treatment response monitoring [15] [16] of breast cancer. However, when using DWI, the applied pulse sequences, b-values and approach (before or after contrast administration, selected slices or complete volumes) differ in most publications [17]. This article investigates the effect of T1-shortening contrast media (CM) administration on the ADC values of fat saturated DW-EPI and its impact on the ability to differentiate benign from malignant breast lesions.
Materials and Methods
The institutional review board of the University of Erlangen-Nuremberg approved this study and waived the need for informed consent.
Patients
From August 2011 to September 2012, 379 breast MRI examinations were performed at the University Hospital Erlangen. Patients who took part in another study (n = 74) and patients who did not receive contrast media (CM) (n = 19) were excluded. From our local database we retrieved all patients who had a histologically verified mass lesion before or after MRI exam. The lesions eligible for the study defined as mass lesions according to the BI-RADS lexicon were greater than 5 mm in size in the dynamic MR sequence and were also identifiable on the DWI sequences.
MRI
Images were acquired on a 1.5 T scanner (Magnetom Avanto®, Siemens Healthcare, Erlangen, Germany) with a dedicated breast array coil (Siemens Healthcare, Erlangen; Germany) and the patient in a prone position. Our standard breast MRI protocol included an axial 2 D T2-weighted STIR sequence (TR/TE/TI, 7200/85/150 msec, FOV 380 × 380 mm, matrix = 512 × 358, slice thickness 3 mm, resolution: 1.1 × 0.7 × 3.0 mm, acquisition time: 3.30 min), a pre- and post-contrast sagittal T1-weighted 3 D gradient echo (GRE) pulse sequence (TR/TE, 21/4.8 msec, FOV 180 × 180 mm, matrix = 512 × 512, slice thickness 2 mm, resolution: 0.4 × 0.4 × 2.0 mm, acquisition time: 4.42 min), and an axial 3 D dynamic GRE pulse sequence (TR/TE, 11/4.8 msec, FOV 360 × 360 mm, matrix = 512 × 430, slice thickness 3 mm, resolution: 0.8 × 0.7 × 3.0 mm, acquisition time per time point: 1:07 min) with one acquisition before and acquisitions up to 6 min after CM. The contrast media (0.1 mmol/kg body weight gadobutrol, Gadovist®, Bayer Schering Pharma, Berlin, Germany) was applied into the cubital vein after the first of the six dynamic acquisitions with an MRI compatible power injector (Spectris®, Medrad, Pittsburgh, PA, USA) with a flow of 1.0 mL/sec followed by a 20 cc saline flush.
Diffusion-weighted (DW) images were acquired in axial slice orientation with a diffusion-weighted spin-echo EPI with fat saturation (DW SE-EPI fs) pulse sequence (TR/TE/TI, 4100/98/150 msec, FOV 340 × 170 mm, matrix = 192 × 96, resolution 1.8 × 1.8 × 4.0 mm). The DW-EPI sequence using a chemical shift selective fat suppression pulse was applied before and subsequent to the administration of contrast media following the T1-weighted dynamic scan protocol. DWI measurements were acquired with two averages of 26 slices with a slice thickness of 4 mm and b-values of 50, 400 and 800 s/mm² using 3-scan trace calculation resulting in a scan time of 1.31 minutes.
Image analysis
The breast MRI was evaluated in consensus by two board-certified radiologists (J. R., W. E.) with more than eight years of breast MRI experience.
The inclusion criteria for the evaluation of the DW images were histologically proven focal mass lesions with a diameter of more than 5 mm or centrally necrotic lesions with an enhancing rim of more than 5 mm. The lesions had to be clearly identifiable in one of the early (one to three minutes after CM application) post-contrast subtracted images of the dynamic MRI series and in the DW sequences. Lesions were first located in the subtracted images of the dynamic protocol and then identified in the corresponding DW images. As the ADC map is calculated on the basis of a pixel-by-pixel analysis, it is essential to have no lesion displacement between the acquisitions of different b-values. Both readers visually analyzed all DW images in consensus concerning lesion displacement between the b50 and b400 and the b400 and b800 images ([Fig. 1]). If there was lesion displacement between the b50 and b400 images, no ADC map was calculated. Otherwise, an ADC map was calculated on the basis of the b50 and b400 images (ADC400 and ADC400CM). If there was no lesion displacement between the b400 and b800 sequence, an ADC map was calculated on the basis of the b50, b400 and b800 images (ADC800 and ADC800CM). In this subgroup all lesions had four ADC values (ADC400 ± CM and ADC800 ± CM; [Fig. 2]). The ADC map was calculated with the scanner software using a monoexponential fit. To obtain the ADC value of a lesion, it was first located in the subtractions of the dynamic protocol and then identified in the diffusion-weighted images, where a region of interest (ROI) was drawn and copied to the ADC map. The ROI was drawn into the most homogeneous area of the lesion. In centrally necrotic lesions the ROI was drawn in the CM-enhancing rim. Histology was obtained by core needle or surgical biopsy.

