

Subscribe to RSS
DOI: 10.5935/1984-0063.20190081
Increase in the frequency of obstructive sleep apnea in elderly people
Authors

BACKGROUND The prevalence of obstructive sleep apnea (OSA) increases with age. However, older adults have limited perception of the symptoms related with poor sleep quality.
Objectives To know the frequency and characteristics of age-related OSA in a large population with clinical suspicion of sleep apnea.
Methods We conducted a retrospective study. OSA was studied by respiratory polygraphy (RP). Patients were grouped by age (G): GI was between 18-45; GII: 46-65 and GIII > 65 years old. Other demographic characteristics, symptoms and RP indicators were compared. Epworth Sleep Scale (ESS) was used to analyze symptoms.
Results We included 2491 patients with sleep apnea symptoms. OSA frequency (AHI > 15) in each group was 33.2 % in GI; 45.8 in GII and 50.3 in GIII (p < 0.001). Despite the significant increase in OSA severity, GIII group reported fewer symptoms (ESS: 6.0; p < 0.001). Multivariate adjusted analysis showed that the odds ratio of having OSA is three times as high at age > 65 (OR: 3.32 (2.29 - 4.88) p < 0.001).
Conclusions As in previous reports, OSA prevalence in our population was higher among the elderly. The early identification of this syndrome in a population with poor perception of symptoms would aid to improve patient management.
INTRODUCTION
A rise in the prevalence of obstructive sleep apnea (OSA) characterized by nocturnal episodes of upper airway obstruction, sleep fragmentations and hypoxemia has been observed in the elderly population[1]. Physiological and physical changes would be related with sleep quality, quantity, and its architecture[2].
OSA consequences in this population are well known as the decline in cognitive function has been related with an increase of the apnea-hypopnea index (AHI). Elderly patients with OSA have shown an impairment in physical and memory functions and a higher risk of falls than counterparts without OSA[3]. In addition, OSA in older populations has been associated with negative outcomes such as stroke[4], non-dipper pattern or nocturnal hypertension[5] and mortality[6].
Moreover, OSA symptoms may be under-recognized by patients, caregivers, and even doctors as a "natural" occurrence of aging. These patients commonly present lower Epworth Sleepiness Scale (ESS) scores, and less excessive daytime sleepiness compared with younger patients[1].
The aim of this study was to know the frequency and characteristics of age-related OSA in a large population with clinical suspicion of sleep apnea.
MATERIALS AND METHODS
Study design
We performed a single-center, retrospective study. The protocol was approved by the Ethics and Review Committee at "Hospital Británico" in accordance with the ethical standards of Helsinki Declaration.
Patients
Consecutive patients referred for Respiratory Polygraphy (RP) between 09/2009 and 03/2017 were included based on the following criteria: > 18 years old, clinical suspicion of sleep apnea due to symptoms such as snoring, apneas observed by others and/or excessive daytime sleepiness. Patients with a known diagnosis of COPD, obesity hypoventilation syndrome, chronic heart failure, and neuromuscular disorders were excluded.
Anthropometric data and the ESS and Berlin questionnaire answers were obtained when the RP equipment was delivered to patients at the hospital.
Patients were grouped by age (G): GI :18-45; GII: 46-65; GIII: > 65 years old.
RP Recordings
Patients were trained on the use, assembly and turning on-off of RP devices. They also received printed instructions with iconographic information for operation. The devices used were: Apnea Link Air® (ResMed, Sydney-Australia) and Alice PDX® and Alice night One® (Philips-Respironics, USA). All were equipped with a pulse oximeter, effort belts and a high-sensitive nasal pressure cannula (level III devices from the American Academy of Sleep Medicine).
Recordings were manually analyzed using specific software. Events were manually scored by pulmonologists trained under the guidelines of the American Academy of Sleep Medicine (AASM).
