
Subscribe to RSS
DOI: 10.4103/ajns.AJNS_51_21
Spinal intradural extramedullary capillary hemangioma with coexistent spinal edema and syringomyelia successfully treated by tumor removal and cervical laminoplasty
Capillary hemangioma (CH) is usually found in pediatric patients and is located in soft tissue of the neck or head. As uncommon location of CH, spinal intradural extramedullary space has been reported; however, coexistent spinal edema or syringomyelia with spinal intradural extramedullary CH seems rare manifestations on preoperative magnetic resonance imaging. Laminectomy and tumor resection have been often performed for spinal intradural extramedullary CH. An 83-year-old man was referred to our hospital, complaining of nocturia and motor weakness of the lower extremities. Magnetic resonance imaging revealed a mass at the level of T1, which was homogeneously enhanced on gadolinium-enhanced T1-weighted images. The lesion was accompanied by spinal edema and syringomyelia. An intradural extramedullary tumor was first considered. We thought that the coexistent spinal edema and syringomyelia could have been caused by spinal stenosis. Preoperative angiography revealed that the mass was fed by the radicular artery of C5–C6. To improve the clinical symptoms of the patient, tumor removal and cervical laminoplasty were performed. The spinal edema and syringomyelia regressed postoperatively. The histopathological diagnosis was CH. This is the first reported case of cervical intradural extramedullary CH with spinal edema and syringomyelia successfully treated by cervical laminoplasty and tumor removal.
#
Key-words:
Angiography - intradural extramedullary capillary hemangioma - laminoplasty - spinal edema - syringomyelia - tumor removalIntroduction
Capillary hemangioma (CH), a benign vascular tumor, is mostly found in the soft tissue of the head and neck such as skin, subcutaneous, or mucosal tissue in pediatric cases.[[1]],[[2]] Spinal intradural extramedullary CH has been previously reported, but this entity is still considered to be rare.[[3]],[[4]],[[5]],[[6]] Radiculopathy or myelopathy can result from the occupation of the spinal canal space by spinal CH.[[4]],[[7]] Spinal intradural extramedullary CH shows varying intensity on T1- and T2-weighted magnetic resonance imaging (MRI) but usually demonstrates strong homogeneous enhancement with gadolinium contrast agent.[[4]] Coexistent spinal edema or syringomyelia with spinal intradural extramedullary CH has been previously described; however, the reported cases are still limited.[[8]],[[9]],[[10]],[[11]],[[12]]
Regarding to surgical treatment for spinal intradural extramedullary CH, laminectomy and tumor resection seem to be usually performed.[[4]] To the best of our knowledge, there has not been mentioned any case of spinal intradural extramedullary CH with coexistent spinal edema and syringomyelia successfully treated laminoplasty and tumor resection.[[8]],[[9]],[[10]],[[12]],[[13]]
Here, we report a rare case of cervical intradural extramedullary CH accompanied by spinal edema and syringomyelia treated with laminoplasty and tumor resection.
#
Case Report
An 83-year-old man was introduced to our department of neurosurgery. The patient was complaining of motor weakness of the bilateral lower extremities, which had gradually worsened. The motor weakness was observed mostly in the right leg and resulted in gait disturbance. The patient also mentioned numbness of the bilateral lower extremities, and thermal nociception was dull under the bilateral inguinal region. The muscle tendon reflex of the lower extremities was bilaterally exacerbated, and Babinski reflex was positive. The patient was bothered by nocturia as well.
We first suspected lumbar spinal canal stenosis. MRI revealed, however, a lesion at the level of T1, which was homogeneously enhanced on gadolinium-enhanced T1-weighted image [[Figure 1]]a and [[Figure 1]]b. The lesion was accompanied by spinal edema spreading from C1 to T8 and syringomyelia from the C5 to T6 [[Figure 1]]c,[[Figure 1]]d,[[Figure 1]]e. There were no findings of flow voids. The lesion was first considered an intradural extramedullary tumor, such as a meningioma or schwannoma. We thought that the coexistent spinal edema and syringomyelia could have resulted from cervical spinal stenosis. Therefore, we planned tumor removal and cervical laminoplasty. To evaluate the vascularity of the tumor, computed tomography angiography (CTA) was performed. The lesion seemed to be fed by the radicular artery of C5–C6 and drain to the venous plexus [[Figure 1]]f. On cerebral angiography performed for further examination of the tumor vascularity, the right radicular artery of C5–C6 was recognized as a single feeder [[Figure 1]]g. The tumor was not fed by the left ascending cervical artery or the vertebral arteries.

