

Subscribe to RSS
DOI: 10.4103/ajns.AJNS_158_18
Timing of surgery and surgical strategies in symptomatic brainstem cavernomas: Review of the literature
Authors

Brainstem cavernomas (BSCs) are angiographically occult, benign low flow vascular malformations that pose a significant surgical challenge due to their eloquent location. The present study includes an extensive review of the literature and three illustrative cases of BSC with emphasis on the timing of surgery: surgical approaches, usage of intraoperative monitoring, and complication avoidance. A systematic search was performed using the PubMed database was from January 1, 1999, to June 2018. The relevant articles were reviewed with particular attention to hemorrhage rates, timing of surgery, indications for surgery, surgical approaches, and outcome. Along with this, a retrospective analysis of three cases of symptomatic BSC, who were operated for the same, during the year 2018 in our institute was conducted. All the three patients presented with at least 1 episode of hemorrhage before surgery. Of these, one patient was operated immediately due to altered sensorium whereas the other two were operated after at least 4 weeks of the hemorrhagic episode. The patients who were operated in the subacute phase of bleed were seen to have liquefaction of hematoma, thus providing a good surgical demarcation and thereby reduced surgery-related trauma to the surrounding eloquent structures. Two patients improved neurologically during the immediate postoperative period, whereas one had transient worsening of neurological deficits during the immediate postoperative period in the form of additional cranial nerve palsies which completely improved on follow-up after 2 months. Radical resection is recommended in all patients with symptomatic BSCs. Surgery should be considered after the first or the second episode of hemorrhage as multiple rebleeds can cause exacerbation of deficits and sometimes mortality as well. Considering surgical timing, anywhere between 4 and 6 weeks or the subacute phase of the hemorrhage is considered appropriate. The aims of surgical intervention must be to improve preoperative function, minimize surgical morbidity and to reduce hemorrhagic rates. In spite of the significant surgical morbidity associated with BSCs, appropriate patient selection, meticulous surgical planning with adjuncts such as intraoperative monitoring and neuronavigation will go a long way in avoidance of major postoperative complications.
Introduction
Cavernous malformations (CMs) or cavernomas are rare, angiographically occult lesions occurring in the central nervous system with an incidence of approximately 0.5% (0.4%–0.6%) in the general population.[[1]],[[2]] They are the second-most common type of cerebrovascular lesions, constituting about 10%–15% of all intracranial vascular malformations.[[3]],[[4]] The common location of intracranial CMs is the supratentorial regions, basal ganglia, brain stem, cerebellopontine angle, and cerebellar hemispheres.[[3]] Among these, the prevalence within the brainstem varies from 4% to 35%.[[1]],[[5]],[[6]],[[7]] Histopathologically, cavernomas are characterized by dilated, thin-walled sinusoidal vascular channels lined by a simple endothelium and thin fibrous adventitia, lacking in muscular and elastic layers, which predisposes to bleeding. These channels are filled with blood at various stages of thrombosis and organization. These lesions are usually surrounded by hemosiderin and gliosis, but typically no brain parenchyma is found within the lesion.[[1]],[[3]],[[4]],[[8]],[[9]]
Brainstem cavernomas (BSCs) garner significant interest from neurosurgeons due to their eloquent and precarious location, which when cause hemorrhages, can have devastating morbidity and sometimes mortality. Thus, promoting relentless efforts to improve microsurgical techniques and operative adjuncts such as intraoperative monitoring and neuronavigation to improve the postoperative outcome.[[5]],[[10]] However, the selection of surgical approach, indications and the timing of intervention yet remains unclear owing to the limitations found in the knowledge about the natural history of the disease.[[1]],[[4]],[[10]] In this article, we describe three cases of BSCs treated surgically at our institute along with an extensive review of natural history, clinical characteristics, radiology, timing of surgery, planning of a therapeutic approach, and intraoperative adjuncts used in the treatment of BSCs.
Materials and Methods
The charts of the three patients who were admitted with a diagnosis of BSC were retrospectively reviewed. All of them had a preoperative magnetic resonance imaging (MRI) brain with T1; T2; susceptibility weighted imaging (SWI); diffusion-weighted imaging; and apparent diffusion coefficient sequences done. The episode of hemorrhage was defined as an acute, new-onset, or worsening neurological deficit corresponding to the location of hemorrhage on computed tomography and MRI imaging.[[11]],[[12]] There was a through preoperative planning in terms of the surgical approach to be used. One patient had to be taken up for emergency surgery, whereas the other two were operated after about 1 month of bleed. Intraoperative monitoring in the form of motor evoked potential (MEP), brainstem auditory evoked response (BAER), and somatosensory evoked potential (SSEP) were recorded for all the cases.
A systematic search was performed using the PubMed database with all possible combinations of CM keywords and MESH terms such as “brainstem cavernoma,” “natural history,” “timing of surgery,” “surgical approaches,” “safe entry zones,” and “surgical outcome” was performed from January 1, 1999, to June 2018. We incorporated the English language studies that provided relevant information about the keywords and an extensive review of the literature was done. Among the articles providing similar information, the latest one was considered.
Case Presentation
Case 1
A 47-year-old male was a known case of left putaminal CM. He underwent craniotomy and excision of the lesion following an episode of hemorrhage and hemiparesis in 1996. The residual right hemiparesis improved with time. He was on regular follow-up with serial MRI which showed no residue/recurrence/any other lesions. The follow-up MRI done in January 2018 showed a small lesion in the pons which was planned for conservative management as the patient was asymptomatic. He presented to the emergency department 4 months later with sudden-onset altered sensorium. On neurological examination, he was E3, V4, and M6 with ataxia.
The MRI brain revealed a large intra-axial pontine lesion, extending more to the left with a characteristic “popcorn” appearance with a rim of signal loss due to hemosiderin, with areas of fresh bleed and surrounding edema causing brainstem compression. The SWI sequences demonstrated prominent blooming and the T2 signal was varied internally due to multiple hemorrhages within the lesion. The T1 images were isointense to hyperintense [[Figure 1]].

Microsurgical removal of the lesion was performed by a combined left retrosigmoid and posterior transpetrosal approach with the patient in lateral position. Intraoperative SSEP, MEP, and BAER were recorded. There was no discoloration noted on the pontine surface. The lesion was approached through the lateral pontine zone/the peritrigeminal area.[[10]],[[13]] Postcorticectomy, the hematoma was evacuated. The lesion was reddish brown in color, well-marginated, firm, found adherent to the surrounding brain stem. Piecemeal complete excision of the lesion was done. There were no changes in the evoked potentials intraoperatively.