Abb. 1 42-jährige Patientin mit einem 1 cm großen invasiv-duktalen Karzinom in der linken Brust. In der frühen Subtraktionsaufnahme der dynamischen Serie erkennbare, umschriebene Läsion mit KM-Aufnahme (schwarzer Stern, a). In der gleichen Schicht findet sich ein Fokus von 4 mm (Pfeilspitze). In den diffusionsgewichteten Bildern mit den b-Werten 50 und 400 ist die Läsion scharf abgrenzbar (schwarzer Stern, b und c). Bei der b800 Messung ist die Läsion in anterior/posterior Richtung verschoben (weiße Pfeile, d). Auf der ADC-Karte, berechnet auf Basis der b50 / b400 Messungen ist die Läsion homogen hypointens (weißer Stern, e). In der ADC Karte basierend auf der b50-/ b400-/b800-Messung führt die Verschiebung der Läsion bei der b800 Messung zu einem hyperintensem Rand (weiße Pfeilspitzen, f), der den ADC-Wert verfälschen kann.
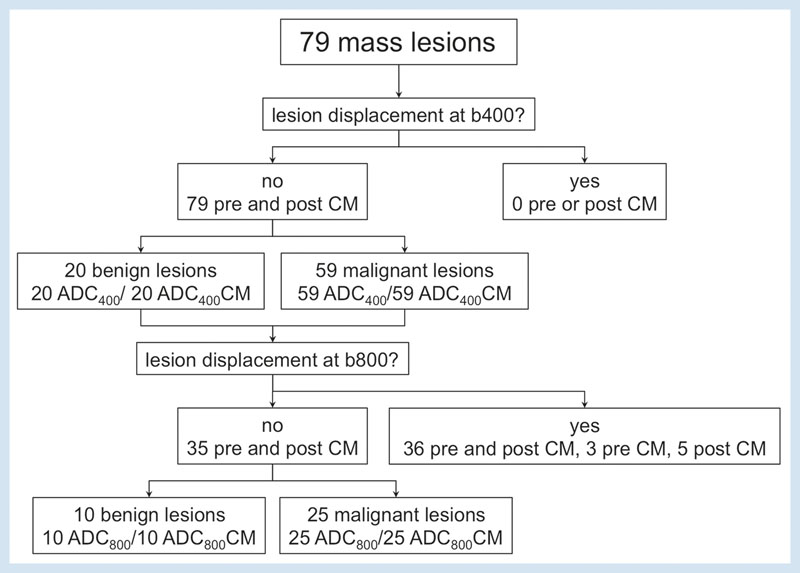
Abb. 2 Ergebnis der Analyse der Läsionsverschiebung zwischen der b50- und b400-Messung und der b400- and b800-Messung. In dem Fall eines Versatzes der Läsion zwischen der b50- and b400-Messung wurde keine ADC-Karte berechnet. Andernfalls wurde eine ADC-Karte auf Basis der b50- and b400-Bilder berechnet (ADC400 and ADC400CM). Bei fehlendem Versatz der Läsion zwischen der b400- and b800-Messung wurde zusätzlich eine AC-Karte auf Basis der b50-, b400- and b800-Bilder berechnet (ADC800 and ADC800CM). In dieser Untergruppe hatten alle Läsionen vier ADC-Werte (ADC400 ± CM and ADC800 ± CM). CM = Kontrastmittel.
Statistical analysis
Differences in patient characteristics were calculated with the Student’s t-test. The mean value and standard deviation of all ADC values of the benign and malignant lesions pre- and post-CM application were calculated and the highest and lowest values were indicated. The mean ADC value of all benign and malignant lesions pre- and post-CM (ADC400 vs. ADC400CM and ADC800 vs. ADC800CM) was compared using the Student’s t-test. In the subgroup with no lesion displacement between the b50, b400 and b800 measurement, the ADC400 value was compared with the ADC800 value in the same group (benign pre-CM, benign post-CM, malignant pre-CM and malignant post-CM) using the paired t-test. All statistics were calculated with SPSS 19.0® (Chicago, Illinois, USA). A p-value < 0.05 was considered significant.