After we performed CTA and cerebral angiography, we reconsidered that the lesion could be a vascular tumor. However, we did not think that we had to alter the surgical planning. Prior to the ooeration. We obtained informed consent from the oatient.
Operation
The patient was placed in the supine position. Transcranial motor-evoked potential was intraoperatively monitored. A 4-Fr sheath was inserted into the right femoral artery, and a catheter was introduced in the right radicular artery to inject intraoperatively indocyanine green. Mild heparinization was intraoperatively performed to avoid embolic complications. The patient was then set in the prone position. Following a midline skin incision and the detachment of the paraspinal muscle from the vertebrae at the level of C3–T1, the vertebral arch was opened, and the dura was exposed. The dura was medially opened, and then a mass was observed [[Figure 2]]a. The lesion was then evaluated with indocyanine green. The lesion was superficially enhanced after the feeder was visualized [[Figure 2]]b. The lesion was detached from the caudal side and partially thrombosed. The tumor was entirely detached from the spine and the feeder was finally cut [[Figure 2]]c. Intraoperative bleeding from the lesion did not occur. Indocyanine green was intra-arterially injected again, and we confirmed that the tumor was not apparently residual [[Figure 2]]d. Then, cervical laminoplasty was performed [[Figure 2]]e and [[Figure 2]]f. No remarkable change was observed in the motor-evoked potentials.

#
Postoperative course
Disappearance of the spinal edema and regression of syringomyelia were confirmed on postoperative MRI [[Figure 3]]. The patient's postoperative course was uneventful. Preoperative symptoms were resolved, and the patient was discharged from the hospital on postoperative day 15. He is now followed in an outpatient clinic. The spinal edema and syringomyelia disappeared without apparent recurrence of the vascular tumor on MRI performed 3 years and 2 months after the surgery [[Figure 4]].


#
Histopathological findings
On hematoxylin and eosin staining, the tumor was observed to be composed of a lobular aggregation of increased vessel epithelium. The tumor was partially enveloped by the meninges and hyalinized connective tissue. Nerve tissue was found along the outer margin of the tumor. Red blood cells were observed in the vessels. Immunohistologically, the tumor was positive for CD31, CD34, and αSAM. Any malignant findings were identified. These findings corresponded to CH [[Figure 5]].

#
#
Discussion
Here, we presented a rare case of spinal intradural extramedullary CH accompanied by spinal edema and syringomyelia. Our case was successfully treated with tumor removal and laminoplasty.
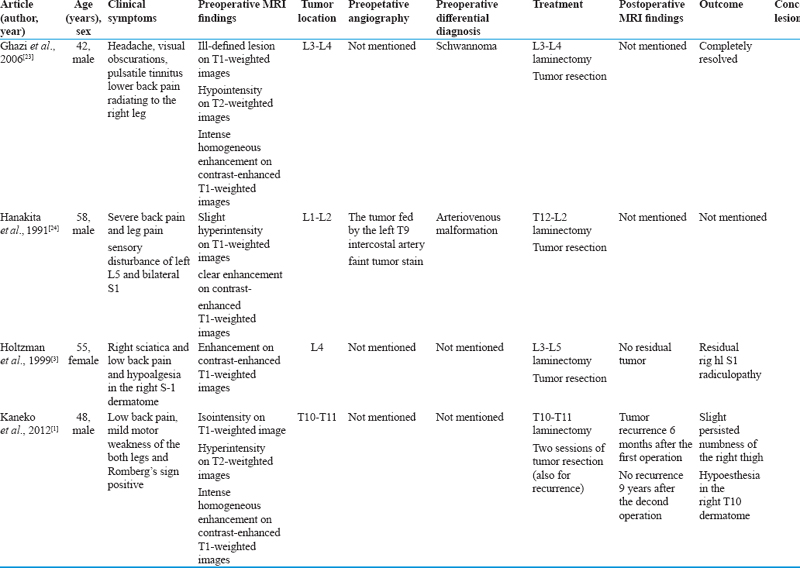
CH is generally found in pediatric cases.[[3]] The typical locations of CH are the skin, the subcutaneous tissue, or the mucosa in a head or neck lesion.[[3]],[[4]],[[5]],[[6]] When CH develops in the spine, CH is usually found in the vertebral body, and extraosseous lesions of the spine seem to be rare.[[14]] Spinal CH can be seen as an intradural extramedullary lesion when CH appears in the neuroaxis.[[4]],[[10]] Spinal intradural extramedullary CH with detailed description has been previously reported [[Table 1]].[[1]],[[3]],[[4]],[[6]],[[7]],[[8]],[[9]],[[10]],[[11]],[[12]],[[13]],[[15]],[[16]],[[17]],[[18]],[[19]],[[20]],[[21]],[[22]],[[23]],[[24]],[[25]],[[26]],[[27]],[[28]],[[29]],[[30]],[[31]],[[32]],[[33]],[[34]],[[35]],[[36]] An adult case of spinal intradural extramedullary CH was first reported by Hanakita et al.