Histopathological examination revealed the lesion to be a CM.
Postoperative period was uneventful. Patient's sensorium was normal with significant improvement in ataxia. He had mild left trigeminal hypoesthesia postoperatively. Postoperative MRI showed no residual lesion [[Figure 1]]. At 2-month follow-up, the patient was symptom-free.
Case 2
A 67-year-old male, who was a known case of right trigeminal neuralgia for 6 months, presented with a history of right facial, persistent dysesthesia for 2 months which did not subside with medications. On neurological examination, he had a right hemifacial hypoesthesia involving the ophthalmic, maxillary, and mandibular divisions of the trigeminal nerve. He had no other neurological deficits.
The MRI brain showed a right side intra-axial lesion, at the level of the root entry zone of trigeminal nerve. The SWI sequences showed blooming. The lesion was hyper- to iso-intense on T1WI and hyper to hypointense on T2 weighted image (T2WI).
Microsurgical removal of the lesion was performed by the right retrosigmoid approach, with the patient in lateral position. Intraoperative SSEP, MEP, and BAER were recorded. The lesion was approached through the safe entry zone in the lateral pontine or the peritrigeminal area,[[13]] similar to the previous case. There was mild xanthochromic discoloration noted on the pontine surface. Dark reddish brown fluid was found after corticectomy. The lesion was reddish brown with a relatively good margin in most areas and was excised piecemeal. Near total decompression of the lesion was done when the BAER showed increased latency, which is when further excision was stopped.
Histopathological examination revealed the lesion to be a CM.
Postoperative period was uneventful. Patient's symptoms subsided completely with no neurological deficits. There was no postoperative rebleed seen from the residual lesion. Postoperative MRI showed a small residual lesion on the medial side of the operative cavity.
Case 3
A 47-year-old male presented with a subacute onset left-sided facial numbness and right-sided deviation of angle of mouth for 1 month. On examination, there was hypoesthesia in the left V1 and V2 divisions and left UMN Upper motor neuron (UMN) type of facial palsy. There were no other deficits.
MRI brain showed a left pontomedullary lesion with a dorsal component abutting into the fourth ventricle with similar imaging characteristics as the other 2 lesions [[Figure 2]].

Lesion was approached through a suboccipital craniotomy and a trans-fourth ventricular approach. Intraoperative monitoring was similar to what was used in the previous cases. Lesion was found to be abutting into the fourth ventricle with the surrounding brainstem-stained xanthochromic due to the bleed [[Figure 2]]. Lesion was capsulated with partial liquefaction of the hematoma. There was a good plane between the lesion and the surrounding brain. Complete excision of the lesion in a piecemeal fashion was done.
Histopathologically, the lesion was proved to be a cavernoma.
Postoperatively, the facial numbness partially subsided. There was persistent left UMN type of facial palsy. The patient also developed a left abducens nerve palsy postoperatively. Postoperative MRI showed complete excision of the lesion [[Figure 2]]. At 3-month follow-up, there was complete improvement in the facial and abducens nerve palsy along with the facial numbness.
Discussion
Epidemiology
Relapse and remission are the two most common words used in correlation with the natural history of CMs. Cavernomas may be single or multiple; familial or sporadic in occurrence, and congenital or de novo in evolution. The true natural history of these familiar lesions is yet unclear despite so many studies on the topic.[[14]] They are low flow vascular malformations.[[3]] The most common location of CMs in the brain stem is the pons followed by the midbrain and medulla. BSCs constitute 8.5%–35% of all symptomatic intracranial cavernomas.[[14]]
Clinical presentation
BSCs can have a varied clinical presentation. About 40% of the patients remain asymptomatic till the first episode of bleed. Patients with hemorrhage may present with subjective symptoms such as headache, vomiting, giddiness, nausea, altered sensorium or rarely, and trigeminal neuralgia.[[1]],[[3]],[[10]] However, episodes of loss of consciousness or cardiorespiratory failure though reported are rare. Focal neurological deficits can manifest in the form of cranial nerve (CN) palsies, motor/sensory deficits, or cerebellar signs. The deficits may fluctuate in their degrees of severity and combination depending on location, size of the lesion, hemorrhagic episodes-single or recurrent, and extent of hemorrhage. There is a direct interaction between the persistence of neurological deficits and the intervening time duration of hemorrhage. Symptoms are usually subacute in onset with gradual progression over hours to days. Neurological deficits usually improve with time and some authors have reported up to 37% of complete recovery.[[1]],[[2]],[[4]],[[10]],[[15]]
Radiology
MRI is the optimal standard for the diagnosis of cavernomas. The radiographic appearance is variable, depending on the stage of hemorrhage. The classical description of CMs is known as the “popcorn,” with a central area of heterogeneous signal on T1 and T2WI, surrounded by a ring of hemosiderin, which is hypointense on T2WI. T1 and fluid-attenuated inversion recovery images are helpful in defining the boundaries of the CM and to assess how close the CM is to the pial surface. T2 MRI should not be used for this assessment as the “blooming” artifact of the peripheral hemosiderin content provides a false and often exaggerated assessment of the CMs. The most sensitive sequence to detect cavernomas is the gradient echo T2 or the SWI sequences because of the magnetic susceptibility of products generated by degradation of hemoglobin. SWI sequences are also used to screen the brain and cord to look for multiple lesions in familial cases.[[3]],[[10]] Diffusion tensor imaging allows for the visualization of white matter tracts, thus improving the anatomical localization of corticospinal and sensory tracts preoperatively. The relationship between the lesion and the dislocated fiber tracts can be displayed in a three-dimensional manner, facilitating the preoperative planning of the surgical approach.[[6]],[[7]],[[10]]
Hemorrhage rate
Hemorrhage rate in cerebral CMs is the most researched aspect of their natural history. A thorough literature search on the natural history of CMs and BSCs has revealed variable hemorrhagic rates with considerable controversy with regard to it. Unruptured CMs have a relatively low prospective risk of hemorrhage (0.4%–0.6% per patient-year). Annual rates of hemorrhage range from 2.3% to 13.6% and rebleeding rates vary between 5% and 21.5% in various studies.[[2]],[[10]],[[14]] There is a significant range in the variability in the annual hemorrhagic rate from 15% to 60.9% as quoted by various authors such as Taslimi et al.,[[4]] Horne et al., and others.[[1]],[[5]],[[16]],[[17]] However, there are various confounding factors that could have led to this large variability, thus making it difficult to bank on any result till date. From all the studies analyzed, we report an overall annual hemorrhage rate of 2.5% per patient-year for cerebral CMs (95% confidence interval 1.3%–5.1%).[[1]],[[2]]
