

Subscribe to RSS
DOI: 10.4103/ijps.IJPS_23_17
Assessment of perfusion of free flaps used in head and neck reconstruction using pulsatility index
Authors
Address for correspondence:
Publication History
Publication Date:
09 July 2019 (online)


ABSTRACT
Objective: To detect venous or arterial obstruction in the pedicle of a free flap we can monitor resistance in the flap bed which is reflected in Pulsatility Index (PI) Therefore if we detect change in the values of the PI in these flaps then we can detect complications in flap due to vascular insufficiency early. Materials and Methods: Seven patients of Free Fibular Flap Reconstruction and ten patients of Free Radial Forearm Flap reconstruction were evaluated over a period of 18 months. In the pre op we recorded PI of Radial and Peroneal artery using colour doppler study. In the Post Operative Period 2 readings of PI at the anastomotic site were taken on Day 1 and Day 7. Results: Both Free Radial Forearm and Free Fibula flaps which were healthy (n = 15) showed a significant decrease in PI values on first Post Op day as compared to Pre Op. Also there was a significant fall in PI on Post Op Day 7 as compared to post op Day 1 (P < 0.05) in these flaps. The flaps developing complications (n = 2) had significantly higher Day 1 Post op PI readings as compared to healthy flaps (P < 0.05). Conclusion: PI is an objective index which can indicate changes in perfusion of free flaps used in Head and Neck reconstruction based on which we can predict if a flap is susceptible to circulatory compromise.
INTRODUCTION
The maintenance of patent vascular anastomoses is fundamental to the success of any free tissue transfer. The art and science of microsurgery have progressed steadily over the past 30 years, with advances in technical skills and equipment, and the discovery of more reliable flaps. Even though free flap success rates have risen salvage rates for failing free flaps have not increased to the same degree.
It is suggested by several authors that this is a result of late detection of vascular compromise in the flap. It is now evident that flap salvage rate is inversely related to the time interval between the onset of ischaemia and its detection.[1]
Vascular occlusion (thrombosis) remains the primary reason for flap loss, with venous thrombosis being more common than arterial occlusion.[2]
The Virchows triad (hypercoagulability, stasis and endothelial damage) does lead to thrombosis, but it is the less common factors which lead to the pre-thrombotic sates. These factors have been identified as kinks or twists in the pedicle, tight closure or oedema, haematoma and spasm or inadequate flow.[3]
The majority of flap failures occur within the first 48 h, so it is important to have a tool which can raise a red flag regarding flap survival within this period.
At present, the most common monitoring method in use is a regular clinical assessment of the flap for colour, temperature, turgor and capillary refill time. This approach is cheap but requires experienced staff, is subjective but most importantly has a slow response time.[4]
A number of modalities have been used in an attempt to move from a subjective clinical assessment to a more objective approach. These approaches have included tissue oximetry[5] intravenous fluorescein,[6] laser doppler,[7] photoplethysmography[8] temperature measurements,[9] electromagnetic flowmetry,[10] implantable Doppler[11] and microdialysis.[12] The plethora of techniques available suggests that none is optimal.
Colour Doppler Sonography has been in use for planning[13] and monitoring[14] of flaps for many years. It enables accurate measurement of blood flow velocity and quantifies the inflow and outflow of blood. However, this technique is operator-dependent[15] as the assessment of flow in a vessel at a given point is dependent on both the velocity and the cross-sectional area.
This can be seen in the following equation where velocity of blood flow in the vessel v = (Δf c)/(2ft. cosθ) where v is the velocity of the moving target, ft the frequency of the transmitted ultrasound, θ is the angle between the direction of ultrasound beam and the direction of the moving target and c is the velocity of sound in blood (1.540 m/s). Doppler shift (Δf = ft−fr) is expressed in Hertz and is the difference between the transmitted and reflected frequency from the flowing red blood cell.
To determine the quantity of blood flow through the vessel, the velocity of flow and the cross-sectional area of the vessel would be required where F = v*a (a is cross-sectional area of the vessel).
To overcome this problem, Gosling and King in 1971 developed an index which could quantify flow velocity independent of the angle of the probe – the pulsatility Index (PI).
PI = Maximum velocity − minimum velocity/mean velocity
MATERIALS AND METHODS
Over a period of approximately 2 years from August 2014 to June 2016, 17 cases of head and neck reconstruction with free flap were recruited for this observational study. Ten cases had radial forearm free flap and 7 cases needed free fibula osseo myocutaneous flaps.