Results
163/286 women with breast MRI exams and DW sequences had no suspicious MR finding. 63/123 patients had enhancing lesions smaller than 6 mm (foci) or non-mass-enhancing lesions in contrast-enhanced MRI and so did not meet the inclusion criteria.
Hence, 60/123 women (mean age, 50 years; range, 39 – 61 years) with 79 mass lesions in the T1w dynamic sequence were included in the study. The mean lesion size was 1.5 ± 0.8 cm.
Histology revealed a benign result in 20 lesions (13 fibroadenomas, 5 areas of fibrocystic disease and one case of a sclerosing adenosis and a focal scar each). A malignant histology was found in 59 lesions (33 purely invasive ductal carcinomas, 16 invasive ductal carcinomas with intraductal carcinoma in situ (DCIS), 3 pure DCIS, 2 recurrent invasive ductal carcinomas, 3 invasive lobular carcinomas, and 2 mucinous carcinomas). The benign lesions had a mean size of 1.2 ± 0.5 cm, and the malignant lesions had a mean size of 1.6 ± 0.8 cm.
Analyzing the diffusion-weighted images, there was no lesion displacement between the b50 and the b400 measurements. Therefore, ADC values were calculated for all 79 lesions with the b50 and b400 measurements.
Significant lesion displacement occurred between the b400 and b800 measurements in 39 lesions (10 benign, 29 malignant including 2 mucinous carcinomas) before contrast media (CM) application and in 41 after CM application (9 benign, 32 malignant including 2 mucinous carcinomas). In 3 lesions there was only displacement pre-CM and in 5 lesions only post-CM. In 36 lesions the readers found lesion displacement pre- and post-CM ([Fig. 2]). In 35 lesions (10 benign, 25 malignant), sequence acquisition with all three b-values was possible before and after CM without lesion displacement. Therefore, pair-wise comparison of the ADC values based on all DW measurements was possible in these 35 lesions ([Fig. 2]).
Analyzing the ADC400 values, the mean ADC value of all 20 benign lesions was 1.89 × 10-3 mm2/s before and 1.85 × 10-3 mm2/s after CM administration. Two malignant lesions were mucinous carcinomas. These lesions revealed an ADC value of 1.74 and 2.03 × 10-3 mm2/s before CM application and 1.75 and 1.86 × 10-3 mm2/s after CM application. The remaining 57 malignant lesions exhibited a mean ADC value of 1.00 × 10-3 mm2/s prior to and 0.88 × 10-3 mm2/s after CM.
In the subgroup without lesion displacement between the b400 and b800 acquisition, the mean ADC value of benign lesions (n = 10) was 1.99 × 10-3 mm2/s before and 1.97 × 10-3 mm2/s after CM application. The 25 malignant lesions in this subgroup exhibited a mean ADC value of 0.90 × 10-3 mm2/s prior to and 0.80 × 10-3 mm2/s after CM ([Table 1, ] [Fig. 3]).

Abb. 3 ADC-Werte der gutartigen (weiß) und bösartigen (grau) Läsionen vor und nach KM-Gabe, berechnet auf Basis der b50-/ b400- und der b50-/ b400-/b800-Messungen. Die Rauten zeigen den höchsten und niedrigsten ADC-Wert, der schwarze Strich den durchschnittlichen ADC-Wert. Die Kreise repräsentieren die ADC-Werte der muzinösen Karzinome.
While there is no significant change for benign lesions, the CM administration resulted in a highly significant (p < 0.01) decrease of the ADC value in malignant lesions in both groups (ADC400 and ADC800).
If there was no lesion displacement between the b400 and b800 measurement (35 lesions, 10 benign and 25 malignant), the ADC value was calculated on the basis of the b50, b400 measurement and on the basis of the b50, b400 and b800 measurement pre- and post-CM application. Therefore, a pair-wise comparison of these ADC values was possible. The mean ADC value obtained for the benign lesions was 1.98 × 10-3 mm2/s in both b-value combinations, while for malignant lesions the ADC value was 0.91 × 10-3 mm2/s calculated on the basis of b50 and b400 compared to 0.85 × 10-3 mm2/s calculated on the basis of b50, b400 and b800. This difference was highly significant (p < 0.01).