[[24]] The clinical symptoms related to spinal intradural extramedullary CH are chronic progressive myelopathy or radiculopathy resulting in motor or sensory deficits, though acute neurological aggravation due to intratumoral bleeding of intradural extramedullary CH has been reported.[[10]],[[31]],[[34]] Neurological deficits in our case were gradually progressing as typical manifestations of spinal intradural extramedullary CH.











Regarding the radiological features in our case, homogeneous enhancement of the tumor on gadolinium-enhanced T1-weighted MRI was observed. We first thought that the tumor was a common intradural extramedullary tumor such as meningioma or neurinoma, but a vascular tumor was successfully found on CTA and cervical angiography preoperatively performed to evaluate the vascularity of the tumor.
Spinal intradural extramedullary CH can show different intensities on T1-weighted or T2-weighted MRIs and shows strong homogeneous enhancement with gadolinium contrast agent.[[4]],[[7]],[[12]] Neurinoma or meningioma can also show strong enhancement on MRI, so neurinoma without cystic change or necrosis cannot be easily differentiated from spinal CH.[[7]] The dural tail sign, considered a typical feature of meningioma, cannot completely rule out spinal CH because spinal intradural extramedullary CH can arise from the inner surface of the dura mater.[[7]] Thus, MRI findings alone are not sufficient to differentiate spinal intradural extramedullary CH from neurinoma or meningioma. Preoperative angiography can be useful for preoperative possible diagnosis, as in our case. As we suspected a spinal vascular tumor, we intraoperatively evaluated the feeder and drainers of the tumor with indocyanine green injected through a catheter placed in the feeder. Intradural extramedullary vascular tumors need to be differentiated from arteriovenous malformations.[[7]] Due to the lack of flow void on preoperative MRI, arteriovenous malformation seemed not to be possible in our case. Hemangioendothelioma is reported to be rare, although it shows similar radiological findings on MRI to spinal CH.[[7]]
In addition to the radiological findings of spinal CH on MRI, the preoperative radiological findings, spinal edema and syringomyelia, are of interest in our case. Among the previously reported cases of spinal intradural extramedullary CH, coexistent spinal edema or syringomyelia was disclosed on preoperative MRI in five cases.[[8]],[[9]],[[10]],[[11]],[[12]] In the case reported by Lee et al., preoperative syringomyelia on the conus medullaris and arachnoiditis were confirmed on MRI.[[9]] Lee et al. speculated that the disturbed circulation of cerebrospinal fluid below spinal intradural extramedullary CH and possible minute bleeding from spinal intradural extramedullary CH could have been causative for syringomyelia and arachnoiditis.[[9]] In their case, preoperative syringomyelia on the conus medullaris and arachnoiditis aggravated even 1 year after the surgery on MRI. They discussed that intraoperative bleeding could have been responsible for the residual radiological findings.[[9]] Intraoperative bleeding should be avoided not to result in such complications. In our case, spinal intradural extramedullary hemangioma was partially thrombosed and the single feeder was preoperatively detected. These conditions in our case could be favorable to prevent from bleeding of spinal intradural extramedullary CH.