The study was approved by the Institutional Ethics committee and an informed written consent was taken from all the patients enroled in the study.
A Phillips HD 7 ultrasonogram machine with high-frequency probe (4–12 MHz) was used to make all recordings. Ten cases of radial forearm free flap (RFF) reconstruction were done of which 4 cases were for cover of defects over forehead, 4 for reconstruction of tongue defects and 2 for reconstruction of angle of mouth and cheek. For reconstructing the scalp defect the recipient site vessel was superficial temporal artery and vein. In one case of forehead reconstruction, we required a cephalic vein graft from opposite forearm to anastomose the flap cephalic vein to facial vein. For all the remaining cases, the recipient site vessel was facial artery and facial vein.
For the 7 cases where free fibula osseomyocutaneous flap (FFF) were used to reconstruct defects of segmental mandibulectomy, as part of resection of carcinomas of gingivobuccal sulcus of oral cavity, the recipient site vessel was facial artery and facial vein.
The advantage of taking the facial artery and superficial temporal artery as the anastomosing vessel is that they are quite superficial. The facial artery in the neck can be easily monitored with the high-frequency probe and the task becomes much easier in those cases which undergo modified radical neck dissection type 2 as the Sternocleidomastoid is also removed. Another alternative is to monitor the perforator sites marked preoperatively in the flap. We prefer to measure the PI at the anastomosis sites in the neck and in front of the tragus (for superficial temporal artery anastomosis) as at times, it is difficult for the probe to reach the intraoral site where the perforator was marked.
A pre-operative evaluation of the donor peroneal and radial artery was done to rule out any stenosis or presence of atherosclerotic plaques. The PI of these vessels was also recorded [Table 1]. The waveform of both these vessels was found to be triphasic [Figure 1] suggesting a high peripheral vascular resistance in their vascular beds.[16]

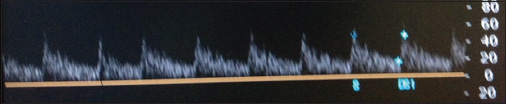
The waveforms at the anastomotic site were found to be monophasic [Figure 2] with continuous flow suggesting a low vascular resistance bed as compared to that of the forearm and leg.
After surgery PI was recorded after 24 h and on the 7th day with the patient in supine position. All measurements were performed with the help of staff of the department of radiodiagnosis. Blood pressure was also recorded simultaneously, but as all these patients had been optimised before surgery, they were all normotensive. Data regarding PI of all the healthy flaps (n = 15) at 24 h and on the 7th day along with the PI of the unhealthy flaps (n = 2) at 24 h were collated. Descriptive analysis (mean and standard deviation) for the day 1 and day 7 PI of the healthy flaps and day 1 PI of the unhealthy flaps was done. The statistical analysis was performed using paired and unpaired t-test and Pearson's correlation coefficient with a significance threshold of P < 0.05.
RESULTS
Patient demographics
Of the 17 patients enroled in the study, 9 were males and 8 females. Four patients had both hypertension and diabetes mellitus, and one had only hypertension which was controlled by medications before surgery. The mean age of the study group was 51.6 (range 35–62 years). Among the male population 3 patients were found to have a history of smoking.
Results of free fibula osseomyocutaneous flap reconstruction
Of the seven patients who underwent FFF reconstruction, the pre-operative PI of the peroneal artery was recorded. Postoperatively, at 24 h and on the 7th post-operative day, the PI was recorded at the anastomotic site on the facial artery. One flap which had high post-operative PI on the first post-operative day developed complications and could not be salvaged [Table 2].
Results of radial forearm flap reconstruction
Ten patients underwent reconstruction with the RFF flap of which 4 were for scalp defect where the anastomosis site was with the superficial temporal artery in front of the tragus. In the remainder of the 6 cases, the anastomosis was with the facial artery localised just below the angle of the mandible in the neck. One flap for tongue reconstruction which developed complication on the 3rd day had a high PI on Post-operative day 1 and was eventually salvaged [Table 3].
The comparison of PI of post-operative day 1 and day 7 for all the healthy flaps revealed a significant fall in the value of PI (P < 0.05) on paired t-test which reflects a pattern of fall in vascular resistance of the healthy flaps [Figure 3].

