
RSS-Feed abonnieren
DOI: 10.5999/aps.2015.42.5.552
Clinical Experience of the Klippel-Trenaunay Syndrome
Background The Klippel-Trenaunay syndrome (KTS) is characterized by three clinical features, namely cutaneous capillary malformations, venous malformations, and soft tissue and/or bony hypertrophy of the extremities. The varied manifestations are attributed to the unpredictable clinical nature and prognosis of the syndrome. To elucidate the clinical characteristics of this disease, we reviewed a relatively large number of KTS patients who presented to our vascular anomalies center.
Methods We conducted a retrospective study with 19 patients who were diagnosed with KTS and treated in our vascular anomalies clinic between 2003 and 2014, and examined their demographic characteristics, their clinical features, and the treatments administered.
Results The sex distribution was balanced, with 9 (47%) males and 10 (53%) females. The mean follow-up period was 4.1 years (range, 7 months-9 years). Most of the patients received conservative treatments such as medication or physiotherapy. Compression therapies such as wearing of elastic garments/bandages were also administered, and surgical interventions were considered only when the patients became excessively symptomatic. Other treatments included laser therapy and sclerotherapy, and all the treatments were adjusted according to each case, tailored to the conditions of the individual patients.
Conclusions KTS is an extremely rare, multifactorial disorder that induces widely varied symptoms. Because of this unique feature, plastic surgeons, when not careful, tend to attach a one-sided importance to typical symptoms such as limb hypertrophy or capillary malformation and thus overlook other symptoms and clinical features. KTS can be suspected in all infants who show capillary malformations or limb hypertrophy and require a multi-disciplinary approach for comprehensive management.
#
INTRODUCTION
Depending on the nature of the cells constituting a lesion, vascular anomalies can be divided into the vascular tumor group and the vascular malformation group. According to the classification of the International Society for the Study of Vascular Anomalies, officially recognized in 1996, the Klippel-Trenaunay syndrome (KTS) can be classified as combined vascular malformations that affect the capillary, venous, and lymphatic systems. KTS is characterized by three clinical features, namely cutaneous capillary malformations, venous malformations, and soft tissue and/or bony hypertrophy of the extremity. KTS is named after two French physicians, Klippel and Trenaunay [[1]], who first described its possible clinical features in the 1990s. KTS can be diagnosed when at least two of the three abovementioned major clinical features are present [[2]]. KTS is a combined capillary-lymphatic-venous malformation (CLVM) without the formation of any noticeable arteriovenous fistula [[3]]. The etiology is obscure and has been postulated to result from an embryonic developmental disorder of mesodermal tissues that affect angiogenesis at different stages, possibly following intra-uterine insult [[4]]. Other researchers have argued that deep vein obstruction and/or atresia cause chronic venous hypertension, ultimately resulting in port-wine stains, varicose veins, and limb hypertrophy. There is no documented sex predilection, and the lesions can involve the lower or upper limbs and rarely the trunk. KTS patients present many symptoms such as mild hypertrophy, stains, and a few venous varicosities. Occasionally, they may also present with symptoms such as hematuria and/or hematochezia when an internal organ is associated [[5]]. The differential diagnosis for a vascular lesion associated with limb enlargement also includes other disorders such as the Sturge-Weber syndrome, the Parkes-Weber syndrome, and the Proteus syndrome. Because of the overlap with other vascular malformation syndromes, KTS causes further confusion. The varied manifestations are attributed to the unpredictable clinical nature of vascular malformations. Therefore, all treatments should be adjusted according to the individual patients' symptoms, clinical course, and prognoses. The review of the medical records of the patients who underwent treatment at our vascular anomalies center also verified the diversity of the clinical features and courses, as well as their respective therapies.