Discussion
According to our results, diffusion-weighted MR imaging of the breast is feasible after contrast media (CM) application using spectral fat saturation. The average ADC values decreased after CM application in benign and malignant lesions. This is in agreement with our preliminary results [18]. However, in benign lesions this decrease was not significant. Yuen et al. also found a decrease of the ADC value after CM application in 19 breast carcinomas [19]. In contrast to our study, Yuen et al. did not have benign lesions as a control group. There are some studies dealing with the influence of CM on the ADC value of normal brain tissue and infarcts. Yamada et al. found a significant decrease of the ADC value after CM administration [20], while there was no difference in the study of Fitzek et al. [21]. In the study of Yamada et al., DWI was obtained immediately after CM application, while there was a longer time interval in the study of Fitzek et al. Firat et al. combined both protocols and found a significant decrease of the ADC value of normal brain tissue and infarct immediately after CM application which normalized in the late post-contrast DW images [22]. They explained this phenomenon as an effect of the intravascular CM on the diffusion-weighted images. In their study meningiomas which are highly vascularized revealed the highest decrease of the ADC value immediately after CM application. The mechanism of the effect of CM on the ADC value is not yet understood. Yuen et al. supposed a decrease of microperfusion due to CM which leads to a drop of the ADC value in regions with a high content of microvessels like in malignant breast tumors [19]. In our study we used b50 as the lowest b-value in order to reduce the effect of macroperfusion on the ADC value. However, the effect of microperfusion is still present. In a comment on the article by Yuen, Ramadan and Mulkern wrote that “Gd contrast alters the local magnetic susceptibilities within specific tissue compartments, which in turn produce background magnetic field gradients that can add to, or detract from, diffusion sensitization gradients and subsequently alter measured diffusion coefficients” [23]. Clearly, further experiments are required to investigate the origin of the observed effect. Due to the heterogeneous nature and wide variety of breast lesions, a comprehensive study would require a very rigid design and quantitative analysis of e. g. the amount of residual contrast agent at the time of DWI acquisition and its potential dependency on the relaxivity of different agents, which was beyond the scope of this study.
For the discrimination of benign and malignant lesions, the difference between the highest ADC value in malignant lesions and the lowest ADC value of the benign lesions is of special interest. In our study this difference was nearly identical pre- and post-contrast when calculating the ADC value on the basis of the b50 and b400 images (0.18 × 10-3 mm2/s pre-CM and 0.15 × 10-3 mm2/s pos- CM) but increased using b50, b400 and b800 for calculating the ADC map (0.29 × 10-3 mm2/s pre-CM and 0.53 × 10-3 mm2/s post-CM).
In our study mucinous carcinomas behaved differently from other carcinomas regarding the ADC value. Woodhams et al. measured higher ADC values in mucinous carcinomas in comparison to other malignant lesions. In their study pure mucinous carcinomas had even higher ADC values than the majority of benign lesions [24]. In our study both pure type mucinous carcinomas revealed ADC values not noticeably different from benign lesions ([Fig. 3]).
Excluding mucinous carcinomas, the ADC values of benign and malignant lesions had no overlap pre- or post-CM in our study, which is slightly better than in other published studies [10] [11] [12] [25] [26] [27] [28]. This positive result might be stochastic due to the small population number or a consequence of the inclusion criteria. However, it can also be due to the strict analysis of the DW images concerning the lesion location. If there is even a minor lesion displacement that affects the selected ROI, the calculated ADC maps may result in incorrect ADC values. This led to a dropout of nearly 50 % of all measurements with a b-value of 800 s/mm². Interestingly this phenomenon is not often reported in prior studies. Partridge et al. had a dropout of 11 % of all lesions using b-values of 0 and 600 s/mm² [26]. In our study movement of the lesion occurred exclusively in the anterior posterior position (which was the phase encoding direction) and all lesions moved towards the nipple. One possible explanation for that phenomenon could be a relaxation of the pectoral muscle during the sequence, patient motion or cardiac motion. All of them induce phase shifts, which increase with the strength of the gradient pulses [29]. In 3 lesions, displacement occurred only during pre-CM and in 5 lesions only during post-CM imaging. In these cases relaxation of the pectoral muscle or patient movement is the most likely explanation for lesion displacement. In the remaining 36 lesions with lesion displacement, eddy currents or cardiac motion might be the most likely explanation. Eddy currents are induced when strong gradient pulses are switched rapidly. This can lead to image distortion (contraction, shift, rotation and shear) in the phase encoding direction [29]. For that reason the acquisition of 3 b-values could be helpful to get an evaluable measurement, at least with the 2 lower b-values. It is noteworthy that the contribution of eddy currents is spatially dependent with a stronger effect further away from the isocenter. This might be the reason why this effect is not observed consistently despite the fact that the sequence parameters were kept constant.