Recordings were analyzed in 3-5 minutes' epochs. When necessary, respiratory events were corrected manually. Recording sections with low quality signals or transient disconnections were removed. Only recordings with a valid total recording time (TRT) of > 240 minutes (> 4 hours) were accepted. Apnea and hypopnea were defined as a > 80% drop from baseline airflow for ≥ 10 seconds and a 50% drop for ≥10 seconds associated to ≥ 3% oxygen desaturation, respectively. The AHI was calculated as the number of apneas/hypopneas per hour of valid TRT. Patients were classified either as normal (AHI < 5/h), mild (AHI ≥ 5 and < 15), moderate (AHI ≥ 15 and < 30), or severe (AHI ≥ 30). After clinical evaluation, pulmonologists based their recommendations for the use of CPAP on local standards.
Statistical Analysis
Categorical data are presented as absolute numbers and percentages, and continuous data as means and standard deviations (SD) or median and interquartile ranges (IQR) for normally and not normally distributed data, respectively. Normal assumption was assessed using visual inspection of histograms and the Shapiro-Wilk test.
Comparison of categorical variables between groups was conducted using the chi2 test or the Fisher's exact test as appropriate. To compare continuous variables among groups, ANOVA or Kruskal-Wallis test were used for normally and not normally distributed variables, respectively. We used Tukey's multiple comparisons test as post hoc range tests for the different age groups.
To evaluate the independent contribution of age to the presence of OSA, a multivariate logistic regression model was constructed. Variables introduced to the models included those with univariate association with OSA exhibiting a p value < 0.10 and the gender.
All analyses were two tailed and a p value < 0.05 was considered statistically significant.
Data were analyzed with R: a language and environment for statistical computing version 3.4.1 for OSx (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
We included 2491 patients (61.3% males; mean age: 53.9±13.9, range: 19-89) ([Table 1]). Two hundred fifty-eight patients (10.05%) presented previous OSA diagnosis and 251 (11.4%:) reported psychiatric disorders. Median of body mass index (BMI) was 31.2±7.9 kg/m[2]; 29.6% were overweight and 58.2% were obese (BMI > 30).
|
Variables |
All patients |
Group I |
Group II |
Group III |
p value |
|---|---|---|---|---|---|
|
n |
2491 |
669 |
1279 |
543 |
- |
|
Age, mean (SD) |
53.9 (13.9) |
35.8 (6.7) |
55.8 (5.6) |
71.0 (4.8) |
- |
|
Male, n (%) |
1526 (61.3) |
421 (62.9) |
771 (60.3) |
334 (61.5) |
0.521 |
|
BMI (Kg/m2), median (IQR) |
31.2 |
31.8 |
31.6 |
30.5 |
< 0.001 |
|
(27.3 - 37.4) |
(26.8 - 40.4) |
(27.7 - 37.4) |
(27.2 - 34.1) |
||
|
Neck circumference, n (%) †† |
1157 (59.9) |
255 (47.7) |
648 (65.3) |
254 (62.9) |
< 0.001 |
|
Psychiatric disorders, n (%)* |
251 (11.4) |
35 (5.8) |
143 (12.7) |
73 (15.6) |
< 0.001 |
|
ESS, median (IQR)** |
7.0 |
8.0 |
7.0 |
6.0 |
< 0.001 |
|
(4.0 - 12.0) |
(4.0 - 12.0) |
(4.0 - 12.0) |
(3.0 - 10.0) |
||
|
ESS > 10, n (%)** |
740 (29.9) |
223 (33.6) |
392 (30.9) |
125 (23.1) |
< 0.001 |
|
Berlin high risk, n (%) † |
2189 (88.1) |
561 (84.2) |
1155 (90.4) |
473 (87.1) |
< 0.001 |
|
Snoring, n (%) †† |
1235 (64.0) |
324 (60.7) |
657 (66.2) |
254 (62.9) |
0.085 |
|
Daytime sleepiness, n (%)††† |
1355 (70.2) |
388 (72.5) |
695 (70.1) |
272 (67.3) |
0.225 |
|
AHI > 5, n (%)*** |
1934 (77.7) |
440 (65.8) |
1044 (81.7) |
450 (82.9) |
< 0.001 |
|
AHI > 15, n (%)*** |
1080 (43.4) |
222 (33.2) |
585 (45.8) |
273 (50.3) |
< 0.001 |
|
AHI > 30, n (%)*** |
461 (18.5) |
97 (14.9) |
250 (19.5) |
112 (20.6) |
< 0.05 |
|
Cheyne-Stokes, n (%) |
55 (2.2) |
7 (0.6) |
17 (1.3) |
34 (6.3) |
< 0.001 |
|
High blood pressure, n (%) †† |
895 (46.3) |
107 (20.0) |
510 (51.4) |
278 (68.8) |
< 0.001 |
The findings showed a significant, stepped increase in OSA frequency (AHI > 15 events / hour) associated with age groups: 33.6% in Group I; 45.8% in Group II and 50.3% in Group III (p<0.001).