Definition of hemorrhage
The diverse hemorrhagic rate available in the literature could also be due to the fact that there is no standardized definition on the term “hemorrhage” or “recurrent hemorrhage” till date. Very few studies have attempted to bring about clarity amidst this muddle. Al-Shahi Salman et al.[[18]] in his systematic analysis concluded that the available data were inconclusive about the following aspects such as confirmatory imaging, whether the hemorrhage should be clinically symptomatic and whether it could extend beyond the CM or not. He thus defined a CM hemorrhage as “the one having acute or subacute onset of symptoms (any of headache, epileptic seizure, impaired consciousness, or new/worsened focal neurological deficit referable to the anatomic location of the CM) accompanied by radiological, pathological, surgical, or rarely only cerebrospinal fluid evidence of recent extra- or intra-lesional hemorrhage.” The definition includes neither an increase in CM diameter without other evidence of recent hemorrhage, nor the existence of a hemosiderin halo. Studies quoting rehemorrhage rates based only on the clinical parameters could be erroneously overrating it as there could be other clinical factors such as edema or thrombosis that can cause alterations in the clinical events. Only studies defining rehemorrhage based on clinical parameters, with MRI confirmation of the hemorrhage will provide a more accurate estimation which will understandably be smaller than the current record.[[18]],[[19]]
Time of presentation
Time is the single most important factor in determining bleeding rates. Since CMs can be congenital, radiation-induced, or de novo in origin, the assumption that the bleed was from a congenital lesion thus neglecting the ones from de novo lesions makes it not only an erroneous estimate but an underrated one too. Thus, making the current literature quite unaccountable for this bias as there is no way in differentiating the two from any of the studies available in literature.[[6]],[[20]],[[21]]
Patient selection
The studies quoted in literature have only considered patients with symptomatic hemorrhage, neglecting the asymptomatic ones, thus making it a selection bias. Based on this bias, it can be safely concluded that the rehemorrhage rates are inaccurate as well. Only the selected cohort of symptomatic cases referred to tertiary care centers and institutes are the ones considered for surgical series. The asymptomatic ones and patients with surgical contraindications are not considered at all, thus making it a referral bias. Evidently, these clustered cases have a higher hemorrhagic risk than the asymptomatic patients contributing to higher rebleed rates. In prospective studies which determine the natural history, asymptomatic patients and incidentally detected nonsymptomatic patients are recruited, excluding the patients who require surgical intervention. Thus, underestimating the bleeding risk, making it a selection bias. The time duration and the sample size of a study are influential in the assessment of bleeding risk. The risk of hemorrhage reduces with time, most often after the first 2 years of hemorrhage, thus proving that short follow-up periods are likelier to cite higher hemorrhagic risk. When the sample size is small, the values are erroneous as they can neither represent the population in a statistically significant manner nor the natural history of the disease.[[1]],[[2]],[[4]],[[9]],[[19]],[[21]],[[22]]
Hemorrhage risk factors
Various studies in literature quote a multitude of risk factors for hemorrhage in CM/BSC [[Table 1]]. Female sex, patient age, associated developmental venous anomaly (DVA), perilesional edema, large lesion size, history of previous ictus, deep location/brainstem, and multiplicity of CMs have been reported to affect the risk of bleeding. The percentage of risk among these are vacillating in their spread and report among the studies.[[1]],[[4]],[[18]],[[19]],[[22]],[[23]],[[24]]

Anatomical location
Porter et al.[[25]] reported a 30-fold greater rate of hemorrhage in infratentorial cavernomas than in supratentorial ones. Many studies report a significantly higher hemorrhagic rates of CM in the brain stem and other deep locations like the Basal Ganglia.[[1]],[[2]],[[14]],[[26]] Porter et al.,[[27]] in a prospective study of cerebral CMs, reported the deep location to be a significant factor influencing the clinical event risk. The reported rate of bleeding of 2.7%–6.0% per patient-year in BSC exceeds that of cavernomas (2.4%) in the other intracranial locations.[[2]],[[14]],[[19]],[[26]],[[28]] In a recent meta-analysis by Horne et al.[[17]] on the natural history of untreated cerebral CMs, 575 cases of BMC were included in the study. Brainstem location was independently associated with the occurrence of intracranial cerebral hemorrhage (30.8% 5-year risk bleed). The cause for this increased risk in the brain stem could be due to its structure and eloquence that makes it highly sensitive to even subtle changes in the lesion morphology which is absent in the lesions present elsewhere in the brain. Thus, in theory, leading to a discovery of a higher hemorrhagic rate.
Previous ictus
Several prospective studies pertaining the natural history of CMs and BSCs have reported that history of previous hemorrhage is a definitive risk factor for subsequent one;[[2]],[[18]],[[21]],[[22]] however, there are few authors like Kupersmith et al.[[29]] who have reported that there is no significant difference in the risk between the bled and unbled lesions.
Sex
Many prospective studies of natural history of cerebral CM show a higher predilection toward the female sex as a risk factor for bleeding. Li et al.[[21]] and Al-Shahi Salman et al.[[16]] in their prospective studies with 331 and 139 patients, respectively, along with other large series have statistically proved that the female sex is at a higher risk of bleed whereas there are a few studies that have opined that the female sex does not influence the risk of hemorrhage.[[1]],[[2]],[[5]],[[11]]
Age of the patients
The mean age of patients who present with symptomatic hemorrhages ranges between 32 and 38 years.[[10]] Many retrospective as well as prospective studies have opined that younger age (<40 years) has significantly higher risk of hemorrhage,[[5]],[[15]] although there are a few studies that have reported that age >50 years is a risk factor for bleed.[[21]]
Size of the lesion
Most of the studies such as Al-Shahi Salman et al.[[16]] and Kupersmith et al.[[29]] in their prospective studies report that lesions beyond 10 mm carry a greater risk of hemorrhage. Li et al.[[11]] in his retrospective analysis has concluded the same in lesions more than 20 mm. However, there are a few authors like Li et al.[[21]] who in his prospective analysis showed that lesion size did not significantly impact hemorrhage risk.