During the recruitment for this study, a new technique was introduced as part of the DW-EPI acquisition, which accounts for such potential distortions between the diffusion images. This algorithm performs a registration of the b-value images onto each other (Dynamic Field Correction, DFC) and has been implemented on the recent scanner software versions. An initial study on the performance of this correction can be found in [30].
In international standards for breast MR imaging, a dynamic contrast-enhanced sequence and a T2-weighted sequence are recommended [31] [32]. Up to now, DWI is an add-on, which may help to increase the specificity of breast lesions in some cases. As DWI is an add-on, it makes sense to acquire this add-on at the end of the measurement.
Although we had no overlap of ADC values of benign and malignant lesions, we would not recommend a threshold of approximately 1.4 × 10-3 mm2/s which exactly separates the benign from the malignant lesions in our study ([Fig. 3]). The intention of breast MRI is to identify malignant lesions with a high sensitivity with an acceptable amount of false-positive results. For that reason an adequate threshold could be the average ADC value of malignant lesions plus three times the standard deviation, which should find 99 % of all malignant lesions [13]. In our study this threshold would be about 1.5 × 10-3 mm2/s. Excluding the mucinous carcinomas, this threshold would lead to a sensitivity of 100 % and two false-positive lesions with a specificity of 89 % pre- and post-CM. The positive predictive value of an ADC threshold lower than 1.5 × 10-3 mm2/s would be 97 %.
Our study faces some limitations that suggest directions for future work. The small number of lesions, especially those with benign histology, may have influenced the statistical results. Our DWI protocol was measured with 3-scan trace and 2 averages. This resulted in 6 measurements which lead to a diminished signal-to-noise ratio. After the study we doubled the number of measurements to increase image quality.
In summary DWI of the breast is possible before and after CM application. In our evaluation setting, the indication for DW sequences is further characterization of contrast-enhancing lesions. Therefore, DW sequences can be applied after detecting suspicious lesions in the dynamic sequence. Our data even suggest a slightly better discrimination of benign and malignant lesions with DW imaging after CM. However, higher patient numbers need to be investigated in order to verify this.
-
References
- 1 Benndorf M, Baltzer PA, Vag T et al. Acta Radiol. 2010; 51: 715-721
- 2 Mahoney MC, Gatsonis C, Hanna L et al. Radiology. 2012; 264: 51-58
- 3 Bick U, Engelken F, Diederichs G et al. MRI of the Breast as Part of the Assessment in Population-Based Mammography Screening. Fortschr Röntgenstr 2013; [Epub ahead of print]
- 4 Siegmann KC, Moron HU, Baur A et al. Diagnostic value of a breast MRI score for the prediction of malignancy of breast lesions detected solely with MRI. Fortschr Röntgenstr 2009; 181: 556-563
- 5 Dietzel M, Baltzer PA, Vag T et al. Magnetic resonance mammography in small vs. advanced breast lesions – systematic comparison reveals significant impact of lesion size on diagnostic accuracy in 936 histologically verified breast lesions. Fortschr Röntgenstr 2011; 183: 126-135
- 6 Kul S, Cansu A, Alhan E et al. Contribution of diffusion-weighted imaging to dynamic contrast-enhanced MRI in the characterization of breast tumors. Am J Roentgenol Am J Roentgenol 2011; 196: 210-217
- 7 Partridge SC, Mullins CD, Kurland BF et al. Apparent diffusion coefficient values for discriminating benign and malignant breast MRI lesions: effects of lesion type and size. Am J Roentgenol Am J Roentgenol 2010; 194: 1664-1673
- 8 Pinker K, Bickel H, Helbich TH et al. Combined contrast-enhanced magnetic resonance and diffusion-weighted imaging reading adapted to the “Breast Imaging Reporting and Data System” for multiparametric 3-T imaging of breast lesions. Eur Radiol 2013; [Epub ahead of print]