#
METHODS
This study was conducted in 19 patients who were diagnosed with KTS at our vascular anomalies center between 2003 and 2014. We performed a retrospective review of medical records and radiologic findings. In general, the vascular stain appeared at birth, mostly on the lower limbs. Echo/Doppler and duplex scanning were the most efficacious methods for assessing vascular anomalies and arteriovenous shunts. Fast-flow arteriovenous fistula can be distinguished by time resolved imaging of contrast kinetics magnetic resonance imaging (MRI) at our vascular anomalies center. Further, in this study, none of the 19 patients had clinical evidence of arteriovenous fistula. Plain radiography or scanogram was performed to assess bone hypertrophy and limb-length discrepancy. In general, there are some differences on the images of the adult patients, but no noticeable differences were observed in the young patients. The MRI clearly displayed the degree of soft tissue hypertrophy and bone involvement, and confirmed the abnormality of the related lymphatic vasculature or absence thereof.
#
RESULTS
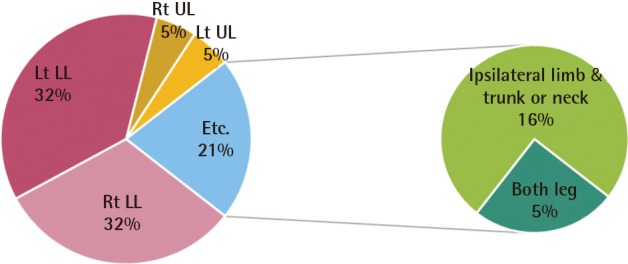
The patients' demographic data and clinical features and the treatments administered were outlined ([Table 1]). Of the 19 patients with KTS, 9 (47%) were male and 10 (53%) were female. Fifteen (79%) patients showed malformations on one limb only. The lower limbs were affected in 13 patients (68%), the left leg in 7 and the right leg in 6. Two patients showed malformations on the upper limbs (11%), one on the left and the other on the right arm. In three patients, the vascular anomalies spread to the trunk or neck; all of them had only one limb affected. Four patients (21%) showed malformations on two limbs; one patient, on both legs; and three patients, on the ipsilateral limb and trunk or neck ([Fig. 1]). The mean follow-up period was 4.1 years (range, 7 months to 9 years). An 18-year-old male presented with varicose veins and hypertrophy of the lower extremity ([Fig. 2]). He was managed by elastic garments and medical drugs such as Entelon (Hanlim Pharm. Co., Yongin, Korea) and prophylactic antibiotics. Entelon is made of the Vitis vinifera extract and is used for improving veno-lymphatic insufficiency symptoms such as heaviness, pain, and lymphedema of the extremities. A 7-year-old female presented with capillary malformation on the affected extremity. A dilated superficial venous system and a persistent embryonic lateral marginal vein were also observed ([Fig. 3]). She was treated by sclerotherapy in combination with compression therapy. A 33-year-old female presented with a capillary-venous malformation and soft tissue hypertrophy of the affected extremity ([Fig. 4]). She received conservative treatment, and the follow-up period was 9 years. Many patients with KTS can be managed conservatively by medical drugs or physical therapy. Compression therapy such as the use of an elastic garment/bandage is also effective in patients suffering from limb swelling, edema, and/or pain. Pulsed dye laser therapy can be used for cosmetic reasons, and in our series, seven patients were treated. Surgical intervention was indicated when they became excessively symptomatic. In our series, three patients were treated with sclerotherapy for varicose veins and one patient was operated on for complaints of bleeding and recurrent ulceration. Inversion stripping and multiple-stab avulsion were performed under spinal anesthesia. With respect to the limb-length discrepancy, a cutoff of 2.0-cm difference was suggested for epiphysiodesis [[2] [6]]. In our series, one patient was treated with an orthotic insole, and epiphysiodesis was not performed ([Fig. 5]). Because of the varied clinical manifestations, individual patients received personalized treatments according to their age and symptoms.