An unpaired t-test was used to compare the post-operative day 1 values of the healthy and the complicated flaps, and a significant difference was found in the post-operative values (P < 0.05) [Figure 4].

The normal post-operative day 1 readings for RFF and FFF were studied separately and we found that from our data the mean value of PI in FFF to be 1.36 (±0.252) on post-operative day 1. For this value, the Z-score at 95% was 1.77. A PI above 1.77, we should suspect flow problems in FFF. In case of RFF, the mean PI was 1.26 (±0.117) with Z-score at 95% 1.46 (as determined from Z-score tables). Any RFF with post-operative day 1 PI above this value should be closely monitored for flow problems.
DISCUSSION
PI was originally defined as the sum of the energies in the first and subsequent Fourier harmonics of a velocity waveform, divided by the energy in the zeroth harmonic; however, this has been superseded by a similar but simpler PI calculated merely by dividing the maximum vertical excursion of the waveform by its mean height (Gosling and King, 1974).[17]
Therefore, in a low resistance situation, the difference between the maximum and minimum velocity will not be great and the mean will tend to be moderate, and the PI will be low. However, in case of a high resistance such as venous obstruction in a free flap or downstream arterial thrombosis[16] the resistance would be significantly higher and may even lead to diastolic flow reversal. In such cases, the mean will tend towards 0 and the resulting PI will increase.
The results from our study indicate that changes in PI at the anastomotic site of the vessel seem to be an accurate indicator of flap viability and is an effective tool in predicting compromise in the flap pedicle. In all cases where the flaps remained healthy the PI showed a decreasing trend which means from post-operative day 1 to day 7 the resistance in the flap shows a decreasing trend. This is primarily due to factors such as sympathetic denervation and heightened response to hyperadrenalic state in the first twenty-four hours.[18] This change is not limited to only the RFF and FFF but is also seen on a larger scale in free muscle flaps. Studies conducted on free LD flap using transit time ultra flowmeter showed that the intraoperative transit-time flow increased significantly in the pedicle immediately after the thoracodorsal nerve had been cut.[19] This increase in blood flow might explain some of the known beneficial effects of free muscle flaps on wound healing and chronic infections.[20] [21] On the other hand, free transverse rectus abdominis muscle (TRAM) flaps do not have such a high increase in blood flow as the free muscle and RFF flaps do because of the large adipose content of this flap which has the lowest intake of blood per 100 g of tissue. This is one of the reasons for fat necrosis especially on the random side of the flap.[22] The study by Lorenzetti et al. found that the blood flow in RFF flaps is 6 times more than that of the TRAM flap so this possibly could not be because of simple vasodilation of poor vascularity of adipose tissue. A possible explanation for this is that the RFF tends to act as a shunt in the recipient area thus drawing large volumes of blood.[23] After 24 h, other factors such as opening of choke vessels, resolution of oedema and neovascularisation take the resistance in flap vascular bed further down.[24]
It would seem logical at this point to think that the pedicle should in fact show the PI of the recipient vessel but that is not the case. In fact, the waveform at the anastomotic site is completely different from the waveform recorded in the recipient artery on the opposite. In our study, we recorded the PI of the facial artery on the opposite side and the PI the site of anastomosis along with the waveform which was completely different [Figure 5a and b].

Similar results were also found by Lorizetti et al. who used transit time ultrasonic flow meter to measure intraflap haemodynamics and found that there was no correlation between the flow rates in the recipient artery and in the pedicle of free muscle flaps after anastomosis. Thus blood flow is not dependent on the recipient artery flow in either free radial forearm, TRAM or muscle flaps. On the contrary, the free flap seems to regulate the recipient artery flow according to the flap haemodynamic requirements, which presumably depend on the tissue components (vascular resistance) of the flap.
Now that it is clear that recipient artery would not affect the readings at the anastomotic site, so we can safely conclude that the changes occurring at the anastomotic site would reflect the status of the flap vascular bed. Therefore, in case the flap develops venous congestion so the resistance in the flap bed would increase and hence be reflected as raised PI at the arterial anastomotic site. In our study, the 2 flaps which developed clinical signs of venous congestion were showing raised PI after the first 24 h. The waveform of these flaps was also different from the normal anastomosis site waveform. Similar results were seen by Arya et al.[24] who monitored PI at the perforator site of DIEP flaps using a handheld colour Doppler. In their study, 4 cases developed venous congestion and showed a mean PI of 3.2 in the post-operative period as compared to the mean value of 1.2 found in all healthy flaps. In our study, the mean value of the flaps developing complication was 3.3 and those of healthy flaps was 1.3 recoded on post-operative day 1 (24 h after surgery). As with Arya et al. we also shifted the patient for salvage surgery once the clinical signs of venous congestion began to appear.
