
RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_88_19
Prospective nonrandomized analytical comparative study of clinicoradiological relationship and quality of life between lumbar interbody fusion and posterolateral lumbar fusion

- Introduction
- Materials and Methods
- Results
- Discussion
- Conclusions
- References
Study Design: This prospective, nonrandomized, analytic comparative study analyzed the outcome of 100 patients who underwent spinal fusion surgeries (Posterolateral fusion (PLF) and posterior lumbar interbody fusion [PLIF]) with 6 months of follow-up. Objective: The aim of our study was to compare clinicoradiological outcome of the lumbar spinal fusion surgeries (PLF vs. PLIF/transforaminal lumbar interbody fusion [TLIF]), to assess the quality of life pre- and post-operatively in all patients, and to compare the results within the groups. Summary of Background Data: We retrieved the articles related to posterolateral fusion (PLF) and PLIF/TLIF through computer-assisted PubMed and Cochrane database search. Most of the studies in previous literature did not show any significant difference in the success of fusion between the two groups. However, the global outcome in terms of clinical and radiological parameters was good in all the studies. Materials and Methods: Senior neurosurgeons who are part of the study treated 100 patients presented with degenerative disc disease (DDD). Patients underwent two types of spinal fusion surgeries: Posterolateral fusion (PLF) and PLIF/TLIF, and those two groups were compared for clinicoradiological outcome, successful fusion, and quality of life at 6 months of follow-up. Results were analyzed statistically using SPSS version 21.0 and presented in terms of frequency, percentage, mean, and standard deviation. Measurements were compared between groups using the Student's t-test (independent and paired) for normally distributed variables. Percentage was compared with Chi-square test in various parameters. Statistical significance was determined with P values; P < 0.05 was considered statistically significant. Results: Patients aged between 30and 65 years with lumbar DDD who met the inclusion criteria were included in the study. Patients were operated for 1–3 vertebral levels and showed clinical satisfactory outcome on visual analog scale (P = 0.004) and modified-Oswestry low back pain disability questionnaire (Oswestry disability index) (P = 0.000) at 6 months as compared to the preoperative data, which was statistically significant. Radiological outcome in terms of lumbar lordotic angle (LLA, P = 0.000) and ratio of disc space height (DSH) and height of immediate superior vertebral body (P = 0.000) at 3 months of follow-up was also statistically significant. All of our patients showed a well-placed implant (screws and cage) in the follow-up period. Our patients showed successful fusion more in the PLIF group (81.25%) as compared to the PLF group (67.30%), but those results are not statistically significant (P = 0.112), and all of our patients showed statistically significant difference (P = 0.000) in quality of life score at 6 months of follow-up when compared with the preoperative score. Conclusions: We concluded from our study and after the review of literature that the patients with lumbar DDD should undergo spinal instrumentation surgery either PLF or PLIF as per the requirement as these surgeries provide good clinical and radiological outcomes in terms of pain, disability index, LLA, and maintenance of DSH. Although both the groups have few degrees of risks and complications, these are not major one and can be managed easily. The fusion rates are similar in both the groups (PLF and PLIF). Quality of life index showed significant difference within 1 week, after 3 months, and after 6 months of surgery in all of our patients.
#
Key-words:
Degenerative disc disease - lumbar lordotic angle - Oswestry disability index - posterior lumbar interbody fusion - posterolateral fusion - quality of life score - transforaminal lumbar interbody fusion - visual analog scaleIntroduction