In spite of these results, perception of diurnal symptoms (ESS) diminished with aging ([Table 1]). ESS showed a significant decrease associated with age groups (8.5±5.2; 8.2±5.2 and 7.0±4.2; p<0.01) ([Figure 1]). Accordingly, the percentage of patients with ESS > 10 diminished with age (GI: 33.6; GII: 30.9 and GIII: 23.1; p<0.01) ([Table 1]).

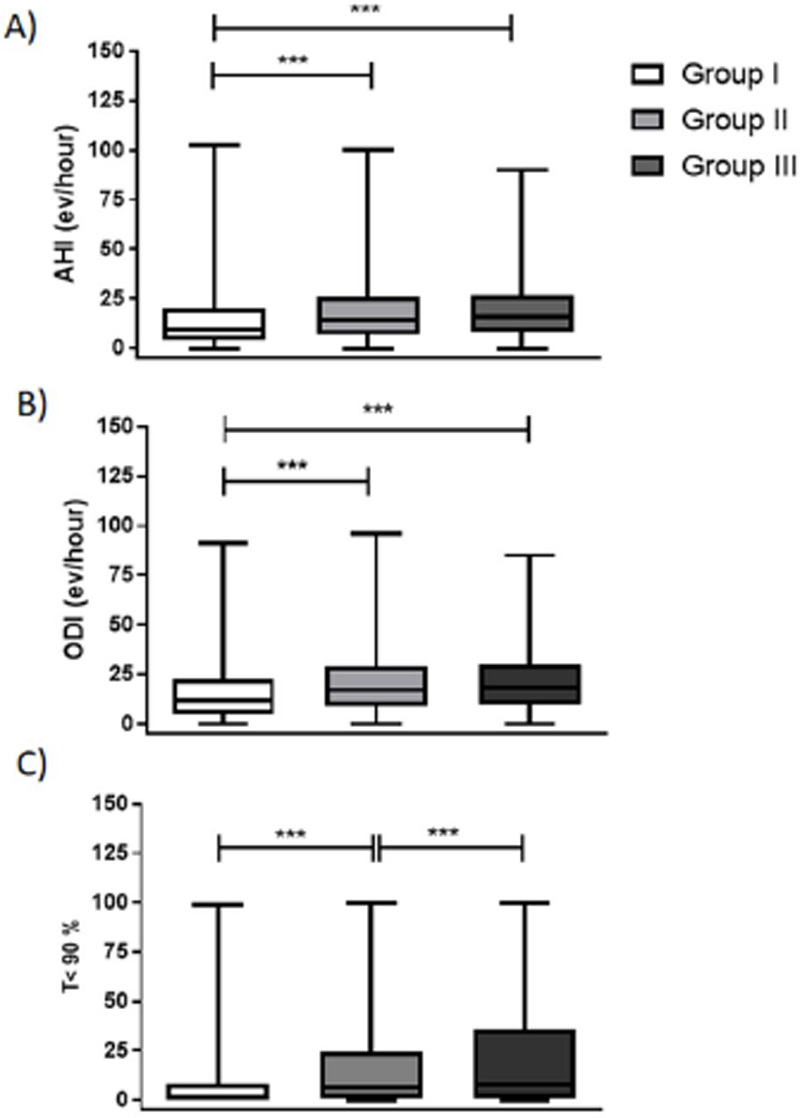
RP indicators increased with age. AHI values were 16.4±19.3, 19.2±16.7, 19.9±16.1 events/hours (p<0.001) in groups I, II and III respectively. Similar 1results were observed in terms of Oxygen Desaturation Index (ODI) (threshold 3%), 18.1±19.0, 21.9±17.4 and 22.3±16.3 events/hours (p<0.001). Finally, time of desaturation below 90% was 9.1±17.8, 16.9±23.4 and 23.1±29.2% (p<0.001), respectively ([Figure 2]).