Developmental venous anomaly
DVAs are congenital anomalies of normal venous drainage, consisting of a number of dilated medullary veins converging into a single large draining vein, typically presenting with a caput medusae appearance. Some authors have reported that DVA has a higher risk of bleeding. The pathological basis to this is said to be that DVA affects the formation and clinical course of CMs by causing venous hypertension. Since DVAs are naturally vulnerable to hemodynamic changes, there is a significantly higher risk of bleed.[[1]],[[11]] However, not all studies of the natural history of CM have had similar results.[[1]],[[2]],[[16]]
Perilesional edema
It was found to be a significant predictor of hemorrhage in various studies. The pathological basis for this was hypothesized to be impaired venous drainage and formation of vascular connections between the lesions and the surrounding tissue. Edema also was related invasion and infiltration of the lesions into the brainstem, thus causing a higher risk of hemorrhage.[[11]],[[21]]
Other factors
Systemic arterial hypertension is said to be an attributable factor causing increased hemorrhagic risk in CMs. The pathological basis is touted to be the changes in arterial pressure that could cause meaningful alterations in the hemorrhagic propensity and patterns within the CM.[[1]],[[21]] Although hypertension is a risk factor, it has been specifically found that pregnancy is not a risk factor for bleeds in CM.[[1]]
Multiplicity of the lesions had no significant risk of hemorrhage on a per lesion basis as consistently seen in most of the studies. It only results in a cumulative increase in the hemorrhagic rate per patient.[[16]],[[21]]
Surgical intervention
In 1928, Dandy first resected a CM located in the pontomedullary region [[11]],[[30]] and since then, the advances in microsurgical techniques and technical aids such as intraoperative monitoring and neuronavigation have had tremendous progress. Complete surgical excision is the treatment of choice in BSCs. Surgical outcome with complete excision and good clinical outcomes is seen in many studies but along with it comes a high rate of immediate and long-term postoperative complications. Surgery in the brainstem is more often than not associated with morbidity and mortality owing to the compact nature and eloquence of the structure. Thus, understanding the natural history, evaluation of the preoperative deficits, thorough preoperative planning of the surgical approach, intraoperative adjuncts such as electrophysiological monitoring/neuronavigation and the surgeon's expertise is of utmost essence, not only for a safe resection and an acceptable postoperative outcome but also for a better quality of life.[[1]],[[10]],[[31]]
Indications for surgery
Surgical indications in BSC's have always been a controversial topic which has garnered varied viewpoints from surgeons across the globe [[Table 2]]. Although CMs are benign, with the asymptomatic lesions having a low hemorrhagic threshold, hemorrhage clustering with a higher rate of rebleeds ranging from 15% to 60% in the first 2 years following a bleed have been reported in all the major studies. Not only does the rebleed rate decline gradually after 2 years, the neurological deficits are also seen to improve spontaneously after a hemorrhage. Up to one-third of the patients make complete recovery with time. Thus, one of the most important indications for surgery is the need for early intervention after a symptomatic bleed, so as to prevent recurrence of hemorrhage. However, intervention must be deferred if the presentation is after 2 years of a bleed, as that in itself could cause new deficits.[[1]],[[4]],[[16]],[[17]],[[32]] Many authors have opined that it is reasonable to wait until after the second hemorrhage for a surgical intervention, as that puts the lesion under an “aggressive subset” which has a higher tendency to bleed than the others. Hence, the surgical risks in these patients are better accepted than the severity of the neurological risk following a subsequent bleed which can have disastrous consequences.[[1]],[[7]],[[10]],[[15]],[[28]] Thus, surgical consideration in symptomatic patients after the first or the second bleed would be the most appropriate time.

Some authors are of the opinion that symptomatic lesions should be operated when they are close to the pial surface or accessible through the safe entry zones to prevent complications.[[8]],[[15]],[[24]],[[26]],[[28]],[[32]],[[33]] When the lesion has caused significant mass effect on the surrounding structures resulting in altered consciousness or the need for life support, surgical intervention should be immediate irrespective of the presence or absence of bleed. The ones in the medulla must be positively treated according to some studies to avoid further life-threatening events. Chen et al.[[34]] compared the initial and final neurologic states between conservative and surgical treatment groups and found no significant differences regardless of patient age. However, the surgical threshold must be lower in children as there is higher cumulative lifetime risk of hemorrhage.[[4]],[[7]],[[9]],[[10]],[[22]],[[26]],[[28]],[[32]] In the geriatric population, intervention after a symptomatic bleed is essential as the elderly are less tolerant to the functional damage, thus compromising on the quality of life with worse outcomes.[[14]] Deep-seated lesions, notably those which are inaccessible to the safe entry zones, carry a higher risk of immediate and long-term morbidity,[[35]] where only some have had impressive results after the removal of such catastrophic lesions.[[1]],[[26]] It is safer to have a “wait and watch policy” till further bleeding episodes in these patients as that might make the lesion more amenable to surgery by reaching closer to a pial surface.[[32]]
Surgical intervention is not preferred in asymptomatic patients, incidentally detected lesions, patients with mild/transient symptoms or patients with a single bleed having mild symptoms. Surgery should be deferred in patients with mild symptoms, especially when the intervention itself carries a risk of significant permanent symptoms.[[9]],[[10]],[[21]],[[26]],[[28]] The goal of surgery is to eliminate the risk of recurrent hemorrhage and to improve and stabilize preoperative function while minimizing surgical complications. Thus, complete excision is imperative to avoid renewed hemorrhage. The circumstances of leaving behind a residue are acceptable is when its anticipated that complete removal would have a high risk of permanent deficits.[[10]],[[25]],[[26]]
Timing of surgery
The objective of surgery in BSC is radical resection because partial removal is associated with a persistent and higher risk of hemorrhage from the residual lesion. Despite a few reports proposing surgery during the acute phase to decompress the brain stem, many recommend delaying surgery for about 4–6 weeks after a symptomatic hemorrhage unless the patient has a life-threatening need for intervention in the form of altered consciousness, cardiorespiratory instability, or progressive neurological deficits. Surgery during the first 2 weeks is not advisable since the hematoma is yet solid with perilesional edema is at its maximum, thereby increasing postoperative deficits. During the 4–6 weeks period, there is liquefaction of hematoma and the edema also subsides (steroids may be used to reduce edema), thus providing a natural buffer against surgery related trauma to the surrounding structures as the hematoma itself provides a good plane for dissection. Usually, after hematoma evacuation, there is adequate space that is obtained for the excision of the cavernoma without any need for retraction of the brain stem.[[1]],[[6]],[[7]],[[8]],[[10]],[[13]],[[14]],[[21]],[[22]],[[26]],[[33]],[[36]] Authors such as Pandey et al.,[[33]] Garcia et al.,[[8]] and Zaidi et al.[[15]] who have large series (>100 patients) recommend intervention after 4 weeks but before 8 weeks of bleed, coz a further delay in surgery as there is retraction and organization of the hematoma along with gliosis, hyaline degeneration, and calcifications leading to tight adherence between the CM and the surrounding parenchyma, making the dissection plane obscure thus increasing the likelihood of mechanical trauma from surgical manipulation.[[7]],[[8]],[[10]],[[13]],[[14]],[[21]],[[22]],[[26]],[[33]]
According to the foregoing opinions and our experience as reported in two cases, subacute-phase surgery (i.e., when the hematoma is liquefied) is useful for the complete excision of the lesion with a minimal damage to the surrounding structures.