One of our cases with free fibula flap reconstruction a, 65-year-old male with poorly differentiated carcinoma of the central segment of the jaw, could not be taken up for salvage surgery immediately as our anaesthesia team termed the patient status high risk for surgery as he was still on assisted ventilation with poor glycaemic control and labile blood pressure. By the time, we could intervene the flap developed clots in the pedicle vascular bed, and the flap had to be discarded.
In our second case, a 35-year-old male with Ca tongue who received a free RFF for reconstruction of tongue defect, we were better prepared to perform a salvage surgery.
Because of raised PI readings on post-operative day 1 [Figure 6], the patient was kept under strict clinical monitoring. We also were able to counsel the patient and family that a second surgery may be required shortly. Colour change was observed about 6 h [Figure 7] after our colour Doppler study showing raised PI. On the appearance of clinical symptoms of flap compromise, the patient was shifted for salvage surgery where the venous anastomosis was taken down and redone [Figure 8].



Following redo anastomosis, the flap colour improved within the next 12 h with slight flap loss at the distal margin of the flap [Figure 9].

We did not get any case of arterial occlusion, but if it were to occur then, it would present as raised PI in the pre-stenotic and stenotic segment of the artery. It is only in the post-stenotic segment of the vessel that we may get a fall in PI as this segment undergoes vasodilation in an effort to increase blood flow. But since most cases of thrombosis are found within the first 10 mm of the anastomosis site,[3] therefore, measurement of PI at the anastomotic site will likely present as raised PI in case of arterial occlusion of the pedicle.
CONCLUSION
The measurement of PI satisfies many of the criteria of an ideal monitoring method set out by Creech and Miller.[25] It is non-invasive and harmless, rapidly-responsive, reproducible, reliable and applicable to most types of flap.
The use of PI to determine realtime changes in the vascular bed of free flaps seems an adequate tool as it is able to raise red flags regarding circulation compromise even before the clinical features present. With the introduction of handheld colour Doppler devices, it would be easier to continuously monitor flaps and data obtained from similar studies can be used to set up guidelines for intervention even before clinical changes appear in the flap.
Even though at present our return to theatre decisions are still governed by clinical signs of ischaemia in the flap, but PI does give us the advantage of proceeding with an early exploration thus increasing chances of flap salvage.
In case of the FFF none of the flaps which were normal exceeded the cut-off value but the flap which showed congestion had day 1 PI of 4.2 which exceeds the cut-off value by a large margin. Therefore, we suspect the chances of getting a false positive are higher than false negative. Similarly, in case of RFF, the flap showing congestion had a PI of 2.4 while the cut-off for RFF is 1.46 so again there are chances of false positives. Still further trials would be required to determine false positive and negative results along with cost efficiency and return to theatre rates.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
-
REFERENCES
- 1 Siemionow M, Arslan E. Ischemia/reperfusion injury: A review in relation to free tissue transfers. Microsurgery 2004; 24: 468-75
- 2 Novakovic D, Patel RS, Goldstein DP, Gullane PJ. Salvage of failed free flaps used in head and neck reconstruction. Head Neck Oncol 2009; 1: 33
- 3 Khouri RK. Avoiding free flap failure. Clin Plast Surg 1992; 19: 773-81