In [Table 2], a multivariate logistic regression analysis suggests the odds ratio of having OSA with clinical relevance increased threefold with age > 65 years (> 15 ev/hour).
|
Variables |
Unadjusted analyses |
Adjusted analyses |
||
|---|---|---|---|---|
|
OR (95% CIs) |
p value |
OR (95% CIs) |
p value |
|
|
Age groups, |
|
|
|
|
|
Group I |
Ref. |
|
Ref. |
|
|
Group II |
2.32 (1.88 - 2.88) |
< 0.001 |
2.77 (2.09 - 3.67) |
< 0.001 |
|
Group III |
2.52 (1.92 - 3.33) |
< 0.001 |
3.32 (2.29 - 4.88) |
< 0.001 |
|
Male gender |
2.42 (2.00 - 2.93) |
< 0.001 |
2.62 (2.04 - 3.37) |
< 0.001 |
|
BMI (per unit) |
1.08 (1.06 - 1.09) |
< 0.001 |
1.09 (2.04 - 1.12) |
< 0.001 |
|
ESS (per unit) |
1.02 (1.01 - 1.04) |
0.014 |
1.03 (1.00 - 1.05) |
0.044 |
|
High blood pressure |
2.37 (1.88 - 3.00) |
< 0.001 |
1.33 (1.02 - 1.74) |
0.038 |
|
Neck circumference > 42 cm |
3.27 (2.61 - 4.11) |
< 0.001 |
1.45 (1.11 - 1.91) |
0.006 |
DISCUSSION/CONCLUSION
OSA increases linearly with age[7]. A higher prevalence has been found in healthy populations > 65 years, with more than 50% showing AHI > 5, and 20% AHI > 15 events/hour[8]. Our study, performed with home sleep testing, has found high prevalence of clinically relevant OSA in elderly patients. The population studied was referred to sleep units because they were considered at high risk for sleep disorders. We observed that more than 50% of patients had AHI > 15, and even considering this is a demanding cut-off point, this population is considered at risk for unfavorable cardiovascular outcomes.
As previously reported[9], our patients showed scarce symptoms and AHI values increased with age. Such reduced perception of symptoms may be associated with underdiagnosis of OSA in elderly patients.
In our study, elderly patients showed a significant increase in ODI and time below 90% as compared with younger subjects. AHI has been extensively used for OSA diagnosis, but it entails many limitations when it comes to assessing severity. A progressively worse hypoxemia profile could be worth studying in elderly patients who have a higher prevalence of cardiac arrhythmias, ischemic events and neurocognitive disorders[10].
Our study included patients referred to our sleep unit for being at risk of sleep disturbances, and thus, do not represent the general population. However, our findings contribute to describe the high prevalence of sleep breathing disorders and poor perception of symptoms in an elderly population.
Regardless of symptom manifestation, objective tests are needed for populations with suspected OSA and comorbidities (such as hypertension and obesity). The role of nocturnal hypoxemia as a severity modifier should be highlighted.
Conflict of Interests
The authors have no conflict of interests to declare.
Acknowledgement
We thank the hospital's technical staff who collaborated daily with the delivery and reception of equipment facilitating the subsequent data collection for this study.
Statement of Ethics
The protocol was approved by the Ethics and Review Committee at "Hospital Británico" in accordance with the ethical standards of Helsinki Declaration.
Author Contributions
Glenda Ernst and Javier Mariani wrote the manuscript and analyzed the results Magalí Blanco, Bárbara C Finn and Alejandro Salvado collaborated with data collection and manuscript writing. Eduardo Borsini to collaborate as supervisor from the all complete study and to write the manuscript.