Low back pain is a common disorder affecting approximately 80% of the population.[[1]] Degenerative lumbar spine disc disease is a common cause of disabling pain which most of the people encounter sometime in their life. Many a time, it requires intervention. There are different types of symptoms and signs such as chronic low back pain, sciatic pain, paresthesia, weakness, disturbance of sphincters, and intermittent claudication seen in lumbar degenerative disc disease (DDD).
In DDD, there is progressive deterioration of the structures, wherein nuclear degeneration, nuclear prolapse (due to increased nuclear pressure under mechanical loads), nuclear fibrosis, disc resorption, loss of disc space, and osteophyte formation occur. There are also facet joint abnormalities, spondylolisthesis, and hypertrophy of ligamentum flavum.
Objectives of the study
Primary objective
-
To compare the clinical and radiological outcome of the mentioned surgical techniques – posterior or transforaminal lumbar interbody fusion (PLIF/TLIF) with posterolateral fusion (PLF) used to deal with lumbar degenerative spine diseases.
#
Secondary objectives
-
To assess the quality of life pre- and post-operatively in all patients
-
To compare quality of life in both groups.
#
#
#
Materials and Methods
Ours is a prospective, nonrandomized, analytic, comparative study, i.e., a quasi-experimental study on clinical and radiological outcome of the patients who underwent posterolateral fusion (PLF) and PLIF/TLIF) at the Neurosurgery Department of Max Super Specialty Hospital, West Block 1, Press Enclave Road, Saket, New Delhi - 110 017, between July 2016 and December 2017 with 6 months of follow-up, and the surgery was performed by anyone of the senior neurosurgeons who were part of the study.
Inclusion criteria
-
Patients aged 30–65 years (male or female)
-
Patients with at least 6 months duration of low back pain with or without leg pain
-
Patients with disc degenerative disease, with or without disc hernia
-
Patients with degenerative spondylolisthesis with neurological symptoms
-
Symptomatic patients with the history of previous lumbar noninstrumental spine surgery
-
Patients with lumbar canal stenosis involving one or more disc levels.
#
Exclusion criteria
-
Patients who have severe osteoporosis (T score-2.5 or lower),
-
Patient having infection
-
Patient with underlying malignancyPatient with psychosocial/behavioral disorders
-
Patients with drug abuse
-
Patients with previous instrumented spine surgery
-
Patients with spinal fractures.
Preoperative variables included age, sex, medical history, clinical findings, ratio of disc space height (DSH) and immediate superior vertebral body height, level involved, lumbar canal diameter, grade of lumbar intervertebral disc degeneration, visual analog scale for pain, Oswestry disability score,[[2]] and quality of life score (QOLS) (EQ-5D-5L).[[3]]
Patients were counseled in their native language regarding their role in the study with respect to evaluating the pre- and post-operative pain, disability, and QOLSs.
Indications for surgery were neurogenic claudication, neurological deficits, degenerated disc with severe persistent backache, high-grade slip with instability, and back pain not relieved by conservative treatment.
Patients underwent two types of spinal fusion surgeries: PLF and PLIF, and those two groups were compared for clinicoradiological outcome, successful fusion, and quality of life at 6 months of follow-up.
#
Study population
We included a total of 100 (30–65 years of age) who presented with DDD, met our inclusion criteria, and were admitted for spinal fusion surgeries (PLF/PLIF).
#
Sample size
The surrogate use for fusion was return to work. The reason that we have used this for the calculation of sample size is because Aygün et al. in 2014[[4]] have reported this for comparing PLF group with PLIF group. They reported that the percentage of return to work in these two groups is 63% and 87%, respectively. The difference thus is 24%. To be able to detect this kind of difference with 80% power and 5% level of significance, the sample size comes to 50. Hence, we proposed to cover these many cases (50) in each group in our study. We have used the following formula:

Zα/2= 1.96 corresponding to 5% level of significance
Zβ=0.84 corresponding to 80% power
Delta = Difference to be detected.
#
Data collection technique and tools
Preoperative variables were recorded including age, sex, medical history, clinical findings, and type and grade of spondylolisthesis. Patients were taken into confidence after explaining the procedure and counseled in their native language regarding their role in the study with respect to evaluating the pre- and post-operative pain evaluation.
Visual analog scale (VAS) and the modified-Oswestry low back pain disability questionnaire provided a clinical assessment before the surgery, within a week after surgery and 3 months and 6 months after the surgery.
For radiological evaluation, X-ray films including anterior-posterior and lateral (neutral, flexion, and extension) were done both pre- and post-operatively (within 1 week and at 3 months).
The DSH and the whole lumbar lordotic angle (LLA) before surgery, within 1 week after surgery, and 3 months after surgery were analyzed.
For the whole LLA, the angle formed by the upper endplate of the L1 vertebral body and the upper endplate of the S1 vertebral body was measured [[Figure 1]]a.

The DSH was measured by the distance connecting the line drawn on the upper and lower endplates of the fusion segment and the center of the superior and inferior endplates. Intervertebral disc height measurements were calculated as the ratio between disc height and height of the immediately superior vertebral body. Measurements were done in the neutral position directly from plane lateral lumbar radiographs. Calculation of a ratio in this fashion obviates technical differences between plane films performed at different times, which might influence absolute measurements. The technique assumes that an individual's vertebral body height remains constant [[Figure 1]]b.
Lumbar disc degeneration was seen in the T2-weighted image of magnetic resonance imaging and is classified as per the Pfirrmann classification [[Table 1]].[[5]]

At 6 months of follow-up, patients got the computed tomography (CT) scan done for lumbosacral spine, and the assessment was done according to the classifications as already described in the review of literature, i.e., Brantigan, Steffee, Fraser (BSF)[[6]] for interbody fusion and Lenke's classification for posterolateral fusion.
#
Brantigan, Steffee, Fraser classification of posterior lumbar interbody fusion success [[Figure 2]]
Brantigan, Steffee, Fraser-1
Radiographical pseudarthrosis is indicated by collapse of the construct, loss of disc height, vertebral slip, broken screws, displacement of the carbon cage, or significant resorption of the bone graft, or lucency visible around the periphery of the graft or cage.

#
Brantigan, Steffee, Fraser-2
Radiographical-locked pseudarthrosis is indicated by lucency visible in the middle of the cages with solid bone growing into the cage from each vertebral endplate.
#
Brantigan, Steffee, Fraser-3
Radiographical fusion
Bone bridges at least half of the fusion area with at least the density originally achieved at the surgery. Radiographical fusion through one cage (half of the fusion area) is considered to be mechanically solid fusion even if there is lucency on the opposite side.
#
#
#
Lenke's classification of posterolateral fusion success [[Figure 3]]
-
Grade A – Definitely solid with bilateral trabeculated stout fusion masses present
-
Grade B – Possibly solid with a unilateral large fusion mass and a contralateral small fusion mass
-
Grade C – Probably not solid with a small fusion mass bilaterally
-
Grade D – Definitely not solid with bone graft resorption or obvious pseudarthrosis bilaterally.

We evaluated the quality of life of the patients at the time of admission, within 1 week, 3 months, and 6 months postoperatively. We used EQ-5D-5L health questionnaire as well as EQ-VAS for this evaluation.
#
Data analysis
Results were analyzed statistically using Statistical Package for the social sciences software version 21.0 (IBM, Armonk, NewYork, United States, US) and presented in terms of frequency, percentage, mean, and standard deviation. Measurements were compared between groups using the Student's t-test (independent and paired) for normally distributed variables. Percentage was compared with Chi-square test in various parameters. Statistical significance was determined with P values; P < 0.05 was considered statistically significant.
#
#
Results
Demographic profile
Age distribution
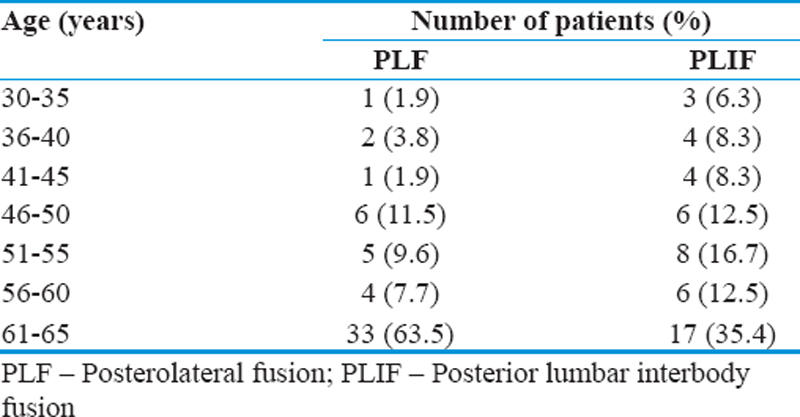
In our study, we included patients aged 30–65 years. Patients of age group 61–65 years are more in both groups – 33, i.e., 63% in PLF (n = 52) and 17, i.e., 35.4% in PLIF (n = 48) group. The age distribution among the groups is not statistically significant (P = 0.146) [[Table 2]].
#
Sex distribution
Overall female patients were more than the male patients (55% vs. 45%) suffering from lumbar DDD. More female patients underwent PLF surgery, i.e., 67.3%, while male patients were more to undergo PLIF surgery, i.e., 58.3%. When compared the two groups, the difference was statistically significant (P = 0.01) [[Table 3]].