#
DISCUSSION
KTS is a rare form of disease that has a low incidence level and few reported cases in Korea. A few review articles have been published with respect to its clinical characteristics, manifestations, and prognoses, but the subjects included in these articles were mostly of a Caucasian origin, which made it difficult to directly apply the findings to Korean patients. Thus, in this article, we summarized the diverse clinical manifestations and treatments of KTS patients over a period of 12 years.
KTS is characterized by three clinical features, namely capillary malformations in the skin (nevus flammeus), venous malformations, and soft tissue hypertrophy. After the first mention of KTS by Klippel and Trenaunay, Parkes Weber detected patients in whom the three clinical features specific to KTS and arteriovenous fistula were found concurrently. Some medical scholars termed it the Klippel-Trenaunay-Weber syndrome [[7]]. However, the recent trend is in favor of treating these patients as cases of KTS plus arteriovenous fistula as a separate disease, calling it the Parkes Weber syndrome. As its etiology and pathogenesis have not yet been elucidated, no consensus has been reached about the appropriate treatments. A considerable amount of research will have to be conducted to better understand its underlying pathological process and thus to find more appropriate and efficacious treatment methods. Servelle [[8]] argued that deep venous stenosis or occlusion leads to port-wine stains, varicose veins, and limb hypertrophy. Meanwhile, Baskerville et al. [[4]] reported the results of a study that used phlebography; that is, deep venous stenosis was observed in only 5 of the 36 limbs affected. Thereupon, the author argued that KTS is a mesodermal disorder and that deep vein abnormalities are not part of its etiology but one of its numerous clinical features. Other researchers have held the view that KTS may be attributable to somatic mutations of the factors important for vasculogenesis or angiogenesis in the embryonic developmental process [[9]]. According to a few journal articles, KTS mostly occurs sporadically, with only rare cases of familial background, manifesting different types of anomalies, if any, among family members [[10] [11]]. Patients with KTS show a wide range of symptoms covering a broad spectrum of severity, from negligible hypertrophy of the limbs or slight varicosities to life-threatening complications. Numerous complications are associated with this syndrome, including thrombosis, coagulopathy, pulmonary embolism, heart failure, hemothorax, and bleeding from abnormal vessels of the gastrointestinal tract, kidney, or genitalia [[12] [13] [14]]. Patients with abnormal lymphatic drainage are at a higher risk of contracting cellulitis and bacteremia [[15]]. Moreover, affected individuals may experience deep emotional and psychological trauma due to their deformed appearance [[16]]. No prospective study has yet been conducted on the seriousness of KTS. Despite numerous retrospective studies, no clear conclusions have yet been drawn on its prognostic factors that are conducive to the assessment of its clinical course. KTS patients and their parents are constantly faced with a seemingly endless series of complications associated with the disease and often feel helpless about the lack of clear countermeasures. In addition, many KTS-related reports published in journals tend to attach more importance to the emphasis of the hazard and seriousness of the disease instead of presenting therapeutic approaches and useful recommendations.
