

Subscribe to RSS
DOI: 10.5999/aps.2015.42.5.642
Capsular Contracture after Calf Augmentation with Silicone Implant Insertion
Authors
The legs are an aesthetically important part of the body, and an increasing number of patients desire calf-contouring procedures to improve the overall appearance of their legs. At one end of the spectrum, botulinum toxin injections are used to reduce the volume of hypertrophic calf muscles, and at the other end, silicone implants or autologous fat may be used to add volume. The shape of the calf is determined by a number of factors: the soleus and gastrocnemius musculature, the length and orientation of the bones, and the distribution of subcutaneous fat. Since Carlsen first performed calf augmentation with carved silastic foam implants inserted beneath the deep fascia of the calf in 1972, various methods of inserting silicone gel-filled implants and silicone rubber implants have been reported [[1]]. Inserting silicone implants into the calf has disadvantages; early postoperative complications include hematoma, seroma, wound disruption and infection, and later complications include capsular contracture, extrusion, rupture, and palpability. However, it is generally a safe procedure with a low incidence of complications [[2]]. Given the infrequent occurrence of complications, it is not surprising that few reports containing radiological or pathological images documenting capsular contracture have been published [[3]].
A 50-year-old female presented with a palpable hard implant in her left calf ([Fig. 1]). She complained of discomfort during walking. She had undergone calf augmentation surgery 20 years previously in the United Kingdom. No information was available about the type of implant or the plane of insertion. Physical examination revealed a firm, visible, and immobile implant in the posteromedial aspect of the left calf. No signs of inflammation were noted. A horizontal scar 4 cm in length was observed in the popliteal crease. Magnetic resonance imaging (MRI) was performed to assess the plane of insertion and to check for rupture. The implant was located beneath the deep fascia of the lower leg, at the medial aspect of the medial gastrocnemius muscle. High signal intensity in T2-weighted images and low signal intensity in T1-weighted images were observed. The implant was surrounded by a 3-mm layer of fibrotic or calcified tissue with low intensity in both T1- and T2-weighted images ([Fig. 2]).


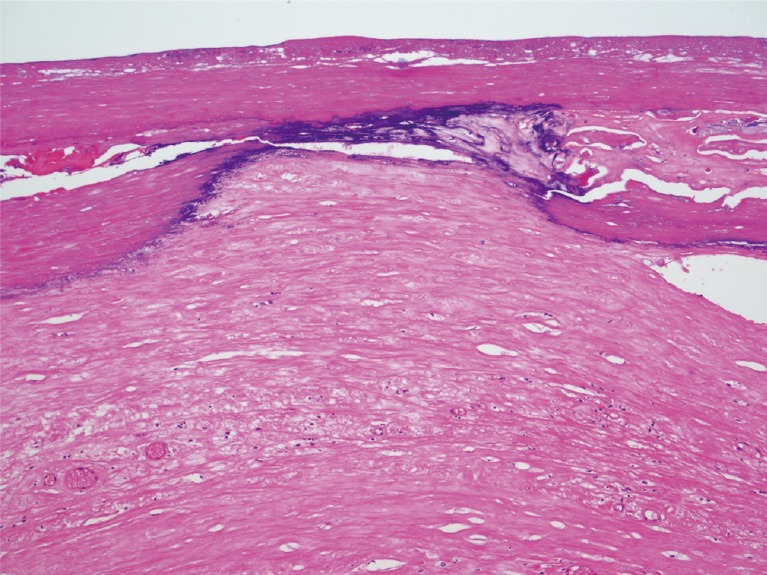
The patient did not desire reinsertion, and preferred to leave her right calf implant inserted. Therefore, we planned to remove the left implant with simultaneous capsulotomy or capsulectomy. Under general anesthesia, a 4-cm incision was made along the scar from the previous operation. Dissection was performed through the subcutaneous adipose tissue until the deep fascia was reached. An incision was made in the fascia to expose a thick, calcified capsule. This capsule was incised and an intact, lenticular-shaped, solid silicone implant 5 cm in width and 13 cm in length was exposed. No signs of extracapsular rupture were noted, and the implant was extracted. Since the capsule was very thick and severely calcified, we performed a capsulectomy ([Fig. 3]). The capsule was 3.2 mm thick on average and had multiple calcified nodules. Histopathological analysis revealed a thick layer of wavy collagen bundles with focal calcifications ([Fig. 4]). An additional incision was made at the distal end of the capsule to facilitate removal. A negative suction drain was inserted into the subfascial space, and the incision was closed layer by layer. The drain was removed two days after surgery, and the patient's leg healed well without any incidence of hematoma, seroma, infection, or sensory loss ([Fig. 5]). Ambulation was restricted to minimal movement for one week.


