
Subscribe to RSS
DOI: 10.4103/ajns.AJNS_371_19
Spinal ewing's Sarcoma presenting as an epidural collection: A rare presentation of a rare entity

Rare entities are difficult to predict. They are considered last rightly, to expedite treatment and alleviate symptoms quickly. Rare presentations of rare diseases form a particularly difficult section of diagnoses that are not only impossible to predict but difficult to recognize, diagnose, and treat. Often the dilemma is to, investigate thoroughly saving time but financially burdening the patient and hospital, or, to investigate in gradual increments taking more time and effort, especially in rare cases where prolonged hospitalization and suffering occurs before the diagnosis is reached. This approach, however, wastes critically important time, which, especially in neurological compression, may often lead to irreversible deficits. This dilemma is admirably demonstrated in this case report of spinal Ewing's sarcoma. A young female presented to us with recurrent high cervical epidural collections presenting as compressive myelopathy. She underwent repeated decompressions, and the collection was misdiagnosed as tuberculosis, which was treated without empirical evidence, leading to significant irreversible disability. Finally, when she came to us, the histopathological assessment was done to reveal the diagnosis. Ewing's sarcomas, and indeed the whole gamut of small-round-cell malignancies, are great imitators. They are known to exist in the skull base mimicking schwannomas, chordomas, germinomas, pituitary adenomas, and even epidermoids and occasionally extend to the vertebral bodies and the cranio-vertebral Junction (CVJ) leading to instability and neurological compression. Here, they mimic vertebral tumors, discitis, infective abscesses, and even myeloma. Predictably, such an entity is diagnosed last, and diagnosed late, leading to bad consequences for the patient. Such was the fate of our patient. The report emphasizes the diagnostic dilemma and presents the need to use protocols for diagnosis and treatment, even in rare cases, to effect the best possible outcomes for patients. The use of a thorough diagnostic and management algorhythm prevents deeper and sinister disease processes from being missed.
#
Introduction
Ewing sarcoma (ES) and peripheral primitive neuroectodermal tumor (pPNET) comprise the same spectrum of neoplastic diseases known as the ES family of tumors, which also includes malignant small-cell tumor of the chest wall (Askin tumor) and atypical ES. Primary spinal ES/pPNETs are regarded as undifferentiated malignant small-round-cell tumors, which mostly occur in long bones, flat bones, ribs, and soft tissue. ES/pPNETs account for 6%–8% of primary malignant bone tumors and rarely affect intraspinal/vertebral deep mesenchymal/meningeal tissue.[[1]],[[2]],[[3]] Due to a lack of clinic symptoms and specific biomarkers at the early stages of primary spinal ES/pPNETs, most patients are not diagnosed until advanced stages, which concomitantly worsens outcomes. Furthermore, because the tumor has an aggressive clinical course, with a high tendency for both local recurrence and distant metastasis, a timely and accurate preoperative diagnosis of primary spinal ES/pPNETs could provide useful information for surgical planning.[[3]],[[4]] Therefore, comprehensive studies on the clinical characteristics of primary spinal ES/pPNETs are warranted.
The rarity of the disease makes its purported surgical management and prognostic factors controversial. In addition, most related information about this disease comes from individual case reports or small case series reports, which lack robust statistical outcomes.[[5]],[[6]],[[7]],[[8]],[[9]] To illustrate the surgical management and prognostic factors of primary spinal ES/pPNETs, we present our case report, to highlight the diagnostic dilemma and dire consequences of delay in diagnosis and treatment of these rarest of rare diseases.[[7]],[[8]],[[9]]
#
Case Report
A 33-year-old female presented with features suggestive of high cervical compressive myelopathy and radicular pain at C3. On examination, she had upgoing plantars, spasticity in the lower limbs, and C4 and C5 sensory dermatomal loss. Investigation at her hometown showed vertebral collapse with instability along with compression of the cervical spine [[Figure 1]]. There were signal changes noted in the cord but with heterogeneous enhancement in the C3 vertebra with a collection/pus seen occupying the anterior one-third of the spinal canal compressing the cord from the clivus to C4.