KTS is a complex multifactorial disease that affects the upper and lower limbs, and more rarely, the trunk and neck. No sex dominance is observed, as in our study (male-to-female ratio, 9:10). Although an earlier article reported on familial incidences associated with the translocation between chromosomes 8 and 14, KTS is considered to occur sporadically and accidentally [[17]]. In our study, no familial incidences or backgrounds were verified. Many patients had capillary malformations when diagnosed; they were characteristically patchy in distribution with a sharp border. The venous malformations included varicose veins and atretic deep venous systems. A plethora of venous malformations have been reported in KTS patients, including anomalies of the deep venous system, such as atresia, partial or complete agenesis, hypoplasia, or valvular incompetence [[18]]. The varied clinical manifestations are attributed to the unpredictable location of vascular malformations. Although the hundreds of studies that have been conducted over the past century have reported on the features as sociated with KTS, the etiology or pathogenesis of KTS is yet to be elucidated. Moreover, its diagnostic and therapeutic methods have not been established as yet, as well as any criterion standard of assessment. Up to now, there has been no certainly established prognostic factor of KTS. In general, the capillary malformations in KTS patients are not excised. The most common treatment method is pulsed dye laser therapy, and surgical intervention is indicated when the patients become excessively symptomatic [[19]]. Management of varicosities in KTS patients is generally conservative with compression therapy, although surgical management has been reported with considerable success [[20] [21]]. Wearing of compression garments/bandages is efficacious for patients with limb hypertrophy, venous stasis, and phlebitis, but their application poses problems for rapidly growing infants and small children. This situation should be improved through adequate research to determine the benefits or drawbacks of applying compression garments to infants and small children, and the application methods and appropriate use periods. Although ulceration or bleeding from the lesions merits excision, these are generally associated with poor and delayed healing [[22]]. Prior to all surgical interventions, the blood flow in the deep venous system should be checked by using contrast venography and MRI. The primary goal is to confirm the patency of the deep venous system before excision. Deep venous system atresia is occasionally treated with reconstruction or bypass, but the reconstruction of a deep vein was not performed in our series [[23]]. Although deep vein thrombosis or pulmonary embolism has been reported in KTS patients, it did not occur in our series [[24]]. KTS diagnosis is a great challenge because of the widely varied clinical manifestations and symptoms of KTS. This should be kept in mind in order to not inadvertently miss the signs and symptoms of KTS. Unpredictable chronological changes and courses of KTS signs and symptoms can be overlooked unless constant vigilance is exercised. In other words, KTS requires a comprehensive multidimensional approach to ensure appropriate diagnosis and treatment ([Fig. 6]).

#
#
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
This article was presented at the 72nd Congress of the Korean Society of Plastic and Reconstructive Surgeons on November 9, 2014, in Seoul, Korea.
-
References
- 1 Klippel M, Trenaunay P. Du naevus variquex osteohypertrophique. Arch Gen Med 1900; 3: 641-672
- 2 Jacob AG, Driscoll DJ, Shaughnessy WJ. et al. Klippel-Trenaunay syndrome: spectrum and management. Mayo Clin Proc 1998; 73: 28-36