- 9 Baltzer PA, Benndorf M, Dietzel M et al. Sensitivity and specificity of unenhanced MR mammography (DWI combined with T2-weighted TSE imaging, ueMRM) for the differentiation of mass lesions. Eur Radiol 2010; 20: 1101-1110
- 10 Guo Y, Cai YQ, Cai ZL et al. Differentiation of clinically benign and malignant breast lesions using diffusion-weighted imaging. J Magn Reson Imaging 2002; 16: 172-178
- 11 Rubesova E, Grell AS, De Maertelaer V et al. Quantitative diffusion imaging in breast cancer: a clinical prospective study. J Magn Reson Imaging 2006; 24: 319-324
- 12 Sinha S, Lucas-Quesada FA, Sinha U et al. In vivo diffusion-weighted MRI of the breast: potential for lesion characterization. J Magn Reson Imaging 2002; 15: 693-704
- 13 Wenkel E, Geppert C, Schulz-Wendtland R et al. Diffusion weighted imaging in breast MRI: comparison of two different pulse sequences. Acad Radiol 2007; 14: 1077-1083
- 14 Yabuuchi H, Matsuo Y, Okafuji T et al. Enhanced mass on contrast-enhanced breast MR imaging: Lesion characterization using combination of dynamic contrast-enhanced and diffusion-weighted MR images. J Magn Reson Imaging 2008; 28: 1157-1165
- 15 Pickles MD, Gibbs P, Lowry M et al. Diffusion changes precede size reduction in neoadjuvant treatment of breast cancer. Magn Reson Imaging 2006; 24: 843-847
- 16 Yankeelov TE, Lepage M, Chakravarthy A et al. Integration of quantitative DCE-MRI and ADC mapping to monitor treatment response in human breast cancer: initial results. Magn Reson Imaging 2007; 25: 1-13
- 17 Tsushima Y, Takahashi-Taketomi A, Endo K. Magnetic resonance (MR) differential diagnosis of breast tumors using apparent diffusion coefficient (ADC) on 1.5-T. J Magn Reson Imaging 2009; 30: 249-255
- 18 Geppert C, Wenkel E, Bautz W et al. Enhanced lesion discrimination in breast DWI after contrast administration. Proceedings of the 16th Annual Meeting of ISMRM Toronto: 2008
- 19 Yuen S, Yamada K, Goto M et al. Microperfusion-induced elevation of ADC is suppressed after contrast in breast carcinoma. J Magn Reson Imaging 2009; 29: 1080-1084
- 20 Yamada K, Kubota H, Kizu O et al. Effect of intravenous gadolinium-DTPA on diffusion-weighted images: evaluation of normal brain and infarcts. Stroke 2002; 33: 1799-1802
- 21 Fitzek C, Mentzel HJ, Fitzek S et al. Echoplanar diffusion-weighted MRI with intravenous gadolinium-DTPA. Neuroradiology 2003; 45: 592-597
- 22 Firat AK, Sanli B, Karakas HM et al. The effect of intravenous gadolinium-DTPA on diffusion-weighted imaging. Neuroradiology 2006; 48: 465-470
- 23 Ramadan S, Mulkern RV. Comment on ADC reductions in postcontrast breast tumors. J Magn Reson Imaging 2010; 31: 262 ; author reply 263–264
- 24 Woodhams R, Kakita S, Hata H et al. Diffusion-weighted imaging of mucinous carcinoma of the breast: evaluation of apparent diffusion coefficient and signal intensity in correlation with histologic findings. Am J Roentgenol Am J Roentgenol 2009; 193: 260-266
- 25 Hatakenaka M, Soeda H, Yabuuchi H et al. Apparent diffusion coefficients of breast tumors: clinical application. Magn Reson Med Sci 2008; 7: 23-29
- 26 Partridge SC, DeMartini WB, Kurland BF et al. Quantitative diffusion-weighted imaging as an adjunct to conventional breast MRI for improved positive predictive value. Am J Roentgenol Am J Roentgenol 2009; 193: 1716-1722
- 27 Woodhams R, Matsunaga K, Iwabuchi K et al. Diffusion-weighted imaging of malignant breast tumors: the usefulness of apparent diffusion coefficient (ADC) value and ADC map for the detection of malignant breast tumors and evaluation of cancer extension. J Comput Assist Tomogr 2005; 29: 644-649
- 28 Woodhams R, Matsunaga K, Kan S et al. ADC mapping of benign and malignant breast tumors. Magn Reson Med Sci 2005; 4: 35-42
- 29 Le Bihan D, Poupon C, Amadon A et al. Artifacts and pitfalls in diffusion MRI. J Magn Reson Imaging 2006; 24: 478-488
- 30 Geppert C, Feiweiher T, Janka R et al. Reduction of image distortions in breast DWI using dynamic field correction: impact on ADC assessment. Proceedings of the Annual Meeting of ESMRMB. Leipzig: 2011