Our patient was treated successfully with removal of spinal intradural extramedullary CH and laminoplasty, as we thought that his neurological symptoms resulted from spinal intradural extramedullary CH and cervical spinal stenosis. The etiologies of syringomyelia include Chiari malformation, meningitis, intramedullary tumors, hemorrhage, and posttraumatic spinal injuries.[[37]] However, syringomyelia related to spinal stenosis has been also reported.[[37]],[[38]],[[39]],[[40]] In the previous reported cases, the syringomyelia regressed after surgery. Epidural compression by cervical stenosis has been postulated as a mechanism in the formation of syringomyelia.[[37]] Thus, spinal canal stenosis could also have been a cause in our case. Syringomyelia associated with spinal arteriovenous fistula has been described as well.[[41]] In that report, syringomyelia mostly disappeared 6 months after embolization of the spinal arteriovenous fistula. The authors did not determine the relation between the syringomyelia and spinal arteriovenous fistula to be coincidental or causative.[[41]] However, we think that venous congestion due to spinal arteriovenous fistula could have been a cause for syringomyelia in the reported case, as venous congestion-related hypervascular tumor with arteriovenous shunts has been speculated as a cause of edema and syringomyelia.[[42]] Syringomyelia in our case was not accompanied by spinal arteriovenous fistula but by spinal intradural extramedullary CH. Venous congestion due to spinal intradural extramedullary CH might have caused the syringomyelia. Preoperative spinal edema might have also resulted from epidural compression by spinal canal stenosis and venous congestion due to cervical intradural extramedullary CH. However, as ours is the first reported case of spinal intradural extramedullary CH accompanied with spinal edema and syringomyelia treated by laminoplasty and tumor resection, further similar case reports are needed to determine the detailed mechanisms.
Concerning management options of spinal intradural extramedullary CH, surgical resection seems to be standard treatment, especially in cases that the spinal cord is strongly compressed by spinal intradural extramedullary CH. As the spinal intradural extramedullary CH in our case was fed by a single feeder, preoperative embolization was not performed. However, if intraoperative bleeding risk is estimated to be high due to hypervascularity of the spinal intradural extramedullary CH, preoperative embolization can be effective.[[43]] Radiation therapy may be also an option to prevent the recurrence of spinal intradural extramedullary CH.[[43]] The patient in our case is followed for approximately 3 years without recurrence of the spinal intradural extramedullary CH. In case that the recurrence of the spinal intradural extramedullary CH is confirmed on postoperative images, solely surgical resection or combined management of surgical resection and embolization (or radiation therapy) should be considered according to the size of recurrent spinal intradural extramedullary CH.
#
Conclusion
We reported a case of spinal intradural extramedullary CH that showed preoperative spinal edema and syringomyelia as rare manifestations. The spinal edema and syringomyelia might have resulted from venous congestion of cervical intradural extramedullary CH and coexistent cervical canal stenosis. Removal of cervical intradural extramedullary CH and laminoplasty were effective in our case.
#
#
Conflict of Interest
There are no conflicts of interest.
Acknowledgment
We appreciate Drs. Ryota Ishibashi, Naoko Masuzawa, and Shinshichi Hamada, for their collaboration of this study. We would like to thank Editage (www.editage.com) for English language editing.
Financial support and sponsorship
Nil.
-
References
- 1 Kaneko Y, Yamabe K, Abe M. Rapid regrowth of a capillary hemangioma of the thoracic spinal cord. Neurol Med Chir (Tokyo) 2012;52:665-9.
- 2 Naruke Y, Horie H, Nagai Y, Ando R. Capillary hemangioma involved in filar lipoma: A case report. Clin Neuropathol 2019;38:33-7.
- 3 Holtzman RN, Brisson PM, Pearl RE, Gruber ML. Lobular capillary hemangioma of the cauda equina. Case report. J Neurosurg 1999;90:239-41.
- 4 Bouali S, Maatar N, Bouhoula A, Abderrahmen K, Kallel J, Jemel H. Intradural extramedullary capillary hemangioma in the upper cervical spine: First report. World Neurosurg 2016;92:587.e1-7.