- 3 Lindenauer SM. The Klippel-Trenaunay syndrome: varicosity, hypertrophy and hemangioma with no arteriovenous fistula. Ann Surg 1965; 162: 303-314
- 4 Baskerville PA, Ackroyd JS, Browse NL. The etiology of the Klippel-Trenaunay syndrome. Ann Surg 1985; 202: 624-627
- 5 Husmann DA, Rathburn SR, Driscoll DJ. Klippel-Trenaunay syndrome: incidence and treatment of genitourinary sequelae. J Urol 2007; 177: 1244-1249
- 6 Garzon MC, Huang JT, Enjolras O. et al. Vascular malformations. Part II: associated syndromes. J Am Acad Dermatol 2007; 56: 541-564
- 7 Ziyeh S, Spreer J, Rossler J. et al. Parkes Weber or Klippel-Trenaunay syndrome? Non-invasive diagnosis with MR projection angiography. Eur Radiol 2004; 14: 2025-2029
- 8 Servelle M. Klippel and Trenaunay's syndrome: 768 operated cases. Ann Surg 1985; 201: 365-373
- 9 Berry SA, Peterson C, Mize W. et al. Klippel-Trenaunay syndrome. Am J Med Genet 1998; 79: 319-326
- 10 Aelvoet GE, Jorens PG, Roelen LM. Genetic aspects of the Klippel-Trenaunay syndrome. Br J Dermatol 1992; 126: 603-607
- 11 Craven N, Wright AL. Familial Klippel-Trenaunay syndrome: a case report. Clin Exp Dermatol 1995; 20: 76-79
- 12 Torregrosa A, Marti-Bonmati L, Higueras V. et al. Klippel-Trenaunay syndrome: frequency of cerebral and cerebellar hemihypertrophy on MRI. Neuroradiology 2000; 42: 420-423
- 13 Telander RL, Kaufman BH, Gloviczki P. et al. Prognosis and management of lesions of the trunk in children with Klippel-Trenaunay syndrome. J Pediatr Surg 1984; 19: 417-422
- 14 Samuel M, Spitz L. Klippel-Trenaunay syndrome: clinical features, complications and management in children. Br J Surg 1995; 82: 757-761
- 15 Bird LM, Jones MC, Kuppermann N. et al. Gram-negative bacteremia in four patients with Klippel-Trenaunay-Weber syndrome. Pediatrics 1996; 97: 739-741
- 16 van der Ploeg HM, van der Ploeg MN, van der Ploeg-Stapert JD. Psychological aspects of the Klippel-Trenaunay syndrome. J Psychosom Res 1995; 39: 183-191
- 17 Wang Q, Timur AA, Szafranski P. et al. Identification and molecular characterization of de novo translocation t(8;14)(q22.3;q13) associated with a vascular and tissue overgrowth syndrome. Cytogenet Cell Genet 2001; 95: 183-188
- 18 Baskerville PA, Ackroyd JS, Lea Thomas M. et al. The Klippel-Trenaunay syndrome: clinical, radiological and haemodynamic features and management. Br J Surg 1985; 72: 232-236
- 19 Alster T. Laser treatment of vascular lesions. In: Alster TS. Manual of cutaneous laser techniques. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 1999: 33-52
- 20 Noel AA, Gloviczki P, Cherry Jr KJ. et al. Surgical treatment of venous malformations in Klippel-Trenaunay syndrome. J Vasc Surg 2000; 32: 840-847
- 21 Gloviczki P, Hollier LH, Telander RL. et al. Surgical implications of Klippel-Trenaunay syndrome. Ann Surg 1983; 197: 353-362
- 22 Gates PE, Drvaric DM, Kruger L. Wound healing in orthopaedic procedures for Klippel-Trenaunay syndrome. J Pediatr Orthop 1996; 16: 723-726
- 23 Gloviczki P, Bergan JJ, Rhodes JM. et al. Mid-term results of endoscopic perforator vein interruption for chronic venous insufficiency: lessons learned from the North American subfascial endoscopic perforator surgery registry. The North American Study Group. J Vasc Surg 1999; 29: 489-502
- 24 Kanterman RY, Witt PD, Hsieh PS. et al. Klippel-Trenaunay syndrome: imaging findings and percutaneous intervention. AJR Am J Roentgenol 1996; 167: 989-995
Correspondence
Publikationsverlauf
Eingereicht: 06. Februar 2015
Angenommen: 26. Mai 2015
Artikel online veröffentlicht:
05. Mai 2022
© 2015. The Korean Society of Plastic and Reconstructive Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonCommercial License, permitting unrestricted noncommercial use, distribution, and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes. (https://creativecommons.org/licenses/by-nc/4.0/)
Thieme Medical Publishers, Inc.
