

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_80_19
Gangliocytic paraganglioma of dorsolumbar spine: A rare tumor at rare site
Authors

Spinal paragangliomas are rare benign tumors. The gangliocytic paragangliomas (GP) of spine are even rarer. The GPs are almost exclusively seen in duodenum. In spine, the usual site of affection is cauda equina region. The involvement of other spinal levels is far less often and includes thoracic and cervical region. We report this case of GP involving the conus medullaris region and reaching up to the upper part of cauda equina. The prognosis of spinal GP is excellent after total excision, as it is classified under WHO Grade I tumor. The patient made a full recovery after tumor removal. Clinical, radiological, and pathological characteristics of this rare tumor are discussed here along with.
Introduction
Gangliocytic paraganglioma (GP) was first reported in 1957 as ganglioneuroma by Dahl et al.[[1]] and named as GP by Kepes and Zacharias in 1971.[[2]] It is a rare, encapsulated, slow growing, benign tumor; having rare malignant potential with tendency to metastasize to regional lymph nodes. They are almost exclusively seen in the second part of duodenum.[[3]] GPs of the spine are extremely rare, where cauda equina is the most common site,[[4]] (conus-cauda region). In the present case, the tumor was localized at the level of conus medullaris extending up to the beginning of cauda equina, in dorsolumber region (D12 to upper margin of L2). GP has generally been regarded as a neuroendocrine tumor and with histomorphological features of paraganglioma with mature ganglion cells.
Case Report
A 42-year-old male patient presented with difficulty in walking since 15 days, pain and tingling sensation in the right leg since 6 months. The symptoms aggravated in night and were relieved after taking rest. No bowel or bladder complaints were reported. There was no previous history of hospitalization for any medical or surgical illness. The neurological evaluation showed decreased motor power of right lower limb with no sensory deficits.
Magnetic resonance imaging findings
An isodense, heterogeneous, intradural, extramedullary, enhancing mass lesion extending from lower margin of D12 to upper margin of L2 vertebra, at the level of conus medullaris extending up to the beginning of cauda equina was noted [[Figure 1]]a and [[Figure 1]]b. No evidence of extraspinal invasion was seen. As the lesion was extramedullary and showed extension into the right neural foramina [[Figure 1]]c, radiological impression was kept as a neurogenic tumor-Schwannoma/ependymoma/meningioma/neurofibroma. The clinical diagnosis was also kept the same.

Intraoperative
Tumor was identified to be intradural, extramedullary with no extension in surrounding extraspinal, paravertebral soft tissue. Laminectomy and excision of tumor followed by duroplasty was done. Excised tumor was submitted for histopathology.
Morphology
Multiple gray white tissue bits aggregating to 3 cm × 2.5 cm × 2 cm were received. Histopathological examination showed a capsulated tumor [[Figure 2]]a comprising of three distinct types of cell populations.

Predominant cells were tumor cells (neuroendocrine cells) which were small, round to polygonal, with pale eosinophilic cytoplasm, round to oval nuclei, stippled chromatin, forming solid nests, and trabeculae [[Figure 2]]b.
Ganglion cells having irregular contour, abundant cytoplasm, large vesicular nuclei with prominent nucleoli; were seen scattered and intermingled with neuroendocrine cells [[Figure 2]]b.
Spindle (interstitial) cells, representing Schwann cells, were present along with branching vascular channels forming fine delicate network around the predominant cell type-giving rise to zellballen pattern [[Figure 3]]a and [[Figure 3]]b.