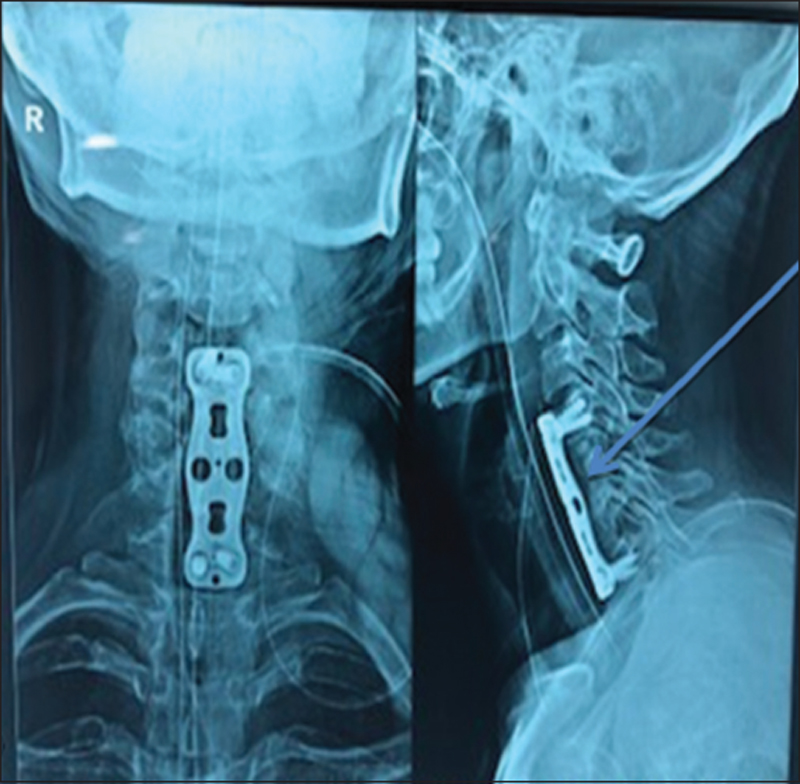
She was subjected to a corpectomy collection drainage and anterior canal decompression, with fusion using a cage and anterior cervical plate construct [[Figure 2]]. After surgery, her neurological status improved dramatically and she was discharged early from the hospital. The vertebral fragments along with the collection were sampled and sent for analysis. They showed no signs of infection (especially tuberculosis [TB]). Histopathology showed a Monolymphatic infiltrate in the collection sample but no malignant cells or evidence of chronic inflammation or stigmata of TB.
Owing to the lack of evidence regarding TB, the patient was referred to an oncologist for further treatment. It was considered possible that the mononuclear infiltrate could indicate a lymphomatous process and thus would require chemotherapy. Unfortunately, the patient was lost to follow-up and did not receive any chemotherapy. No immunohistochemical and advanced typing of the HPE sample to arrive at a definitive diagnosis was done either.
Two years later, she presented to a tertiary referral center with the same symptoms. This time, however, she had spastic quadriparesis with bowel and bladder dysfunction. Her images showed a recollection over the anterior aspect of the spinal canal compressing the cord [[Figure 3]]. A repeat decompression was done, and samples were sent for analysis. The patient again was lost to follow-up and went to a different center for consultation. Due to the inconclusive nature of the histopathology reports, and the recurrence of the compression, she was started empirically on antituberculous management. The high incidence of spinal and bone TB in the country as well as the near-classic clinical and radiological presentation prompted the initiation of therapy. She faithfully took her tablet for 2 years, during which she had no improvement of symptoms.

After 2 years, she noticed a gradual deterioration that worsened rapidly into quadriplegia and complete sensory loss below the neck. Imaging done on an emergency basis showed a posterior spinal compression with significant cord compression, with cord changes [[Figure 4]]. An emergency posterior laminectomy was done from C3 to C7 decompressing and removing the compressive inflamed organized semisolid mass. Unfortunately, postoperatively, she had no improvement in her quadriplegia or her bladder and bowel control. She was shifted to a neuro rehab center for further care, where she gradually has started to improve.

Her histopathology this time showed a small-blue-round-cell tumor with occasional ill-formed rosettes. Further immunohistochemical (IHC) panels revealed diffuse positivity for FLI-1 and focal patchy membranous positivity for CD99, and a final diagnosis of Ewing's sarcoma/PNET was given [[Figure 5]]a and [[Figure 5]]b. She was immediately called back for oncology consultations and to start immediate chemotherapy. This is ongoing and full remission is hoped for, as she gradually improves with neuro rehab.

#
Discussion
The case reported by Ke et al.[[2]] was a primary treatment case. The patient underwent first-stage laminectomy, postoperative radiotherapy and chemotherapy, and second-stage vertebral resection. In our case, the thoracic vertebral compression fracture was the primary manifestation. Due to the delay in medical treatment, the tumor continued to expand and involved the affected spine segment, which limited treatment options and increased the difficulty of second-stage surgery in our hospital. Due to local postoperative changes of soft tissue, the separation of tumor tissue requires great care. However, even if the operation is very difficult, and the patient had preoperative symptoms of paralysis of both lower limbs for 1 month, we still believe that surgical treatment is very necessary. The results of postoperative follow-up showed that patients benefited from this positive surgical choice.