- 5 Nowak DA, Widenka DC. Spinal intradural capillary haemangioma: A review. Eur Spine J 2001;10:464-72.
- 6 Zhu K, He D. Intradural extramedullary capillary hemangioma: A case report and review of the literature. Oncol Lett 2016;11:2896-8.
- 7 Choi BY, Chang KH, Choe G, Han MH, Park SW, Yu IK, et al. Spinal intradural extramedullary capillary hemangioma: MR imaging findings. AJNR Am J Neuroradiol 2001;22:799-802.
- 8 Alobaid A, Bennardo MR, Cenic A, Lach B. Mixed capillary-cavernous extramedullary intradural hemangioma of the spinal cord mimicking meningioma: Case report. Br J Neurosurg 2015;29:438-9.
- 9 Lee JH, Jeon I, Kim SW. Intradural extramedullary capillary hemangioma in the upper thoracic spine with simultaneous extensive arachnoiditis. Korean J Spine 2017;14:57-60.
- 10 Panero I, Eiriz C, Lagares A, Toldos O, Panero A, Paredes I. Intradural-extramedullary capillary hemangioma with acute bleeding: Case report and literature review. World Neurosurg 2017;108:988.e7-14.
- 11 Shi CZ, Shen J, Zheng CT, Zhan RY. A case of giant intradural extramedullary capillary hemangioma. Chin Med J (Engl) 2017;130:251-2.
- 12 Sharma K, Sharma UK, Sigdel B. Cervical capillary haemangioma: A case report. Kathmandu Univ Med J (KUMJ) 2014;12:211-4.
- 13 Shin JH, Lee HK, Jeon SR, Park SH. Spinal intradural capillary hemangioma: MR findings. Am J Neuroradiol 2000;21:954-6.
- 14 Cetinkal A, Colak A, Topuz K, Atabey C, Berber U. Capillary hemangioma of the cervical intervertebral disc. Eur Spine J 2011;20 Suppl 2:S157-60.
- 15 Abdullah DC, Raghuram K, Phillips CD, Jane JA Jr., Miller B. Thoracic intradural extramedullary capillary hemangioma. Am J Neuroradiol 2004;25:1294-6.
- 16 Alakandy LM, Hercules S, Balamurali G, Reid H, Herwadkar A, Holland JP. Thoracic intradural extramedullary capillary haemangioma. Br J Neurosurg 2006;20:235-8.
- 17 Andaluz N, Balko MG, Stanek J, Morgan C, Schwetschenau PR. Lobular capillary hemangioma of the spinal cord: Case report and review of the literature. J Neurooncol 2002;56:261-4.
- 18 Cheng Y, Lu K, Jiang H. Epidural angiolipoma with concomitant intradural extramedullary capillary hemangioma at the same spinal level: A case report. Oncol Lett 2020;20:209-14.
- 19 Chung SK, Nam TK, Park SW, Hwang SN. Capillary hemangioma of the thoracic spinal cord. J Korean Neurosurg Soc 2010;48:272-5.
- 20 Crispino M, Vecchioni S, Galli G, Olivetti L. Spinal intradural extramedullary haemangioma: MRI and neurosurgical findings. Acta Neurochir (Wien) 2005;147:1195-8.
- 21 Funayama T, Sakane M, Murai S, Ochiai N. Multiple capillary hemangiomas of the cauda equina at a level of a single vertebra. J Orthop Sci 2010;15:598-602.
- 22 Ganapathy S, Kleiner LI, Mirkin LD, Hall L. Intradural capillary hemangioma of the cauda equina. Pediatr Radiol 2008;38:1235-8.
- 23 Ghazi NG, Jane JA, Lopes MB, Newman SA. Capillary hemangioma of the cauda equina presenting with radiculopathy and papilledema. J Neuroophthalmol 2006;26:98-102.
- 24 Hanakita J, Suwa H, Nagayasu S, Suzuki H. Capillary hemangioma in the cauda equina: Neuroradiological findings. Neuroradiology 1991;33:458-61.
- 25 Kim KJ, Lee JY, Lee SH. Spinal intradural capillary hemangioma. Surg Neurol 2006;66:212-4.