- 4 Smit JM, Zeebregts CJ, Acosta R, Werker PM. Advancements in free flap monitoring in the last decade: A critical review. Plast Reconstr Surg 2010; 125: 177-85
- 5 Kamolz LP, Giovanoli P, Haslik W, Koller R, Frey M. Continuous free-flap monitoring with tissue-oxygen measurements: Three-year experience. J Reconstr Microsurg 2002; 18: 487-91
- 6 Sloan GM, Sasaki GH. Noninvasive monitoring of tissue viability. Clin Plast Surg 1985; 12: 185-95
- 7 Zdolsek JM, Droog EJ, Thorfinn J, Lidman D. Laser Doppler perfusion imaging of the radial forearm flap: A clinical study. Scand J Plast Reconstr Surg Hand Surg 2006; 40: 101-5
- 8 Stack Jr. BC, Futran ND, Zang B, Scharf JE. Initial experience with personal digital assistant-based reflectance photoplethysmograph for free tissue transfer monitoring. Ann Plast Surg 2003; 51 (02) 136-140
- 9 Khouri RK, Shaw WW. Monitoring of free flaps with surface-temperature recordings: Is it reliable?. Plast Reconstr Surg 1992; 89: 495-9
- 10 Banis Jr. JC, Schwartz KS, Acland RD. Electromagnetic flowmetry – An experimental method for continuous blood flow measurement using a new island flap model. Plast Reconstr Surg 1980; 66: 534-44
- 11 Parker PM, Fischer JC, Shaw WW. Implantable pulsed Doppler cuff for long-term monitoring of free flaps: A preliminary study. Microsurgery 1984; 5: 130-5
- 12 Brix M, Muret P, Mac-Mary S, Ricbourg B, Humbert P. Microdialysis of cutaneous free flaps to monitor results of maxillofacial surgery. Rev Stomatol Chir Maxillofac 2006; 107: 31-7
- 13 Salgado CJ, Moran SL, Mardini S. Flap monitoring and patient management. Plast Reconstr Surg 2009; 124 (06) Suppl e295-302
- 14 Taylor GI, Doyle M, McCarten G. The Doppler probe for planning flaps: Anatomical study and clinical applications. Br J Plast Surg 1990; 43: 1-16
- 15 Few JW, Corral CJ, Fine NA, Dumanian GA. Monitoring buried head and neck free flaps with high-resolution color-duplex ultrasound. Plast Reconstr Surg 2001; 108: 709-12
- 16 Mehra S. Role of duplex Doppler sonography in arterial stenosis. J Indian Acad Clin Med 2010; 11 (04) 294-99
- 17 Gosling RG, King DH. Arterial assessment by Doppler shift ultrasound. Proc R Soc Med 1974; 67: 447-9
- 18 Daniel RK, Kerrigan CL. Principles and physiology of skin flap surgery. In: J. G.McCarthy. (Ed.) Plastic Surgery. Vol. 1. WB Saunders; Philadelphia: 1990. 1 275-328
- 19 Lorenzetti F, Tukiainen E, Asko-Seljavaara S. Intraoperative Evaluation of Blood Flow in free LD Muscle Free Laps. 4th European Conference of Scientists and Palstic Surgeons (ECSPS); Paris, France: 2000
- 20 Mathes SJ, Alpert BS, Chang N. Use of the muscle flap in chronic osteomyelitis: Experimental and clinical correlation. Plast Reconstr Surg 1982; 69: 815-29
- 21 B Mailänder P, Machens HG. Vascular complications after free tissue transfer. Microsurgery 1995; 16: 400-3
- 22 Berge Henegouwen DP, Stelzer G, Dautzenberg T, Helmig L, Ehresmann U. Pedal and distal lower leg bypasses with a distal arteriovenous fistula. Eur J Vasc Surg 1987; 1: 251-8
- 23 Chen LE, Seaber AV, Bossen E, Urbaniak JR. The effect of acute denervation on the microcirculation of skeletal muscle: Rat cremaster model. J Orthop Res 1991; 9: 266-74
- 24 Arya R, Griffiths L, Figus A, King D, Ramakrishnan V, Griffiths M. Post-operative assessment of perfusion of Deep Inferior Epigastric Perforator (DIEP) free flaps via Pulsatility Index (PI) using a portable colour Doppler sonogram device. J Plast Reconstr Aesthet Surg 2013; 66: 931-6
- 25 Creech B, Miller S. Evaluation of circulation in skin flaps. In: Grabb WC, Myers M. editors. Skin Flaps. Boston: Little, Brown; 1975
Address for correspondence:
-
REFERENCES
- 1 Siemionow M, Arslan E. Ischemia/reperfusion injury: A review in relation to free tissue transfers. Microsurgery 2004; 24: 468-75