Principles of surgery in brainstem cavernomas
Surgical management of developmental venous anomaly
There is a clear association between DVA and CM. About 16%–100% of CMs are found in association with DVA.[[36]] A few authors have had a positive correlation between DVA and bleeding risk of CM. Significant difference in the hemodynamic alterations around DVAs with and without CM was found. CMs associated with DVAs had a significantly higher bleeding and rebleeding risk compared to the ones without the association. Thus, hypothesizing that the abnormal hemodynamics of DVAs might induce the formation of CMs. The pathological basis to this is the chronically increased intraluminal pressure and the resulting reduced tissue perfusion leading to tissue hypoxia, stimulating a local increase in angiogenic factors, which would induce the formation of vascular malformations.[[10]],[[37]] Surgical management of DVA is yet another controversial topic that remains unclear till date. A few studies advocate complete removal of DVAs as they are promoting factors in the development of cerebral CMs and resection of the associated DVA components may prevent regrowth of a partially excised CM,[[1]],[[38]] whereas the others are of the opinion that complete removal can cause hemorrhagic infarction as these drain normal brain as well. However, leaving the DVAs intact carries a risk of residual CM which might result in rebleed.[[1]],[[10]],[[11]],[[39]] Zhang et al.[[39]] in his study has recommended complete excision of the CMs combined with the coagulation of the distal radicles in association with the CMs and preservation of the caput medusae and main trunk of the DVAs.
Choice of surgical approach
A good surgical approach must minimize the brain retraction and violation to the normal structures. The shortest distance from the pial surface to the lesion need not be the safest. The presence and position of DVAs also influence the choice of approach and trajectory.[[10]],[[37]] Cavalcanti et al.[[40]] and Giliberto et al.[[13]] have described various microsurgical safe entry zones and approaches based on the location of the lesion in great detail with both cadaveric pictures and exquisite figures. We have combined the work of these authors to give a summary of all the approaches and safe entry zones according to the locations [[Figure 3]] and [[Figure 4]].


Midbrain
The ventral and central areas of the midbrain can be reached through a transsylvian route with the classic pterional or the fronto-orbitozygomatic craniotomy with one of its numerous modifications and the midbrain is approached through the transsylvian route. The safe entry zone in this area is a narrow corridor lateral to the emergence of CN III between the superior cerebellar artery (SCA) and the posterior cerebral artery and medial to the pyramidal tract. Ventrolateral lesions of the midbrain can be reached either through the transsylvian route or though the subtemporal transtentorial approach. Ventrolateral lesions with a more caudal extension can also be approached through more complex skull base transpetrosal approaches that afford a wider and more lateral exposure for the lower midbrain, pons, and higher medulla.
Posterior midbrain is approached through median, lateral, and extreme lateral approaches depending on the location of the lesion. The lateral mesencephalic sulcus is considered the limit between the anterolateral midbrain and the posterior midbrain. Midline lesions are approached through median supracerebellar infratentorial route, which allows an adequate view of the posterior and posterolateral surface of the midbrain, quadrigeminal plate, as well as the posterolateral surface of the upper pons. This approach includes median, paramedian, and extreme lateral variants which provide access to different parts of the posterior midbrain. The occipital transtentorial approach is an alternative for patients with a steep tentorial slope. The supracerebellar infratentorial approach requires a craniotomy exposing the entire width of the transverse sinus as well as the confluence of sinuses to increase the angle of view by upward retraction of the sinus. The lateral supracerebellar infratentorial approach requires a paramedian craniotomy, again exposing the entire width of the transverse sinus. This provides access to the posterior portion of the ambient cistern, including the proximal portion of the trochlear nerve, the SCA, and the posterolateral aspect of the midbrain. The extreme-lateral supracerebellar infratentorial variant is performed through a retrosigmoid craniectomy, with full exposure of the transverse/sigmoid sinus junction. It allows for a more lateral view of the posterolateral midbrain than the lateral approach. The lateral mesencephalic sulcus is the safe entry zone in the posterolateral aspect. The lateral mesencephalic vein runs into the lateral mesencephalic sulcus, thus representing an easily identifiable surface landmark for this structure. In the medial posterior midbrain, two safe entry zones at the level of the supracollicular and infracollicular areas are identified. These are two narrow horizontal lines immediately above and below the lamina quadrigemina.[[8]],[[10]],[[11]],[[13]],[[32]],[[33]],[[41]] [[Table 3]].