- 26 Liu JJ, Lee DJ, Jin LW, Kim KD. Intradural extramedullary capillary hemangioma of the cauda equina: Case report and literature review. Surg Neurol Int 2015;6:S127-31.
- 27 Mastronardi L, Guiducci A, Frondizi D, Carletti S, Spera C, Maira G. Intraneural capillary hemangioma of the cauda equina. Eur Spine J 1997;6:278-80.
- 28 Miri SM, Habibi Z, Hashemi M, Meybodi AT, Tabatabai SA. Capillary hemangioma of cauda equina: A case report. Cases J 2009;2:80.
- 29 Nowak DA, Gumprecht H, Stolzle A, Lumenta CB. Intraneural growth of a capillary haemangioma of the cauda equina. Acta Neurochir (Wien) 2000;142:463-7.
- 30 Pignotti F, Coli A, Fernandez E, Montano N. Capillary hemangioma of the cauda equina. Surg Neurol Int 2015;6:133.
- 31 Roncaroli F, Scheithauer BW, Krauss WE. Capillary hemangioma of the spinal cord. Report of four cases. J Neurosurg 2000;93:148-51.
- 32 Sonawane DV, Jagtap SA, Mathesul AA. Intradural extramedullary capillary hemangioma of lower thoracic spinal cord. Indian J Orthop 2012;46:475-8.
- 33 Takata Y, Sakai T, Higashino K, Goda Y, Tezuka F, Sairyo K. Intradural extramedullary capillary hemangioma in the upper thoracic spine: A review of the literature. Case Rep Orthop 2014;2014:604131.
- 34 Tunthanathip T, Rattanalert S, Oearsakul T, Kanjanapradit K. Spinal capillary hemangiomas: Two cases reports and review of the literature. Asian J Neurosurg 2017;12:556-62.
- 35 Unnithan AK, Joseph TP, Gautam A, Shymole V. Case report of lumbar intradural capillary hemangioma. Surg Neurol Int 2016;7:S139-41.
- 36 Zander DR, Lander P, Just N, Albrecht S, Mohr G. Magnetic resonance imaging features of a nerve root capillary hemangioma of the spinal cord: Case report. Can Assoc Radiol J 1998;49:398-400.
- 37 Badri M, Gader G, Bahri K, Zammel I. Cervicothoracic syringomyelia caused by cervical spinal stenosis: Case report and literature review. Surg Neurol Int 2017;8:288.
- 38 Bhagavathula Venkata SS, Arimappamagan A, Lafazanos S, Pruthi N. Syringomyelia secondary to cervical spondylosis: Case report and review of literature. J Neurosci Rural Pract 2014;5:S78-82.
- 39 Kimura R, Park YS, Nakase H, Sakaki T. Syringomyelia caused by cervical spondylosis. Acta Neurochir (Wien) 2004;146:175-8.
- 40 Rebai R, Boudawara MZ, Ben Yahia M, Mhiri C, Ben Mansour H. Syringomyelobulbia associated with cervical spondylosis. Pathophysiology and therapeutic implications. Neurochirurgie 2002;48:120-3.
- 41 Finsterer J, Bavinzski G, Ungersböck K. Spinal dural arteriovenous fistula associated with syringomyelia. J Neuroradiol 2000;27:211-4.
- 42 Chu BC, Terae S, Hida K, Furukawa M, Abe S, Miyasaka K. MR findings in spinal hemangioblastoma: Correlation with symptoms and with angiographic and surgical findings. AJNR Am J Neuroradiol 2001;22:206-17.
- 43 Rai RR, Shah S, Deogaonkar K, Dalvie S. Aggressive vertebral hemangioma causing spinal cord compression: Presenting a study of two cases and review of literature. J Orthop Case Rep 2018;8:33-7.
Address for correspondence
Publication History
Received: 02 February 2021
Accepted: 23 May 2021
Article published online:
16 August 2022
© 2021. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Kaneko Y, Yamabe K, Abe M. Rapid regrowth of a capillary hemangioma of the thoracic spinal cord. Neurol Med Chir (Tokyo) 2012;52:665-9.
- 2 Naruke Y, Horie H, Nagai Y, Ando R. Capillary hemangioma involved in filar lipoma: A case report. Clin Neuropathol 2019;38:33-7.