Calf augmentation using silicone implants is a relatively safe, reproducible procedure with a low reported incidence of complications. However, as with silicone implants inserted into the breast, implant palpability, asymmetry, rupture, extrusion, infection, or capsular contracture may occur [[4]]. Capsular contracture in the calf has been reported to have an incidence of approximately 3% to 4% [[2]]. The contracture rates are higher when implants are placed in subcutaneous pockets compared to subfascial pockets, submuscular pockets, or supraperiosteal pockets [[2]]. While a diverse range of implant types, including silastic foam, gel-filled silicone, solid silicone, and cohesive silicone gel with soft silicone rubber have been used, no studies have compared the risk of capsular contracture depending on the implant type [[2]].
The mechanism of capsular contracture in breast augmentation has been the focus of much attention, but has yet to be fully elucidated. The subclinical infection hypothesis has led surgeons to use caution when manipulating any implant, and some recommend povidone-iodine irrigation of the pocket. Others have proposed that capsular contracture is a result of cystic fibrosis, or a form of hypertrophic scar tissue [[5]]. Smoking has been found to be a major risk factor, and is a relative contraindication to augmentation. Capsular contracture in calf augmentation may differ from contracture in breast augmentation because calf implants are not exposed to any ductal tissue or endogenous flora; however, further studies are necessary to evaluate this possibility.
While capsular contracture may be estimated in a clinical evaluation, imaging modalities may aid in the diagnosis. The radiological findings associated with silicone implants and subsequent complications have been extensively described for breast augmentation [[3]]. Plain X-rays may reveal the calcified outline of the capsule but are otherwise unrevealing. Ultrasonography, computed tomography, or MRI may show a thickened fibrous capsule. Zahavi et al. [[5]] have reported that greater capsule thickness observed in ultrasonography or MRI findings of the breast correlates with more severe capsular contracture. Capsule thickness averaging 1.39 mm on MRI correlates with a low degree of contracture severity, corresponding to a clinical Baker score of I or II, while capsules averaging 2.62 mm in thickness correlate with a higher degree of contracture, corresponding to a clinical Baker score of III or IV. The same correlation was found in ultrasonography at the thickness levels of 1.14 mm and 2.39 mm, respectively. They suggested a cutoff value of 2 mm to discriminate between thin and thick capsules.
Treatment consists of removing the implant, capsulectomy or capsulotomy, and drain placement. As in capsular contracture of the breast, a new pocket may be formed and implants may be inserted into this neopocket. However, no grading system exists for capsular contracture of the calf, and no standardized indications exist for surgery. Of course, any clinical signs of infection, pain, discomfort, malposition, or implant extrusion will inevitably require surgical removal. Otherwise, the surgeon and patient must contemplate the benefits and disadvantages before deciding on whether and when to intervene.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
-
References
- 1 Niechajev I. Calf augmentation and restoration. Plast Reconstr Surg 2005; 116: 295-305
- 2 Flores-Lima G, Eppley BL. Body contouring with solid silicone implants. Aesthetic Plast Surg 2009; 33: 140-146
- 3 Duryea D, Petscavage-Thomas J, Frauenhoffer EE. et al. Linguine sign in musculoskeletal imaging: calf silicone implant rupture. Skeletal Radiol 2015; 44: 1157-1160
- 4 de la Pena-Salcedo JA, Soto-Miranda MA, Lopez-Salguero JF. Calf implants: a 25-year experience and an anatomical review. Aesthetic Plast Surg 2012; 36: 261-270
- 5 Zahavi A, Sklair ML, Ad-El DD. Capsular contracture of the breast: working towards a better classification using clinical and radiologic assessment. Ann Plast Surg 2006; 57: 248-251
Correspondence
Publication History
Received: 11 March 2015
Accepted: 09 June 2015
Article published online:
05 May 2022
© 2015. The Korean Society of Plastic and Reconstructive Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonCommercial License, permitting unrestricted noncommercial use, distribution, and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes. (https://creativecommons.org/licenses/by-nc/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Niechajev I. Calf augmentation and restoration. Plast Reconstr Surg 2005; 116: 295-305
- 2 Flores-Lima G, Eppley BL. Body contouring with solid silicone implants. Aesthetic Plast Surg 2009; 33: 140-146
- 3 Duryea D, Petscavage-Thomas J, Frauenhoffer EE. et al. Linguine sign in musculoskeletal imaging: calf silicone implant rupture. Skeletal Radiol 2015; 44: 1157-1160
- 4 de la Pena-Salcedo JA, Soto-Miranda MA, Lopez-Salguero JF. Calf implants: a 25-year experience and an anatomical review. Aesthetic Plast Surg 2012; 36: 261-270
- 5 Zahavi A, Sklair ML, Ad-El DD. Capsular contracture of the breast: working towards a better classification using clinical and radiologic assessment. Ann Plast Surg 2006; 57: 248-251