Pons
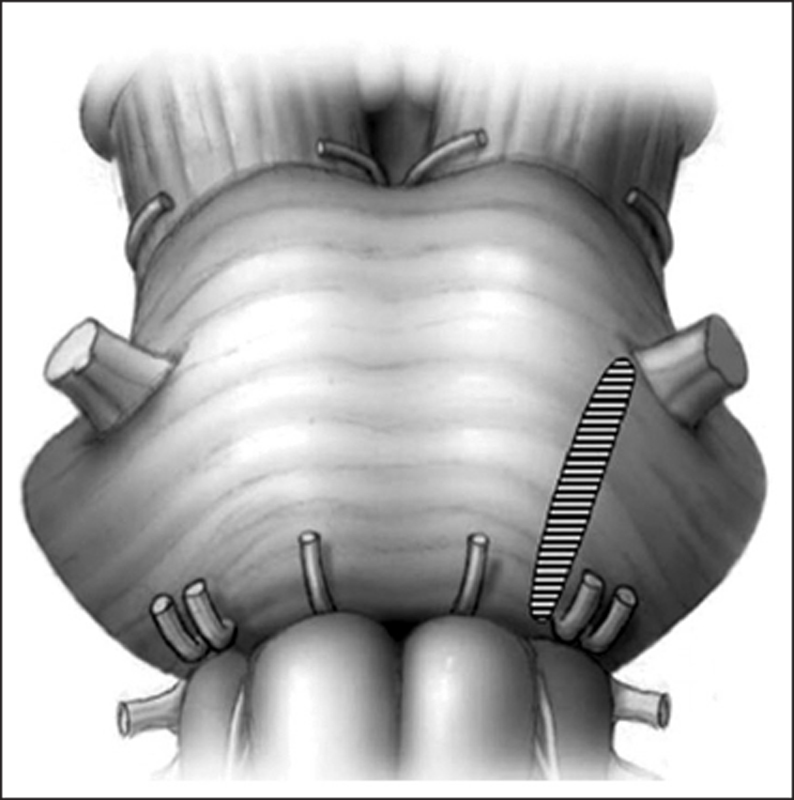
The ventrolateral and lateral areas of pons are accessed through the retrosigmoid approach and usually enter the brainstem between the trigeminal and facial nerves. For more ventral lesions, this approach can be extended by anterior mobilization of the skeletonized sigmoid sinus. The alternative routes to this area include the subtemporal transtentorial route (for lesions with more rostral extension), the presigmoid route, which provides a more lateral and direct view to the lesion or the transpetrosal approach. The safe entry zone into the lateral pons is the so-called “peritrigeminal area” between the emergence of CNs V and VII. This is an area located medially to the trigeminal nerve and laterally to the pyramidal tract [[Figure 5]].
Dorsal pontine area is approached by either a Telovelo tonsillar or a vermian split approach. The safe entry zone is through the floor of the fourth ventricle. They are the median sulcus above the facial colliculus, the suprafacial triangle (located immediately above the facial colliculus between the MLF and the cerebellar peduncles) and the infrafacial triangles (located immediately below the facial colliculus, lateral to the MLF, and is bordered inferiorly by the striae medullares and superolaterally by the facial nerve). However, these safe entry zones are useful only if the lesion is abutting the pial surface. In the cases, where the lesions are not approaching the surface, intraoperative electrophysiological monitoring and mapping of the floor are indispensable armaments to identify a safe corridor [[8]],[[10]],[[11]],[[13]],[[32]],[[33]],[[41]] [[Table 4]].

Medulla
The ventrolateral medullary lesions can be resected through a far-lateral approach through a lateral suboccipital craniectomy. For more ventral lesions, additional drilling of the occipital condyle may be required to achieve optimal exposure. A safe entry zone has been described in this region at the level of the retro-olivary sulcus or between CN XII and C-1 in the anterolateral sulcus.
The upper part of the dorsal medulla is approached through the floor of the fourth ventricle and is the same as the ones used to approach the dorsal pontine area. The lower dorsal medulla is approached by a median suboccipital craniotomy. The three safe entry zones for the posterior medulla: the posterior median fissure below the obex, the posterior intermediate sulcus between the gracile and cuneate fascicles, and the posterior lateral sulcus between the cuneate fascicle medially and the spinal trigeminal tract and nucleus laterally [[8]],[[10]],[[11]],[[13]],[[32]],[[33]],[[41]] [[Table 5]].

Microsurgical technique-keypoints
Repeated hemorrhagic episodes cause enlargement of the lesion and pushes it toward the pial surface causing a xanthochromic discoloration of the surrounding brain tissue and a dark blue area corresponding to the area of bulging hematoma at the pial surface. Such areas are the safest entry point for evacuation of BSC as there is no parenchymal covering over them.[[14]] The hemorrhagic event can be divided into two categories: extralesional and intralesional bleeding. The type of bleeding bears an effect on the surgical decompression. In extra-lesional bleeding, decreasing the mass effect of the hematoma with the excision of cavernoma itself and preserving the surrounding brainstem, is the easier than the intra-lesional bleeding, where complete removal may induce injury of the surrounding brainstem. Therefore, the extent of excision is controversial.[[14]]
The classic 2-point method can be used as an objective means to guide selection of the surgical approach.[[40]],[[42]] In this technique, 1 point is placed in the center of the CM and the second, closest to the pial surface/safe entry zone. The line connecting these 2 points is extended to the skull; this trajectory is used to select the most optimal surgical approach.[[7]] If there is a discrepancy between the shortest trajectory and approach through the safe entry zone, then, the latter should be preferred.
In most of the cases, the CN nuclei and white matter tracts are displaced by the lesions and in many cases the lesions do not surface to the pia. Hence, neuronavigation and electrophysiological monitoring techniques should be used to accurately locate the critical structures intraoperatively. Intraoperative monitoring includes evoked potentials such as SSEP, MEP, BAER, and direct CN monitoring. These provide real-time feedback about the progression of surgery. A baseline reading after position before the start of surgery is a must.[[10]],[[43]]
Lesion is approached through a parenchymal incision smaller than the lesion. Lesion should be internally decompressed first, followed by an attempt to develop a cleavage plane between the gliotic brain and lesion circumferentially. Piecemeal excision should be done with extremely gentle traction. If any resistance is felt, then, further dissection between the lesion and brain is resumed.[[43]]
Surgical outcomes
Surgical outcomes of BSCs with series more than 30 patients since 2010 have been analyzed and summarized in [[Table 6]], of which the largest study of 397 patients was reported by Zaidi et al.[[15]] These 15 studies included a total number of 1666 patients. The complete excision rate was 95% which was comparable with the meta-analysis. The early complication rate was about 32%, with improvement noted in 52.3%, worsening in 10%, and mortality in 2% of the patients. These values too were comparable with the other studies.[[2]]

The surgery of BSCs is always fraught with morbidity as seen in the outcome summary. The predictors of poor outcome that have been identified from the long-term studies are age >40–50 years, poor preoperative status, large lesion size, multiple hemorrhages, ventrally located lesions, presence of a DVA, postoperative rehemorrhage or second operation and time of surgical intervention after 6–8 weeks of bleeding.[[15]] In a recent publication, Garcia et al.[[8]] proposed a grading system for BSCs to help predict good long-term outcomes for patients undergoing resection. Proposed factors in the grading scale include patient age, lesion size, presence of a deep venous anomaly, extension across the midline, and hemorrhage, with a lower score indicating a greater likelihood of a good long-term outcome. The proposed factors in a comparison study between the long-term outcome between observation and surgery could give us a better indication about the correct therapeutic management. However, the results of such a study cannot be taken into account due to the selection bias involved between the cohorts. In the current case series, two patients had immediate improvement postoperatively. One patient developed a postoperative abducens nerve palsy which improved completely after 3 months.