- 2 Novakovic D, Patel RS, Goldstein DP, Gullane PJ. Salvage of failed free flaps used in head and neck reconstruction. Head Neck Oncol 2009; 1: 33
- 3 Khouri RK. Avoiding free flap failure. Clin Plast Surg 1992; 19: 773-81
- 4 Smit JM, Zeebregts CJ, Acosta R, Werker PM. Advancements in free flap monitoring in the last decade: A critical review. Plast Reconstr Surg 2010; 125: 177-85
- 5 Kamolz LP, Giovanoli P, Haslik W, Koller R, Frey M. Continuous free-flap monitoring with tissue-oxygen measurements: Three-year experience. J Reconstr Microsurg 2002; 18: 487-91
- 6 Sloan GM, Sasaki GH. Noninvasive monitoring of tissue viability. Clin Plast Surg 1985; 12: 185-95
- 7 Zdolsek JM, Droog EJ, Thorfinn J, Lidman D. Laser Doppler perfusion imaging of the radial forearm flap: A clinical study. Scand J Plast Reconstr Surg Hand Surg 2006; 40: 101-5
- 8 Stack Jr. BC, Futran ND, Zang B, Scharf JE. Initial experience with personal digital assistant-based reflectance photoplethysmograph for free tissue transfer monitoring. Ann Plast Surg 2003; 51 (02) 136-140
- 9 Khouri RK, Shaw WW. Monitoring of free flaps with surface-temperature recordings: Is it reliable?. Plast Reconstr Surg 1992; 89: 495-9
- 10 Banis Jr. JC, Schwartz KS, Acland RD. Electromagnetic flowmetry – An experimental method for continuous blood flow measurement using a new island flap model. Plast Reconstr Surg 1980; 66: 534-44
- 11 Parker PM, Fischer JC, Shaw WW. Implantable pulsed Doppler cuff for long-term monitoring of free flaps: A preliminary study. Microsurgery 1984; 5: 130-5
- 12 Brix M, Muret P, Mac-Mary S, Ricbourg B, Humbert P. Microdialysis of cutaneous free flaps to monitor results of maxillofacial surgery. Rev Stomatol Chir Maxillofac 2006; 107: 31-7
- 13 Salgado CJ, Moran SL, Mardini S. Flap monitoring and patient management. Plast Reconstr Surg 2009; 124 (06) Suppl e295-302
- 14 Taylor GI, Doyle M, McCarten G. The Doppler probe for planning flaps: Anatomical study and clinical applications. Br J Plast Surg 1990; 43: 1-16
- 15 Few JW, Corral CJ, Fine NA, Dumanian GA. Monitoring buried head and neck free flaps with high-resolution color-duplex ultrasound. Plast Reconstr Surg 2001; 108: 709-12
- 16 Mehra S. Role of duplex Doppler sonography in arterial stenosis. J Indian Acad Clin Med 2010; 11 (04) 294-99
- 17 Gosling RG, King DH. Arterial assessment by Doppler shift ultrasound. Proc R Soc Med 1974; 67: 447-9
- 18 Daniel RK, Kerrigan CL. Principles and physiology of skin flap surgery. In: J. G.McCarthy. (Ed.) Plastic Surgery. Vol. 1. WB Saunders; Philadelphia: 1990. 1 275-328
- 19 Lorenzetti F, Tukiainen E, Asko-Seljavaara S. Intraoperative Evaluation of Blood Flow in free LD Muscle Free Laps. 4th European Conference of Scientists and Palstic Surgeons (ECSPS); Paris, France: 2000
- 20 Mathes SJ, Alpert BS, Chang N. Use of the muscle flap in chronic osteomyelitis: Experimental and clinical correlation. Plast Reconstr Surg 1982; 69: 815-29
- 21 B Mailänder P, Machens HG. Vascular complications after free tissue transfer. Microsurgery 1995; 16: 400-3
- 22 Berge Henegouwen DP, Stelzer G, Dautzenberg T, Helmig L, Ehresmann U. Pedal and distal lower leg bypasses with a distal arteriovenous fistula. Eur J Vasc Surg 1987; 1: 251-8
- 23 Chen LE, Seaber AV, Bossen E, Urbaniak JR. The effect of acute denervation on the microcirculation of skeletal muscle: Rat cremaster model. J Orthop Res 1991; 9: 266-74
- 24 Arya R, Griffiths L, Figus A, King D, Ramakrishnan V, Griffiths M. Post-operative assessment of perfusion of Deep Inferior Epigastric Perforator (DIEP) free flaps via Pulsatility Index (PI) using a portable colour Doppler sonogram device. J Plast Reconstr Aesthet Surg 2013; 66: 931-6
- 25 Creech B, Miller S. Evaluation of circulation in skin flaps. In: Grabb WC, Myers M. editors. Skin Flaps. Boston: Little, Brown; 1975