#
#
Preoperative assessment
All of our patients had a history of low back pain, but 27% of patients presented with leg pain along with low backache (LBA), 58% of our patients also gave a history of sensory symptoms such as numbness/tingling sensation/paresthesias which hampered their daily activities, and only 5% of the patients had bladder bowel involvement.
#
Operative parameters
Vertebral levels involved and operated
When we see the distribution of vertebral levels involved in our patients, we found that L4–5 level was involved the most, i.e., 24%, followed by L5–S1 (21%), L3–L5 (20%), and L4–S1 (15%). Our PLF patients were operated more at L3–L5 (38.4%) followed by L4–S1 (28.8%) levels while PLIF patients were more operated at L4–5 level (50%) followed by L5–S1 (43.75%) level. Thus, we can say that DDD involves lower lumbar levels more (L3–S1) [[Table 4]].

#
Number of vertebral levels operated
In our study, single level was operated (49%) most followed by 2 (36%) and 3 (15%) levels. All intervertebral body fusions were done at single level.
#
Operation time
In our study, we found that in the PLF group, most of the patients were operated for 2 or 3 vertebral levels, while all the patients among the PLIF group were operated for single level. Although the operation time in the PLF group for level 2 and 3 was 239.86 ± 60.51 and 269.33 ± 60.76 min, respectively, which was more than the PLIF group operated for single level, i.e., 208.44 ± 54.90, the difference is not significant. However, only one patient in the PLF group operated for single level and the operation time was 180 ± 0 [[Table 5]].

#
Intraoperative blood loss
In our study, most of the patients in two groups had intraoperative blood loss under 500 ml. Of these two groups, PLF group patients had more incidence of intraoperative blood transfusion (13, i.e., 25%) as compared to PLIF group (3, i.e., 6.3%) and this difference is statistically significant as P value comes to 0.011. However, we have already seen in our previous results that all the patients in PLIF group were operated for single level, but PLF group patients were also operated for 2 and 3 levels which may require more incidence of blood transfusion during the procedure.
#
Complications
We observed in our study that intraoperative complications were far more among the PLF group patients as compared to the PLIF group. Using Chi-square test, we found that there was statistically significant difference between two groups in intraoperative complications (P = 0.011) while early and delayed postoperative complications among the groups had no statistically significant difference (P = 0.199 and 0.345, respectively). In PLF group patients who had intraoperative complications had prolong history, more number of levels was involved which leads to much more adhesions and thinning of dura, and intraoperatively, the incidence of inadvertent dural tear occurred which was managed by dural repair, but only one patient had CSF leak in the postoperative period and was managed with re-exploration. In the early postoperative period, i.e., within 1 month of operation, two patients of PLF group required re-exploration and readjustment of one or two pedicle screws. One patient among PLIF group had radiculopathy after 1½ months of operation and later required adjacent level microdiscectomy. Rest of the patients had surgical site wound infections, and most of them were managed conservatively, but five of them required re-exploration and resuturing [[Table 6]].

#
Clinical outcome
We observed after 1 week, 3 months, and 6 months postoperatively that all of our patients had statistically significant clinical improvement in terms of pain (P = 0.000, 0.009, and 0.004, respectively) and disability index (P = 0.000, 0.000, and 0.000, respectively). Paired t-test was used to get the given results [[Table 7]] and [[Table 8]] [[Figure 4]]a and [[Figure 4]]b.