Radiosurgery
Several studies report a decrease in hemorrhage rates after 2 years of radiosurgery. It is a nonsurgical method to control hemorrhage in CM. However, the use of radiosurgery is yet a controversial topic because the hemorrhage clustering in aggressive lesions also abates after 2 years according to the studies in natural history. Many authors believe that radiosurgery should be an alternative to observation but not to surgery, especially in aggressive lesions. Moreover, SRS might induce the developments of de novo CMs as well. Patients with deep-seated lesions which are surgically inaccessible, patients who have surgical contraindications and aggressive lesions can be considered for radiosurgery, but at marginal doses of 12–14 Gy to reduce procedure-related complications.[[10]],[[14]],[[28]],[[41]],[[46]]
Newer treatment modalities
Genetic analysis has revealed that CMs are linked to loss-of-function mutations in the genes encoding any of three structurally distinct proteins: KRIT1 (aka CCM1), OSM (aka CCM2), and PDCD10 (aka CCM3). Further studies have shown that these mutations resulted in RhoA hyperactivation and endothelial instability. Thus, leading to the hypothesis that reduction of RhoA hyperactivation with drugs, statins or fasudil, ameliorated the pathobiology caused by these mutations in genes for CCM1 and CCM2 (evidence for a role of PDCD10 [CCM3] in a similar pathway is not as strong as for the other 2 CCM genes), which has been shown in many animal studies. No human studies have been done to validate this information till date.[[47]],[[48]],[[49]]
Another new treatment modality is propranolol. There are a few case reports that have mentioned the usage of propranolol in patients with aggressive CMs. Apparently, this drug controls recurrence, de novo evolution of lesions and rehemorrhage, however, the pathophysiology behind the mechanism is yet unclear. Further clinical studies are required to validate the efficacy of this pharmacological agent.[[50]],[[51]] Thus, these alternatives such as SRS or propranolol can be used in patients with high surgical morbidity or any other significant surgical contraindications.
Conclusions
Although surgical excision has significant associated risks, it remains the primary therapeutic option for symptomatic BSCs to eliminate the risk of rebleeding. Surgery should be considered after the first or the second episode of hemorrhage as multiple rebleeds can cause exacerbation of deficits and sometimes mortality as well. Considering surgical timing, anywhere between 4 and 6 weeks or the subacute phase of the hemorrhage is considered appropriate. Accurate patient selection, careful preoperative planning, proper choice of the surgical approach, timing of surgery, meticulous microsurgical techniques, and intraoperative monitoring are mandatory to achieve a good clinical outcome. The aims of surgical intervention must be to improve preoperative function, minimize surgical morbidity and to reduce hemorrhagic rates. Other treatments, such as SRS and medications, might be alternatives for patients with deep-seated lesions or other significant surgical contraindications. Further prospective studies are required for a clear understanding of the natural history of the disease, thereby enabling surgeons to make the correct therapeutic choice to achieve a better surgical outcome.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Conflict of Interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
-
References
- 1 Xie MG, Li D, Guo FZ, Zhang LW, Zhang JT, Wu Z, et al. Brainstem cavernous malformations: Surgical indications based on natural history and surgical outcomes. World Neurosurg 2018;110:55-63.
- 2 Gross BA, Du R. Hemorrhage from cerebral cavernous malformations: A systematic pooled analysis. J Neurosurg 2017;126:1079-87.
- 3 Scavo CG, Roperto R, Cacciotti G, Mastronardi L. Cystic progression of a cavernous malformation at the level of the trigeminal root entry zone presenting with sudden onset of trigeminal neuralgia. J Craniofac Surg 2018;1.
- 4 Taslimi S, Modabbernia A, Amin-Hanjani S, Barker FG 2nd, Macdonald RL. Natural history of cavernous malformation: Systematic review and meta-analysis of 25 studies. Neurology 2016;86:1984-91.
- 5 Arauz A, Patiño-Rodriguez HM, Chavarria-Medina M, Becerril M, Longo GM, Nathal E, et al. Rebleeding and outcome in patients with symptomatic brain stem cavernomas. Cerebrovasc Dis 2017;43:283-9.
- 6 Farhoud A, Aboul-Enein H. Surgical management of symptomatic brain stem cavernoma in a developing country: Technical difficulties and outcome. Neurosurg Rev 2016;39:467-73.
- 7 Ren Y, Li J, Tao C, Zheng J, Zhang S, Xiao A, et al. Surgical treatment of cavernous malformations involving the midbrain: A Single-center case series of 34 patients. World Neurosurg 2017;107:753-63.
- 8 Garcia RM, Ivan ME, Lawton MT. Brainstem cavernous malformations: Surgical results in 104 patients and a proposed grading system to predict neurological outcomes. Neurosurgery 2015;76:265-77.
- 9 Abla AA, Lekovic GP, Garrett M, Wilson DA, Nakaji P, Bristol R, et al. Cavernous malformations of the brainstem presenting in childhood: Surgical experience in 40 patients. Neurosurgery 2010;67:1589-98.
- 10 Petr O, Lanzino G. Brainstem cavernous malformations. J Neurosurg Sci 2015;59:271-82.
- 11 Li D, Yang Y, Hao SY, Wang L, Tang J, Xiao XR, et al. Hemorrhage risk, surgical management, and functional outcome of brainstem cavernous malformations. J Neurosurg 2013;119:996-1008.