No evidence of pleomorphism, hyperchromasia, mitotic activity, and necrosis was noted.
Thus, the provisional histopathological diagnosis of “GP” was given.
Immunohistochemistry
The tumor cells showed diffuse immunohistochemical expression of chromogranin, synaptophysin and neuron-specific enolase (NSE) supporting neuroendocrine differentiation. Ganglion cells expressed NSE, along with chromogranin and synaptophysin. Spindle cells showed S-100 positivity. The findings proved the microscopic diagnosis.
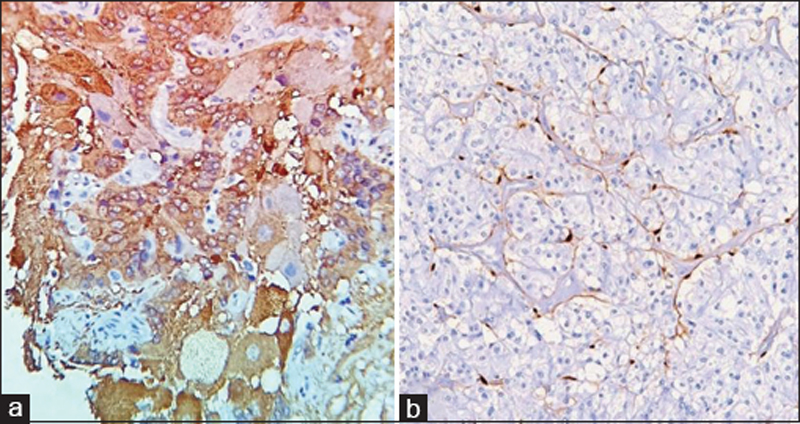
[[Figure 4]] and [[Figure 5]] show immunohistochemical staining for chromogranin [[Figure 4]]a, synaptophysin [[Figure 4]]b, and neuron-specific enolase NSE [[Figure 5]]a highlighting neuroendocrine and ganglion cell components. [[Figure 5]]b: Immunohistochemical staining for S-100 is positive in spindle/interstitial cells 400×, IHC.