#
#
Radiological outcome
Lumbar lordotic angle
In our study, we found statistically significant difference in LLA in X-ray of the lumbosacral spine. Paired t-test was used to get the results and P value was found to be 0.000 at 1 week and 3 months of follow-up.
#
Placement of implants
All of our patients had proper placement of screws with length >2/3 and proper placement of cage except two patients, which we already discussed under early postoperative complications had misplaced screws. They were managed by re-exploration and readjustment of screws.
#
Ratio of disc space height and height of immediate superior vertebral body
Ratio of DSH and immediate superior vertebral body was increased at all levels within 1 week and at 3 months postsurgery with P = 0.000 and 0.000, respectively. Paired t-test was used to get the given results.
#
Fusion grade
At 6 months of follow-up, we assessed the patients with CT scan and BSF Grade 3 was labeled as successful fusion in PLIF group and patients with Lenke's Grade A and B were labeled as successful fusion in PLF group patients, while patients with BSF Grade 1 and 2 in the PLIF group and Lenke's Grade C and D were labeled as unsuccessful fusion. We found that the successful fusion was more among the PLIF group patients, i.e., 81.25%, than the PLF group patients, i.e., 67.30%, although there was no statistically significant difference among the two groups as P value was 0.112 [[Table 9]] [[Figure 5]]a and [[Figure 5]]b.


#
Quality of life
We assessed the QOLS in all patients at the time of admission, within 1 week after operation, after 3 months of operation, and at 6 months after operation. We analyzed our data using paired t-test to find the mean value and standard deviation. After analysis, we found that there was statistically significant difference in the score at all three times (P = 0.000 in all) as compared to score in the preoperative period [[Table 10]].

#
#
#
Discussion
Chronic LBA is one of the most common problems that the patient presents with to the outpatient. With changing lifestyle, sedentary work, and aging population, more and more patients are presenting with chronic LBA.
Recent advances in spine surgeries for degenerative spine diseases have shown reasonable pain relief and functional outcome of the patient. Although interbody fusion by conventional posterior approach is widely practiced, there is higher incidence of several complications resulting from severe muscle damage and blood loss due to the dissection and retraction of broad muscular and soft tissues.
Literature points out the fact the PLIF is superior to PLF in DSH maintenance and demonstrates a tendency toward higher fusion rates, but the results are not statistically significant. Despite a large number of publications of outcomes after spinal fusion surgery, there is still no consensus on the efficacy of several different fusion methods. The data to support an improved outcome with interbody fusion as compared with PLF are scarce. There are less data comparing the clinicoradiological outcome of interbody fusion (PLIF/TLIF) versus posterolateral fusion (PLF). Most of the studies are retrospective, while very few are prospective studies comparing clinicoradiological outcome after spinal fusion surgeries (PLF vs. PLIF). None of the study is assessing and comparing the quality of life in spinal fusion cases.
In this study, we have compared the clinical and radiological parameters in patients who underwent spinal fusion surgeries (PLF vs. PLIF/TLIF). We also assessed and compared the quality of life in two different groups.
We compared our study with the literature as shown in [[Table 11]].