Chen et al.[[3]],[[4]],[[5]],[[6]] believe that local injection of bone cement can kill tumor cells in the vertebral body through local high temperature, cytotoxicity, and blood supply destruction, but in the current case, vertebral injection of bone cement in the first stage failed to effectively inhibit the growth of primary Ewing's sarcoma. In contrast, increased local pressure in the vertebral body led to passive expansion of the primary tumor and bone cement leakage at the posterior margin of the vertebral body. Such a result reminds us of the importance of choosing bone cement injection during vertebroplasty. For patients with vertebral tumors, special attention should be taken during vertebroplasty for bone cement leakage caused by excessive bone cement injection and increased local pressure.[[8]],[[9]],[[10]]
This case further reminds us of the importance of the differential diagnosis of Ewing's sarcoma and compression fractures. For compression fractures of the spine, we must consider the cause with thorough local soft-tissue examination before the surgery and pay attention to eliminate the possibility of a tumor.[[11]] In this case, the tumor marker serum ferritin level was elevated, which is suggestive of Ewing's sarcoma.[[12]] The patient had an abnormal liver function, with no abnormal liver areas on total abdominal computed tomography or hepatitis virus infection, as suggested by hepatitis screening. Statistical analysis of more cases is needed to explore the relationship between liver function abnormalities and the occurrence of Ewing's sarcoma.[[11]],[[13]],[[14]] Histologically, the PNET cells exhibit a primitive, poorly differentiated morphology with varying degrees of pleomorphism and occasional evidence of neuroectodermal differentiation. The final diagnosis requires IHC analysis and cytogenetic studies to identify (11;22)(q24;q12) translocation. EWS/ETS fusions as the presumed initiating oncogenic event are required for proliferation and tumorigenesis.[[13]],[[14]]
#
#
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Sato S, Mitsuyama T, Ishii A, Kawakami M, Kawamata T. Multiple primary cranial Ewing's sarcoma in adulthood: Case report. Neurosurg 2009;64:E384-6.
- 2 Ke C, Duan Q, Yang H, Zhu F, Yan M, Xu SP, et al. Meningeal Ewing sarcoma/peripheral PNET: Clinicopathological, immunohistochemical and FISH study of four cases. Neuropathol 2017;37:35-44.
- 3 Chen J, Jiang Q, Zhang Y, Yu Y, Zheng Y, Chen J, et al. Clinical features and long-term outcome of primary intracranial Ewing sarcoma/peripheral primitive neuroectodermal tumors: 14 cases from a single institution. World Neurosurg 2018;122:e1606-14.
- 4 Tong X, Deng X, Yang T, Yang C, Wu L, Wu J, et al. Clinical presentation and long-term outcome of primary spinal peripheral primitive neuroectodermal tumors. J Neurooncol 2015;124:455-63.
- 5 Ellis JA, Rothrock RJ, Moise G, McCormick PC, Tanji K, Canoll P, et al. Primitive neuroectodermal tumors of the spine: A comprehensive review with illustrative clinical cases. Neurosurg Focus 2011;30:E1.
- 6 Kampman WA, Kros JM, De Jong TH, Lequin MH. Primitive neuroectodermal tumours (PNETs) located in the spinal canal; the relevance of classification as central or peripheral PNET: Case report of a primary spinal PNET occurrence with a critical literature review. J Neurooncol 2006;77:65-72.
- 7 Saeedinia S, Nouri M, Alimohammadi M, Moradi H, Amirjamshidi A. Primary spinal extradural Ewing's sarcoma (primitive neuroectodermal tumor): Report of a case and meta-analysis of the reported cases in the literature. Surg Neurol Int 2012;3:55.
- 8 Qi W, Deng X, Liu T, Hou Y, Yang C, Wu L, et al. Comparison of primary spinal central and peripheral primitive neuroectodermal tumors in clinical and imaging characteristics and long-term outcome. World Neurosurg 2016;88:359-69.
- 9 Tsutsumi S, Yasumoto Y, Manabe A, Ogino I, Arai H, Ito M. Magnetic resonance imaging appearance of primary spinal extradural Ewing's sarcoma: Case report and literature review. Clin Neuroradiol 2013;23:81-5.
- 10 Muller K, Diez B, Muggeri A, Pietsch T, Friedrich C, Rutkowski S, et al. What's in a name? Intracranial peripheral primitive neuroectodermal tumors and CNS primitive neuroectodermal tumors are not the same. Strahlenther Onkol 2013;189:372-9.
- 11 Delattre O, Zucman J, Melot T, Garau XS, Zucker JM, Lenoir GM, et al. The Ewing family of tumors – A subgroup of small-round-cell tumors defined by specific chimeric transcripts. N Engl J Med 1994;331:294-9.