Postoperative
The postoperative period was uneventful. Suture removal was done on 10th day. The patient was instructed to come every month for follow-up and third postoperative month for radiology (magnetic resonance imaging [MRI]). In spite of this, he came only once for check-up, i.e., 1 month postoperative, when he was clinically fine. After this, the patient was lost to follow-up.
Discussion
Spectrum of intradural extramedullary tumors of the peripheral nervous system within the spinal canal in adults includes-Schwannomas, ependymoma, neurofibromas, or solitary metastasis and to a lesser extent paragangliomas. About 85%–90% of paragangliomas arise from the adrenal gland. The extra-adrenal paragangliomas can also occur in the central nervous system (CNS), where they are usually observed in the carotid body and glomus jugulare, also some other unusual sites being pineal region, sella turcica, suprasellar region, or the orbit.[[1]] An uncommon localization is the spinal, where the incidence in the general population comes to be 0.07/100000 people.[[5]] Majority of spinal paragangliomas occur at cauda equina (conus-cauda region). Other spinal levels involved are thoracic and few in cervical region. Nearly mere 25% of the cauda equina paraganglioma show gangliocytic differentiation. The GP in the other spinal regions is even lesser.[[4]] The duodenum is the most common site of the GP, followed by the cauda equine of the spinal cord, respiratory system, jejunum, and esophagus. This case had localization at the level of conus medullaris extending up to the beginning of cauda equina, in dorsolumber region (D12 – upper margin of L2). The histological differential diagnosis considered was an ependymoma, which has a poor prognosis. The distinctive triphasic appearance on histopathology essentially excluded the other possibilities.
Histogenesis
The GP of the spine is considered to originate from neural crest cells which give rise to sympathoadrenal lineage, afterward undergoing divergent differentiation to form neuroendocrine and ganglion cell components.[[6]] Some authors have proposed that these lesions represent a hamartomatous proliferation when in duodenum, perhaps originating from different embryonal layers during the formation and migration of the pancreatic primordia.[[7]],[[8]],[[9]] It is based on the diversity of the elements composing GP. However, the fact that few of them have undergone malignant transformation with lymph node metastases argues in favor of a true neoplastic nature.[[10]]
The presenting complaints of spinal GPs are usually lumbar pain, motor or sensory loss in lower extremities, or bowel and bladder dysfunction. The MRI of intradural extramedullary lesions shows a similar image profile, thus making histologic examination the key to diagnosis. The usual management of this tumor is surgical resection. When the lesions are placed in the junction areas, such as present case, laminotomy is preferred over laminectomy, considering the motion segments, and potential for the development of instability in the future. Adjuvant radiotherapy should be reserved for unencapsulated or incompletely excised lesions as it does not guarantee the prevention of tumor recurrence. However, follow-up in the form of clinical examination every month after the operative procedure till 6 months followed by every 6 months, and a radiological examination MRI at 3rd postoperative month followed by every 6 months is recommended.
Conclusion
This case of GP, localized in dorsolumber region, was seen at the level of conus medullaris extending up to the beginning of cauda equina. Their origin in CNS is still unclear. In view of rarity, a long-term follow-up and assessment of molecular pathogenesis are essential for therapeutic intervention, biological behavior, and monitoring the outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Dahl EV, Waugh JM, Dahlin DC. Gastrointestinal ganglioneuromas; brief review with report of a duodenal ganglioneuroma. Am J Pathol 1957;33:953-65.
- 2 Kepes JJ, Zacharias DL. Gangliocytic paragangliomas of the duodenum. A report of two cases with light and electron microscopic examination. Cancer 1971;27:61-7.
- 3 Kwon J, Lee SE, Kang MJ, Jang JY, Kim SW. A case of gangliocytic paraganglioma in the ampulla of vater. World J Surg Oncol 2010;8:42.
- 4 Landi A, Mancarella C, Marotta N, Tarantino R, Lenzi J. Diagnosis and treatment of paragangliomas of the filum terminale, an extremely rare entity: Personal experience and literature review. J Spine 2013;S3:e001.
- 5 Landi A, Tarantino R, Marotta N, Rocco P, Antonelli M, Salvati M, et al. Paraganglioma of the filum terminale: Case report. World J Surg Oncol 2009;7:95.
- 6 Shankar GM, Chen L, Kim AH, Ross GL, Folkerth RD, Friedlander RM. Composite ganglioneuroma-paraganglioma of the filum terminale. J Neurosurg Spine 2010;12:709-13.
- 7 Guarda LA, Ordonez NG, del Junco GW, Luna MA. Gangliocytic paraganglioma of the duodenum: An immunocytochemical study. Am J Gastroenterol 1983;78:794-8.
- 8 Perrone T, Sibley RK, Rosai J. Duodenal gangliocytic paraganglioma. An immunohistochemical and ultrastructural study and a hypothesis concerning its origin. Am J Surg Pathol 1985;9:31-41.
- 9 Burke AP, Helwig EB. Gangliocytic paraganglioma. Am J Clin Pathol 1989;92:1-9.
- 10 Okubo Y, Wakayama M, Nemoto T, Kitahara K, Nakayama H, Shibuya K, et al. Literature survey on epidemiology and pathology of gangliocytic paraganglioma. BMC Cancer 2011;11:187.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Dahl EV, Waugh JM, Dahlin DC. Gastrointestinal ganglioneuromas; brief review with report of a duodenal ganglioneuroma. Am J Pathol 1957;33:953-65.
- 2 Kepes JJ, Zacharias DL. Gangliocytic paragangliomas of the duodenum. A report of two cases with light and electron microscopic examination. Cancer 1971;27:61-7.
- 3 Kwon J, Lee SE, Kang MJ, Jang JY, Kim SW. A case of gangliocytic paraganglioma in the ampulla of vater. World J Surg Oncol 2010;8:42.
- 4 Landi A, Mancarella C, Marotta N, Tarantino R, Lenzi J. Diagnosis and treatment of paragangliomas of the filum terminale, an extremely rare entity: Personal experience and literature review. J Spine 2013;S3:e001.
- 5 Landi A, Tarantino R, Marotta N, Rocco P, Antonelli M, Salvati M, et al. Paraganglioma of the filum terminale: Case report. World J Surg Oncol 2009;7:95.
- 6 Shankar GM, Chen L, Kim AH, Ross GL, Folkerth RD, Friedlander RM. Composite ganglioneuroma-paraganglioma of the filum terminale. J Neurosurg Spine 2010;12:709-13.
- 7 Guarda LA, Ordonez NG, del Junco GW, Luna MA. Gangliocytic paraganglioma of the duodenum: An immunocytochemical study. Am J Gastroenterol 1983;78:794-8.
- 8 Perrone T, Sibley RK, Rosai J. Duodenal gangliocytic paraganglioma. An immunohistochemical and ultrastructural study and a hypothesis concerning its origin. Am J Surg Pathol 1985;9:31-41.
- 9 Burke AP, Helwig EB. Gangliocytic paraganglioma. Am J Clin Pathol 1989;92:1-9.
- 10 Okubo Y, Wakayama M, Nemoto T, Kitahara K, Nakayama H, Shibuya K, et al. Literature survey on epidemiology and pathology of gangliocytic paraganglioma. BMC Cancer 2011;11:187.