- 31 ACR Practice Guideline for the Performance of Contrast-Enhanced Magnetic Resonance Imaging (MRI) of the Breast Res. 25 ed. 2008
- 32 Mann RM, Kuhl CK, Kinkel K et al. Breast MRI: guidelines from the European Society of Breast Imaging. Eur Radiol 2008; 18: 1307-1318
Correspondence
-
References
- 1 Benndorf M, Baltzer PA, Vag T et al. Acta Radiol. 2010; 51: 715-721
- 2 Mahoney MC, Gatsonis C, Hanna L et al. Radiology. 2012; 264: 51-58
- 3 Bick U, Engelken F, Diederichs G et al. MRI of the Breast as Part of the Assessment in Population-Based Mammography Screening. Fortschr Röntgenstr 2013; [Epub ahead of print]
- 4 Siegmann KC, Moron HU, Baur A et al. Diagnostic value of a breast MRI score for the prediction of malignancy of breast lesions detected solely with MRI. Fortschr Röntgenstr 2009; 181: 556-563
- 5 Dietzel M, Baltzer PA, Vag T et al. Magnetic resonance mammography in small vs. advanced breast lesions – systematic comparison reveals significant impact of lesion size on diagnostic accuracy in 936 histologically verified breast lesions. Fortschr Röntgenstr 2011; 183: 126-135
- 6 Kul S, Cansu A, Alhan E et al. Contribution of diffusion-weighted imaging to dynamic contrast-enhanced MRI in the characterization of breast tumors. Am J Roentgenol Am J Roentgenol 2011; 196: 210-217
- 7 Partridge SC, Mullins CD, Kurland BF et al. Apparent diffusion coefficient values for discriminating benign and malignant breast MRI lesions: effects of lesion type and size. Am J Roentgenol Am J Roentgenol 2010; 194: 1664-1673
- 8 Pinker K, Bickel H, Helbich TH et al. Combined contrast-enhanced magnetic resonance and diffusion-weighted imaging reading adapted to the “Breast Imaging Reporting and Data System” for multiparametric 3-T imaging of breast lesions. Eur Radiol 2013; [Epub ahead of print]
- 9 Baltzer PA, Benndorf M, Dietzel M et al. Sensitivity and specificity of unenhanced MR mammography (DWI combined with T2-weighted TSE imaging, ueMRM) for the differentiation of mass lesions. Eur Radiol 2010; 20: 1101-1110
- 10 Guo Y, Cai YQ, Cai ZL et al. Differentiation of clinically benign and malignant breast lesions using diffusion-weighted imaging. J Magn Reson Imaging 2002; 16: 172-178
- 11 Rubesova E, Grell AS, De Maertelaer V et al. Quantitative diffusion imaging in breast cancer: a clinical prospective study. J Magn Reson Imaging 2006; 24: 319-324
- 12 Sinha S, Lucas-Quesada FA, Sinha U et al. In vivo diffusion-weighted MRI of the breast: potential for lesion characterization. J Magn Reson Imaging 2002; 15: 693-704
- 13 Wenkel E, Geppert C, Schulz-Wendtland R et al. Diffusion weighted imaging in breast MRI: comparison of two different pulse sequences. Acad Radiol 2007; 14: 1077-1083
- 14 Yabuuchi H, Matsuo Y, Okafuji T et al. Enhanced mass on contrast-enhanced breast MR imaging: Lesion characterization using combination of dynamic contrast-enhanced and diffusion-weighted MR images. J Magn Reson Imaging 2008; 28: 1157-1165
- 15 Pickles MD, Gibbs P, Lowry M et al. Diffusion changes precede size reduction in neoadjuvant treatment of breast cancer. Magn Reson Imaging 2006; 24: 843-847
- 16 Yankeelov TE, Lepage M, Chakravarthy A et al. Integration of quantitative DCE-MRI and ADC mapping to monitor treatment response in human breast cancer: initial results. Magn Reson Imaging 2007; 25: 1-13
- 17 Tsushima Y, Takahashi-Taketomi A, Endo K. Magnetic resonance (MR) differential diagnosis of breast tumors using apparent diffusion coefficient (ADC) on 1.5-T. J Magn Reson Imaging 2009; 30: 249-255
- 18 Geppert C, Wenkel E, Bautz W et al. Enhanced lesion discrimination in breast DWI after contrast administration. Proceedings of the 16th Annual Meeting of ISMRM Toronto: 2008
- 19 Yuen S, Yamada K, Goto M et al. Microperfusion-induced elevation of ADC is suppressed after contrast in breast carcinoma. J Magn Reson Imaging 2009; 29: 1080-1084