- 3 Holtzman RN, Brisson PM, Pearl RE, Gruber ML. Lobular capillary hemangioma of the cauda equina. Case report. J Neurosurg 1999;90:239-41.
- 4 Bouali S, Maatar N, Bouhoula A, Abderrahmen K, Kallel J, Jemel H. Intradural extramedullary capillary hemangioma in the upper cervical spine: First report. World Neurosurg 2016;92:587.e1-7.
- 5 Nowak DA, Widenka DC. Spinal intradural capillary haemangioma: A review. Eur Spine J 2001;10:464-72.
- 6 Zhu K, He D. Intradural extramedullary capillary hemangioma: A case report and review of the literature. Oncol Lett 2016;11:2896-8.
- 7 Choi BY, Chang KH, Choe G, Han MH, Park SW, Yu IK, et al. Spinal intradural extramedullary capillary hemangioma: MR imaging findings. AJNR Am J Neuroradiol 2001;22:799-802.
- 8 Alobaid A, Bennardo MR, Cenic A, Lach B. Mixed capillary-cavernous extramedullary intradural hemangioma of the spinal cord mimicking meningioma: Case report. Br J Neurosurg 2015;29:438-9.
- 9 Lee JH, Jeon I, Kim SW. Intradural extramedullary capillary hemangioma in the upper thoracic spine with simultaneous extensive arachnoiditis. Korean J Spine 2017;14:57-60.
- 10 Panero I, Eiriz C, Lagares A, Toldos O, Panero A, Paredes I. Intradural-extramedullary capillary hemangioma with acute bleeding: Case report and literature review. World Neurosurg 2017;108:988.e7-14.
- 11 Shi CZ, Shen J, Zheng CT, Zhan RY. A case of giant intradural extramedullary capillary hemangioma. Chin Med J (Engl) 2017;130:251-2.
- 12 Sharma K, Sharma UK, Sigdel B. Cervical capillary haemangioma: A case report. Kathmandu Univ Med J (KUMJ) 2014;12:211-4.
- 13 Shin JH, Lee HK, Jeon SR, Park SH. Spinal intradural capillary hemangioma: MR findings. Am J Neuroradiol 2000;21:954-6.
- 14 Cetinkal A, Colak A, Topuz K, Atabey C, Berber U. Capillary hemangioma of the cervical intervertebral disc. Eur Spine J 2011;20 Suppl 2:S157-60.
- 15 Abdullah DC, Raghuram K, Phillips CD, Jane JA Jr., Miller B. Thoracic intradural extramedullary capillary hemangioma. Am J Neuroradiol 2004;25:1294-6.
- 16 Alakandy LM, Hercules S, Balamurali G, Reid H, Herwadkar A, Holland JP. Thoracic intradural extramedullary capillary haemangioma. Br J Neurosurg 2006;20:235-8.
- 17 Andaluz N, Balko MG, Stanek J, Morgan C, Schwetschenau PR. Lobular capillary hemangioma of the spinal cord: Case report and review of the literature. J Neurooncol 2002;56:261-4.
- 18 Cheng Y, Lu K, Jiang H. Epidural angiolipoma with concomitant intradural extramedullary capillary hemangioma at the same spinal level: A case report. Oncol Lett 2020;20:209-14.
- 19 Chung SK, Nam TK, Park SW, Hwang SN. Capillary hemangioma of the thoracic spinal cord. J Korean Neurosurg Soc 2010;48:272-5.
- 20 Crispino M, Vecchioni S, Galli G, Olivetti L. Spinal intradural extramedullary haemangioma: MRI and neurosurgical findings. Acta Neurochir (Wien) 2005;147:1195-8.
- 21 Funayama T, Sakane M, Murai S, Ochiai N. Multiple capillary hemangiomas of the cauda equina at a level of a single vertebra. J Orthop Sci 2010;15:598-602.
- 22 Ganapathy S, Kleiner LI, Mirkin LD, Hall L. Intradural capillary hemangioma of the cauda equina. Pediatr Radiol 2008;38:1235-8.
- 23 Ghazi NG, Jane JA, Lopes MB, Newman SA. Capillary hemangioma of the cauda equina presenting with radiculopathy and papilledema. J Neuroophthalmol 2006;26:98-102.