333 Seventh Avenue, 18th Floor, New York, NY 10001, USA
-
References
- 1 Klippel M, Trenaunay P. Du naevus variquex osteohypertrophique. Arch Gen Med 1900; 3: 641-672
- 2 Jacob AG, Driscoll DJ, Shaughnessy WJ. et al. Klippel-Trenaunay syndrome: spectrum and management. Mayo Clin Proc 1998; 73: 28-36
- 3 Lindenauer SM. The Klippel-Trenaunay syndrome: varicosity, hypertrophy and hemangioma with no arteriovenous fistula. Ann Surg 1965; 162: 303-314
- 4 Baskerville PA, Ackroyd JS, Browse NL. The etiology of the Klippel-Trenaunay syndrome. Ann Surg 1985; 202: 624-627
- 5 Husmann DA, Rathburn SR, Driscoll DJ. Klippel-Trenaunay syndrome: incidence and treatment of genitourinary sequelae. J Urol 2007; 177: 1244-1249
- 6 Garzon MC, Huang JT, Enjolras O. et al. Vascular malformations. Part II: associated syndromes. J Am Acad Dermatol 2007; 56: 541-564
- 7 Ziyeh S, Spreer J, Rossler J. et al. Parkes Weber or Klippel-Trenaunay syndrome? Non-invasive diagnosis with MR projection angiography. Eur Radiol 2004; 14: 2025-2029
- 8 Servelle M. Klippel and Trenaunay's syndrome: 768 operated cases. Ann Surg 1985; 201: 365-373
- 9 Berry SA, Peterson C, Mize W. et al. Klippel-Trenaunay syndrome. Am J Med Genet 1998; 79: 319-326
- 10 Aelvoet GE, Jorens PG, Roelen LM. Genetic aspects of the Klippel-Trenaunay syndrome. Br J Dermatol 1992; 126: 603-607
- 11 Craven N, Wright AL. Familial Klippel-Trenaunay syndrome: a case report. Clin Exp Dermatol 1995; 20: 76-79
- 12 Torregrosa A, Marti-Bonmati L, Higueras V. et al. Klippel-Trenaunay syndrome: frequency of cerebral and cerebellar hemihypertrophy on MRI. Neuroradiology 2000; 42: 420-423
- 13 Telander RL, Kaufman BH, Gloviczki P. et al. Prognosis and management of lesions of the trunk in children with Klippel-Trenaunay syndrome. J Pediatr Surg 1984; 19: 417-422
- 14 Samuel M, Spitz L. Klippel-Trenaunay syndrome: clinical features, complications and management in children. Br J Surg 1995; 82: 757-761
- 15 Bird LM, Jones MC, Kuppermann N. et al. Gram-negative bacteremia in four patients with Klippel-Trenaunay-Weber syndrome. Pediatrics 1996; 97: 739-741
- 16 van der Ploeg HM, van der Ploeg MN, van der Ploeg-Stapert JD. Psychological aspects of the Klippel-Trenaunay syndrome. J Psychosom Res 1995; 39: 183-191
- 17 Wang Q, Timur AA, Szafranski P. et al. Identification and molecular characterization of de novo translocation t(8;14)(q22.3;q13) associated with a vascular and tissue overgrowth syndrome. Cytogenet Cell Genet 2001; 95: 183-188
- 18 Baskerville PA, Ackroyd JS, Lea Thomas M. et al. The Klippel-Trenaunay syndrome: clinical, radiological and haemodynamic features and management. Br J Surg 1985; 72: 232-236
- 19 Alster T. Laser treatment of vascular lesions. In: Alster TS. Manual of cutaneous laser techniques. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 1999: 33-52
- 20 Noel AA, Gloviczki P, Cherry Jr KJ. et al. Surgical treatment of venous malformations in Klippel-Trenaunay syndrome. J Vasc Surg 2000; 32: 840-847
- 21 Gloviczki P, Hollier LH, Telander RL. et al. Surgical implications of Klippel-Trenaunay syndrome. Ann Surg 1983; 197: 353-362
- 22 Gates PE, Drvaric DM, Kruger L. Wound healing in orthopaedic procedures for Klippel-Trenaunay syndrome. J Pediatr Orthop 1996; 16: 723-726
- 23 Gloviczki P, Bergan JJ, Rhodes JM. et al. Mid-term results of endoscopic perforator vein interruption for chronic venous insufficiency: lessons learned from the North American subfascial endoscopic perforator surgery registry. The North American Study Group. J Vasc Surg 1999; 29: 489-502
- 24 Kanterman RY, Witt PD, Hsieh PS. et al. Klippel-Trenaunay syndrome: imaging findings and percutaneous intervention. AJR Am J Roentgenol 1996; 167: 989-995