- 20 Yamada K, Kubota H, Kizu O et al. Effect of intravenous gadolinium-DTPA on diffusion-weighted images: evaluation of normal brain and infarcts. Stroke 2002; 33: 1799-1802
- 21 Fitzek C, Mentzel HJ, Fitzek S et al. Echoplanar diffusion-weighted MRI with intravenous gadolinium-DTPA. Neuroradiology 2003; 45: 592-597
- 22 Firat AK, Sanli B, Karakas HM et al. The effect of intravenous gadolinium-DTPA on diffusion-weighted imaging. Neuroradiology 2006; 48: 465-470
- 23 Ramadan S, Mulkern RV. Comment on ADC reductions in postcontrast breast tumors. J Magn Reson Imaging 2010; 31: 262 ; author reply 263–264
- 24 Woodhams R, Kakita S, Hata H et al. Diffusion-weighted imaging of mucinous carcinoma of the breast: evaluation of apparent diffusion coefficient and signal intensity in correlation with histologic findings. Am J Roentgenol Am J Roentgenol 2009; 193: 260-266
- 25 Hatakenaka M, Soeda H, Yabuuchi H et al. Apparent diffusion coefficients of breast tumors: clinical application. Magn Reson Med Sci 2008; 7: 23-29
- 26 Partridge SC, DeMartini WB, Kurland BF et al. Quantitative diffusion-weighted imaging as an adjunct to conventional breast MRI for improved positive predictive value. Am J Roentgenol Am J Roentgenol 2009; 193: 1716-1722
- 27 Woodhams R, Matsunaga K, Iwabuchi K et al. Diffusion-weighted imaging of malignant breast tumors: the usefulness of apparent diffusion coefficient (ADC) value and ADC map for the detection of malignant breast tumors and evaluation of cancer extension. J Comput Assist Tomogr 2005; 29: 644-649
- 28 Woodhams R, Matsunaga K, Kan S et al. ADC mapping of benign and malignant breast tumors. Magn Reson Med Sci 2005; 4: 35-42
- 29 Le Bihan D, Poupon C, Amadon A et al. Artifacts and pitfalls in diffusion MRI. J Magn Reson Imaging 2006; 24: 478-488
- 30 Geppert C, Feiweiher T, Janka R et al. Reduction of image distortions in breast DWI using dynamic field correction: impact on ADC assessment. Proceedings of the Annual Meeting of ESMRMB. Leipzig: 2011
- 31 ACR Practice Guideline for the Performance of Contrast-Enhanced Magnetic Resonance Imaging (MRI) of the Breast Res. 25 ed. 2008
- 32 Mann RM, Kuhl CK, Kinkel K et al. Breast MRI: guidelines from the European Society of Breast Imaging. Eur Radiol 2008; 18: 1307-1318
Abb. 1 42-jährige Patientin mit einem 1 cm großen invasiv-duktalen Karzinom in der linken Brust. In der frühen Subtraktionsaufnahme der dynamischen Serie erkennbare, umschriebene Läsion mit KM-Aufnahme (schwarzer Stern, a). In der gleichen Schicht findet sich ein Fokus von 4 mm (Pfeilspitze). In den diffusionsgewichteten Bildern mit den b-Werten 50 und 400 ist die Läsion scharf abgrenzbar (schwarzer Stern, b und c). Bei der b800 Messung ist die Läsion in anterior/posterior Richtung verschoben (weiße Pfeile, d). Auf der ADC-Karte, berechnet auf Basis der b50 / b400 Messungen ist die Läsion homogen hypointens (weißer Stern, e). In der ADC Karte basierend auf der b50-/ b400-/b800-Messung führt die Verschiebung der Läsion bei der b800 Messung zu einem hyperintensem Rand (weiße Pfeilspitzen, f), der den ADC-Wert verfälschen kann.
Abb. 2 Ergebnis der Analyse der Läsionsverschiebung zwischen der b50- und b400-Messung und der b400- and b800-Messung. In dem Fall eines Versatzes der Läsion zwischen der b50- and b400-Messung wurde keine ADC-Karte berechnet. Andernfalls wurde eine ADC-Karte auf Basis der b50- and b400-Bilder berechnet (ADC400 and ADC400CM). Bei fehlendem Versatz der Läsion zwischen der b400- and b800-Messung wurde zusätzlich eine AC-Karte auf Basis der b50-, b400- and b800-Bilder berechnet (ADC800 and ADC800CM). In dieser Untergruppe hatten alle Läsionen vier ADC-Werte (ADC400 ± CM and ADC800 ± CM). CM = Kontrastmittel.
Abb. 3 ADC-Werte der gutartigen (weiß) und bösartigen (grau) Läsionen vor und nach KM-Gabe, berechnet auf Basis der b50-/ b400- und der b50-/ b400-/b800-Messungen. Die Rauten zeigen den höchsten und niedrigsten ADC-Wert, der schwarze Strich den durchschnittlichen ADC-Wert. Die Kreise repräsentieren die ADC-Werte der muzinösen Karzinome.