Comparison of our study with the previous literature
Thus, we found that most of the previous literature includes retrospective studies or review and meta-analysis, while our study is a prospective nonrandomized study with a sample size of 100 patients. Like other studies, our patients who underwent ≤3 vertebral levels operated showed no statistically significant difference in operation time, blood loss, early and delayed postoperative complications, with significant difference in intraoperative complications among two groups (P = 0.011), but those patients had prolonged history with more number of vertebral level involvement which lead to much more adhesions and thinning of dura causing inadvertent dural tear at the time of neural decompression not at the time of instrumentation. Those complications were managed by dural repair intraoperatively except one case required postoperative re-exploration and repair. Global outcome assessment in terms of VAS score, Oswestry disability index score, improvement in ratio of DSH/height of immediate superior vertebral body, and lumbar lordosis angle (LLA) was good in all of our patients, and there was no statistically significant difference among the two groups. Fusion rates were 67.3% in the PLF while 81.3% in the PLIF group, but this difference was not statistically significant as P = 0.112. None of the previous study assessed the QOLS while we assessed as well as compared and found that QOLS improved significantly at 6 months of follow-up when compared with preoperative score as P value comes 0.000, but there was no significant difference if compared among the two groups.
#
#
Conclusions
We concluded from our study and after the review of literature that the patients with lumbar DDD should undergo spinal instrumentation surgery either PLF or PLIF as per the requirement as these surgeries provide good clinical and radiological outcomes in terms of pain, disability index, LLA, and maintenance of DSH; although both the groups have few degree of risks and complications, these are not major one and can be managed easily. The fusion rates are similar in both the groups (PLF and PLIF). Quality of life index showed significant difference within 1 week, after 3 months, and after 6 months of surgery in all of our patients.
Recommendations
At present, spinal instrumentation surgeries give good clinicoradiological outcome to the patients suffering from DDD and improve their quality of life.
#
#
#
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Kelsey JL, White AA 3rd. Epidemiology and impact of low-back pain. Spine (Phila Pa 1976) 1980;5:133-42.
- 2 Fairbank JC, Pynsent PB. The Oswestry disability index. Spine (Phila PA 1976) 2000;25:2940-52.
- 3 Oemar M. EQ-5D-5L User Guide Version 2.0; 2013.
- 4 Aygün H, Cakar A, Hüseyinoǧlu N, Hüseyinoǧlu U, Celik R. Clinical and radiological comparison of posterolateral fusion and posterior interbody fusion techniques for multilevel lumbar spinal stabilization in manual workers. Asian Spine J 2014;8:571-80.
- 5 Naderi S, Benzel EC. Spine Surgery-Techniques, Complication Avoidance and Management. History of Spine Surgery. 3rd ed., Vol. 13. Ch. 1. p. 123.
- 6 Brantigan JW, Steffee AD. A carbon fiber implant to aid interbody lumbar fusion. Two-year clinical results in the first 26 patients. Spine (Phila Pa 1976) 1993;18:2106-7.
- 7 Lidar Z, Beaumont A, Lifshutz J, Maiman DJ. Clinical and radiological relationship between posterior lumbar interbody fusion and posterolateral lumbar fusion. Surg Neurol 2005;64:303-8.8
- 8 Cheng L, Nie L, Zhang L. Posterior lumbar interbody fusion versus posterolateral fusion in spondylolisthesis: A prospective controlled study in the Han nationality. Int Orthop 2009;33:1043-7.
- 9 Wu Y, Tang H, Li Z, Zhang Q, Shi Z. Outcome of posterior lumbar interbody fusion versus posterolateral fusion in lumbar degenerative disease. J Clin Neurosci 2011;18:780-3.
- 10 Høy K, Bünger C, Niederman B, Helmig P, Hansen Es, Li H, et al. Transforaminal lumbar interbody fusion (TLIF) versus posterolateral instrumented fusion (PLF) in degenerative lumbar disorders: A randomized clinical trial with 2-year follow-up. Eur Spine j 2013;22:2022-9.