Funding Sources
No funding was required to conduct this study.
Appendix
Supplementary Material We had no supplementary material
-
REFERENCES
- 1 Neikrug AB, Ancoli-Israel S. Sleep disorders in the older adult - a minireview. Gerontology. 2010;56(2):181-9.
- 2 Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47-112.
- 3 Cohen-Zion M, Stepnowsky C, Marler, Shochat T, Kripke DF, Ancoli- Israel S. Changes in cognitive function associated with sleep disordered breathing in older people. J Am Geriatr Soc. 2001;49(12):1622-7.
- 4 Munoz R, Duran-Cantolla J, Martínez-Vila E, Gallego J, Rubio R, Aizpuru F, et al. Severe sleep apnea and risk of ischemic stroke in the elderly. Stroke. 2006;37(9):2317-21.
- 5 Onen SH, Lesourd B, Ouchchane L, Lin JS, Dubray C, Gooneratne NS, et al. Occult nighttime hypertension in daytime normotensive older patients with obstructive sleep apnea. J Am Med Dir Assoc. 2012;13(8):752-6.
- 6 Gooneratne NS, Richards KC, Joffe M, Lam RW, Pack F, Staley B, et al. Sleep disordered breathing with excessive daytime sleepiness is a risk factor for mortality in older adults. Sleep. 2011;34(4):435-42.
- 7 Young T, Peppard PE, Gottlieb DJ. The epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217-39.
- 8 Durán J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apnea-hypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163(3 Pt 1):685-9.
- 9 Martínez-García MA, Durán-Cantolla J, Montserrat JM. Sleep apneahypopnea syndrome in the elderly. Arch Bronconeumol. 2010;46(9):479-88.
- 10 Kendzerska T, Gershon AS, Hawker G, Leung RS, Tomlinson G. Obstructive sleep apnea and risk of cardiovascular events and all-cause mortality: a decade-long historical cohort study. PLoS Med. 2014;11(2):e1001599.
Corresponding author:
Publication History
Received: 16 January 2019
Accepted: 28 July 2019
Article published online:
31 October 2023
© 2023. Brazilian Sleep Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
REFERENCES
- 1 Neikrug AB, Ancoli-Israel S. Sleep disorders in the older adult - a minireview. Gerontology. 2010;56(2):181-9.
- 2 Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47-112.
- 3 Cohen-Zion M, Stepnowsky C, Marler, Shochat T, Kripke DF, Ancoli- Israel S. Changes in cognitive function associated with sleep disordered breathing in older people. J Am Geriatr Soc. 2001;49(12):1622-7.
- 4 Munoz R, Duran-Cantolla J, Martínez-Vila E, Gallego J, Rubio R, Aizpuru F, et al. Severe sleep apnea and risk of ischemic stroke in the elderly. Stroke. 2006;37(9):2317-21.
- 5 Onen SH, Lesourd B, Ouchchane L, Lin JS, Dubray C, Gooneratne NS, et al. Occult nighttime hypertension in daytime normotensive older patients with obstructive sleep apnea. J Am Med Dir Assoc. 2012;13(8):752-6.
- 6 Gooneratne NS, Richards KC, Joffe M, Lam RW, Pack F, Staley B, et al. Sleep disordered breathing with excessive daytime sleepiness is a risk factor for mortality in older adults. Sleep. 2011;34(4):435-42.
- 7 Young T, Peppard PE, Gottlieb DJ. The epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217-39.
- 8 Durán J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apnea-hypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163(3 Pt 1):685-9.
- 9 Martínez-García MA, Durán-Cantolla J, Montserrat JM. Sleep apneahypopnea syndrome in the elderly. Arch Bronconeumol. 2010;46(9):479-88.
- 10 Kendzerska T, Gershon AS, Hawker G, Leung RS, Tomlinson G. Obstructive sleep apnea and risk of cardiovascular events and all-cause mortality: a decade-long historical cohort study. PLoS Med. 2014;11(2):e1001599.