- 12 Folpe AL, Goldblum JR, Rubin BP, Shehata BM, Liu W, Dei Tos AP, et al. Morphologic and immunophenotypic diversity in Ewing family tumors: A study of 66 genetically confirmed cases. Am J Surg Pathol 2005;29:1025-33.
- 13 Hrabálek L, Kalita O, Svebisova H, Ehrmann J Jr., Hajduch M, Trojanec R, et al. Dumbbell-shaped peripheral primitive neuroectodermal tumor of the spine – Case report and review of the literature. J Neurooncol 2009;92:211-7.
- 14 Vural C, Uluoglu O, Akyurek N, Oguz A, Karadeniz C. The evaluation of CD99 immunoreactivity and EWS/FLI1 translocation by fluorescence in situ hybridization in central PNETs and Ewing's sarcoma family of tumors. Pathol Oncol Res 2011;17:619-25.
Address for correspondence
Publication History
Received: 28 December 2019
Accepted: 02 April 2020
Article published online:
16 August 2022
© 2020. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sato S, Mitsuyama T, Ishii A, Kawakami M, Kawamata T. Multiple primary cranial Ewing's sarcoma in adulthood: Case report. Neurosurg 2009;64:E384-6.
- 2 Ke C, Duan Q, Yang H, Zhu F, Yan M, Xu SP, et al. Meningeal Ewing sarcoma/peripheral PNET: Clinicopathological, immunohistochemical and FISH study of four cases. Neuropathol 2017;37:35-44.
- 3 Chen J, Jiang Q, Zhang Y, Yu Y, Zheng Y, Chen J, et al. Clinical features and long-term outcome of primary intracranial Ewing sarcoma/peripheral primitive neuroectodermal tumors: 14 cases from a single institution. World Neurosurg 2018;122:e1606-14.
- 4 Tong X, Deng X, Yang T, Yang C, Wu L, Wu J, et al. Clinical presentation and long-term outcome of primary spinal peripheral primitive neuroectodermal tumors. J Neurooncol 2015;124:455-63.
- 5 Ellis JA, Rothrock RJ, Moise G, McCormick PC, Tanji K, Canoll P, et al. Primitive neuroectodermal tumors of the spine: A comprehensive review with illustrative clinical cases. Neurosurg Focus 2011;30:E1.
- 6 Kampman WA, Kros JM, De Jong TH, Lequin MH. Primitive neuroectodermal tumours (PNETs) located in the spinal canal; the relevance of classification as central or peripheral PNET: Case report of a primary spinal PNET occurrence with a critical literature review. J Neurooncol 2006;77:65-72.
- 7 Saeedinia S, Nouri M, Alimohammadi M, Moradi H, Amirjamshidi A. Primary spinal extradural Ewing's sarcoma (primitive neuroectodermal tumor): Report of a case and meta-analysis of the reported cases in the literature. Surg Neurol Int 2012;3:55.
- 8 Qi W, Deng X, Liu T, Hou Y, Yang C, Wu L, et al. Comparison of primary spinal central and peripheral primitive neuroectodermal tumors in clinical and imaging characteristics and long-term outcome. World Neurosurg 2016;88:359-69.
- 9 Tsutsumi S, Yasumoto Y, Manabe A, Ogino I, Arai H, Ito M. Magnetic resonance imaging appearance of primary spinal extradural Ewing's sarcoma: Case report and literature review. Clin Neuroradiol 2013;23:81-5.
- 10 Muller K, Diez B, Muggeri A, Pietsch T, Friedrich C, Rutkowski S, et al. What's in a name? Intracranial peripheral primitive neuroectodermal tumors and CNS primitive neuroectodermal tumors are not the same. Strahlenther Onkol 2013;189:372-9.
- 11 Delattre O, Zucman J, Melot T, Garau XS, Zucker JM, Lenoir GM, et al. The Ewing family of tumors – A subgroup of small-round-cell tumors defined by specific chimeric transcripts. N Engl J Med 1994;331:294-9.
- 12 Folpe AL, Goldblum JR, Rubin BP, Shehata BM, Liu W, Dei Tos AP, et al. Morphologic and immunophenotypic diversity in Ewing family tumors: A study of 66 genetically confirmed cases. Am J Surg Pathol 2005;29:1025-33.
- 13 Hrabálek L, Kalita O, Svebisova H, Ehrmann J Jr., Hajduch M, Trojanec R, et al. Dumbbell-shaped peripheral primitive neuroectodermal tumor of the spine – Case report and review of the literature. J Neurooncol 2009;92:211-7.
- 14 Vural C, Uluoglu O, Akyurek N, Oguz A, Karadeniz C. The evaluation of CD99 immunoreactivity and EWS/FLI1 translocation by fluorescence in situ hybridization in central PNETs and Ewing's sarcoma family of tumors. Pathol Oncol Res 2011;17:619-25.