- 11 Woo Lee G. Comparison of posterolateral lumbar fusion and posterior lumbar. Spine 2014;39:e1475-80.
- 12 Al Barbarawi Mm, Audat Zm, Allouh MZ. Analytical comparison study of the clinical and radiological outcome of spine fixation using posterolateral, posterior lumber interbody and transforaminal lumber interbody spinal fixation techniques to treat lumber spine degenerative disc disease. Scoliosis 2015;10:17.
- 13 Jalalpour K, Neumann P, Johansson C, Hedlund R. A randomized controlled trial comparing transforaminal lumbar interbody fusion and uninstrumented posterolateral fusion in the degenerative lumbar spine. Global Spine J 2015;5:322-8.
- 14 Luo J, Cao K, Yu T, Li L, Huang S, Gong M, et al. Comparison of posterior lumbar interbody fusion versus posterolateral fusion for the treatment of isthmic spondylolisthesis. Clin Spine Surg 2017;30:e915-22.
- 15 Campbell R. Posterolateral versus interbody fusion. Global Spine J 2017;7:482-90.
- 16 Makanji H, Schoenfeld AJ, Bhalla A, Bono CM. Critical analysis of trends in lumbar fusion for degenerative disorders revisited: Influence of technique on fusion rate and clinical outcomes. Eur Spine J 2018;27:1868-76.
Address for correspondence
Publikationsverlauf
Eingereicht: 24. September 2019
Angenommen: 20. Februar 2020
Artikel online veröffentlicht:
16. August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Kelsey JL, White AA 3rd. Epidemiology and impact of low-back pain. Spine (Phila Pa 1976) 1980;5:133-42.
- 2 Fairbank JC, Pynsent PB. The Oswestry disability index. Spine (Phila PA 1976) 2000;25:2940-52.
- 3 Oemar M. EQ-5D-5L User Guide Version 2.0; 2013.
- 4 Aygün H, Cakar A, Hüseyinoǧlu N, Hüseyinoǧlu U, Celik R. Clinical and radiological comparison of posterolateral fusion and posterior interbody fusion techniques for multilevel lumbar spinal stabilization in manual workers. Asian Spine J 2014;8:571-80.
- 5 Naderi S, Benzel EC. Spine Surgery-Techniques, Complication Avoidance and Management. History of Spine Surgery. 3rd ed., Vol. 13. Ch. 1. p. 123.
- 6 Brantigan JW, Steffee AD. A carbon fiber implant to aid interbody lumbar fusion. Two-year clinical results in the first 26 patients. Spine (Phila Pa 1976) 1993;18:2106-7.
- 7 Lidar Z, Beaumont A, Lifshutz J, Maiman DJ. Clinical and radiological relationship between posterior lumbar interbody fusion and posterolateral lumbar fusion. Surg Neurol 2005;64:303-8.8
- 8 Cheng L, Nie L, Zhang L. Posterior lumbar interbody fusion versus posterolateral fusion in spondylolisthesis: A prospective controlled study in the Han nationality. Int Orthop 2009;33:1043-7.
- 9 Wu Y, Tang H, Li Z, Zhang Q, Shi Z. Outcome of posterior lumbar interbody fusion versus posterolateral fusion in lumbar degenerative disease. J Clin Neurosci 2011;18:780-3.
- 10 Høy K, Bünger C, Niederman B, Helmig P, Hansen Es, Li H, et al. Transforaminal lumbar interbody fusion (TLIF) versus posterolateral instrumented fusion (PLF) in degenerative lumbar disorders: A randomized clinical trial with 2-year follow-up. Eur Spine j 2013;22:2022-9.
- 11 Woo Lee G. Comparison of posterolateral lumbar fusion and posterior lumbar. Spine 2014;39:e1475-80.
- 12 Al Barbarawi Mm, Audat Zm, Allouh MZ. Analytical comparison study of the clinical and radiological outcome of spine fixation using posterolateral, posterior lumber interbody and transforaminal lumber interbody spinal fixation techniques to treat lumber spine degenerative disc disease. Scoliosis 2015;10:17.
- 13 Jalalpour K, Neumann P, Johansson C, Hedlund R. A randomized controlled trial comparing transforaminal lumbar interbody fusion and uninstrumented posterolateral fusion in the degenerative lumbar spine. Global Spine J 2015;5:322-8.
- 14 Luo J, Cao K, Yu T, Li L, Huang S, Gong M, et al. Comparison of posterior lumbar interbody fusion versus posterolateral fusion for the treatment of isthmic spondylolisthesis. Clin Spine Surg 2017;30:e915-22.
- 15 Campbell R. Posterolateral versus interbody fusion. Global Spine J 2017;7:482-90.
- 16 Makanji H, Schoenfeld AJ, Bhalla A, Bono CM. Critical analysis of trends in lumbar fusion for degenerative disorders revisited: Influence of technique on fusion rate and clinical outcomes. Eur Spine J 2018;27:1868-76.