- 24 Hanakita J, Suwa H, Nagayasu S, Suzuki H. Capillary hemangioma in the cauda equina: Neuroradiological findings. Neuroradiology 1991;33:458-61.
- 25 Kim KJ, Lee JY, Lee SH. Spinal intradural capillary hemangioma. Surg Neurol 2006;66:212-4.
- 26 Liu JJ, Lee DJ, Jin LW, Kim KD. Intradural extramedullary capillary hemangioma of the cauda equina: Case report and literature review. Surg Neurol Int 2015;6:S127-31.
- 27 Mastronardi L, Guiducci A, Frondizi D, Carletti S, Spera C, Maira G. Intraneural capillary hemangioma of the cauda equina. Eur Spine J 1997;6:278-80.
- 28 Miri SM, Habibi Z, Hashemi M, Meybodi AT, Tabatabai SA. Capillary hemangioma of cauda equina: A case report. Cases J 2009;2:80.
- 29 Nowak DA, Gumprecht H, Stolzle A, Lumenta CB. Intraneural growth of a capillary haemangioma of the cauda equina. Acta Neurochir (Wien) 2000;142:463-7.
- 30 Pignotti F, Coli A, Fernandez E, Montano N. Capillary hemangioma of the cauda equina. Surg Neurol Int 2015;6:133.
- 31 Roncaroli F, Scheithauer BW, Krauss WE. Capillary hemangioma of the spinal cord. Report of four cases. J Neurosurg 2000;93:148-51.
- 32 Sonawane DV, Jagtap SA, Mathesul AA. Intradural extramedullary capillary hemangioma of lower thoracic spinal cord. Indian J Orthop 2012;46:475-8.
- 33 Takata Y, Sakai T, Higashino K, Goda Y, Tezuka F, Sairyo K. Intradural extramedullary capillary hemangioma in the upper thoracic spine: A review of the literature. Case Rep Orthop 2014;2014:604131.
- 34 Tunthanathip T, Rattanalert S, Oearsakul T, Kanjanapradit K. Spinal capillary hemangiomas: Two cases reports and review of the literature. Asian J Neurosurg 2017;12:556-62.
- 35 Unnithan AK, Joseph TP, Gautam A, Shymole V. Case report of lumbar intradural capillary hemangioma. Surg Neurol Int 2016;7:S139-41.
- 36 Zander DR, Lander P, Just N, Albrecht S, Mohr G. Magnetic resonance imaging features of a nerve root capillary hemangioma of the spinal cord: Case report. Can Assoc Radiol J 1998;49:398-400.
- 37 Badri M, Gader G, Bahri K, Zammel I. Cervicothoracic syringomyelia caused by cervical spinal stenosis: Case report and literature review. Surg Neurol Int 2017;8:288.
- 38 Bhagavathula Venkata SS, Arimappamagan A, Lafazanos S, Pruthi N. Syringomyelia secondary to cervical spondylosis: Case report and review of literature. J Neurosci Rural Pract 2014;5:S78-82.
- 39 Kimura R, Park YS, Nakase H, Sakaki T. Syringomyelia caused by cervical spondylosis. Acta Neurochir (Wien) 2004;146:175-8.
- 40 Rebai R, Boudawara MZ, Ben Yahia M, Mhiri C, Ben Mansour H. Syringomyelobulbia associated with cervical spondylosis. Pathophysiology and therapeutic implications. Neurochirurgie 2002;48:120-3.
- 41 Finsterer J, Bavinzski G, Ungersböck K. Spinal dural arteriovenous fistula associated with syringomyelia. J Neuroradiol 2000;27:211-4.
- 42 Chu BC, Terae S, Hida K, Furukawa M, Abe S, Miyasaka K. MR findings in spinal hemangioblastoma: Correlation with symptoms and with angiographic and surgical findings. AJNR Am J Neuroradiol 2001;22:206-17.
- 43 Rai RR, Shah S, Deogaonkar K, Dalvie S. Aggressive vertebral hemangioma causing spinal cord compression: Presenting a study of two cases and review of literature. J Orthop Case Rep 2018;8:33-7.