- 12 Abla AA, Lekovic GP, Turner JD, de Oliveira JG, Porter R, Spetzler RF, et al. Advances in the treatment and outcome of brainstem cavernous malformation surgery: A single-center case series of 300 surgically treated patients. Neurosurgery 2011;68:403-14.
- 13 Giliberto G, Lanzino DJ, Diehn FE, Factor D, Flemming KD, Lanzino G, et al. Brainstem cavernous malformations: Anatomical, clinical, and surgical considerations. Neurosurg Focus 2010;29:E9.
- 14 Negoto T, Terachi S, Baba Y, Yamashita S, Kuramoto T, Morioka M. Symptomatic brainstem cavernoma of elderly patients: Timing and strategy of surgical treatment. Two case reports and review of the literature. World Neurosurg 2018;111:227-34.
- 15 Zaidi HA, Mooney MA, Levitt MR, Dru AB, Abla AA, Spetzler RF, et al. Impact of timing of intervention among 397 consecutively treated brainstem cavernous malformations. Neurosurgery 2017;81:620-6.
- 16 Al-Shahi Salman R, Hall JM, Horne MA, Moultrie F, Josephson CB, Bhattacharya JJ, et al. Untreated clinical course of cerebral cavernous malformations: A prospective, population-based cohort study. Lancet Neurol 2012;11:217-24.
- 17 Horne MA, Flemming KD, Su IC, Stapf C, Jeon JP, Li D, et al. Clinical course of untreated cerebral cavernous malformations: A meta-analysis of individual patient data. Lancet Neurol 2016;15:166-73.
- 18 Al-Shahi Salman R, Berg MJ, Morrison L, Awad IA, Angioma Alliance Scientific Advisory Board. Hemorrhage from cavernous malformations of the brain: Definition and reporting standards. Angioma alliance scientific advisory board. Stroke 2008;39:3222-30.
- 19 Starke RM. Do brainstem cavernous malformations have a higher rate of hemorrhage? Expert Rev Neurother 2015;15:1109-11.
- 20 Ruggeri AG, Donnarumma P, Pichierri A, Delfini R. Two cystic cavernous angiomas after radiotherapy for atypical meningioma in adult woman: Case report and literature review. J Korean Neurosurg Soc 2014;55:40-2.
- 21 Li D, Hao SY, Jia GJ, Wu Z, Zhang LW, Zhang JT, et al. Hemorrhage risks and functional outcomes of untreated brainstem cavernous malformations. J Neurosurg 2014;121:32-41.
- 22 Li D, Hao SY, Tang J, Xiao XR, Jia GJ, Wu Z, et al. Surgical management of pediatric brainstem cavernous malformations. J Neurosurg Pediatr 2014;13:484-502.
- 23 Hu P, Liang J, Bao Y, Li M, Ling F. The pterional transsylvian transtentorial approach to ventrolateral pontine cavernomas: Indications and techniques. World Neurosurg 2014;82:1276-82.
- 24 Huang AP, Chen JS, Yang CC, Wang KC, Yang SH, Lai DM, et al. Brain stem cavernous malformations. J Clin Neurosci 2010;17:74-9.
- 25 Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, et al. Cavernous malformations of the brainstem: Experience with 100 patients. J Neurosurg 1999;90:50-8.
- 26 Wang CC, Liu A, Zhang JT, Sun B, Zhao YL. Surgical management of brain-stem cavernous malformations: Report of 137 cases. Surg Neurol 2003;59:444-54.
- 27 Porter PJ, Willinsky RA, Harper W, Wallace MC. Cerebral cavernous malformations: Natural history and prognosis after clinical deterioration with or without hemorrhage. J Neurosurg 1997;87:190-7.
- 28 Gross BA, Batjer HH, Awad IA, Bendok BR. Brainstem cavernous malformations. Neurosurgery 2009;64:E805-18.
- 29 Kupersmith MJ, Kalish H, Epstein F, Yu G, Berenstein A, Woo H, et al. Natural history of brainstem cavernous malformations. Neurosurgery 2001;48:47-53.
- 30 Gross BA, Batjer HH, Awad IA, Bendok BR, Du R. Brainstem cavernous malformations: 1390 surgical cases from the literature. World Neurosurg 2013;80:89-93.
- 31 Dukatz T, Sarnthein J, Sitter H, Bozinov O, Benes L, Sure U, et al. Quality of life after brainstem cavernoma surgery in 71 patients. Neurosurgery 2011;69:689-95.
- 32 Abla AA, Turner JD, Mitha AP, Lekovic G, Spetzler RF. Surgical approaches to brainstem cavernous malformations. Neurosurg Focus 2010;29:E8.
- 33 Pandey P, Westbroek EM, Gooderham PA, Steinberg GK. Cavernous malformation of brainstem, thalamus, and basal ganglia: A series of 176 patients. Neurosurgery 2013;72:573-89.
- 34 Chen L, Zhao Y, Zhou L, Zhu W, Pan Z, Mao Y, et al. Surgical strategies in treating brainstem cavernous malformations. Neurosurgery 2011;68:609-20.
- 35 Ferroli P, Sinisi M, Franzini A, Giombini S, Solero CL, Broggi G, et al. Brainstem cavernomas: Long-term results of microsurgical resection in 52 patients. Neurosurgery 2005;56:1203-12.
- 36 Zhang S, Li H, Liu W, Hui X, You C. Surgical treatment of hemorrhagic brainstem cavernous malformations. Neurol India 2016;64:1210-9.
- 37 Perrini P, Lanzino G. The association of venous developmental anomalies and cavernous malformations: Pathophysiological, diagnostic, and surgical considerations. Neurosurg Focus 2006;21:e5.
- 38 Knerlich-Lukoschus F, Steinbok P, Dunham C, Cochrane DD. Cerebellar cavernous malformation in pediatric patients: Defining clinical, neuroimaging, and therapeutic characteristics. J Neurosurg Pediatr 2015;16:256-66.
- 39 Zhang P, Liu L, Cao Y, Wang S, Zhao J. Cerebellar cavernous malformations with and without associated developmental venous anomalies. BMC Neurol 2013;13:134.
- 40 Cavalcanti DD, Preul MC, Kalani MY, Spetzler RF. Microsurgical anatomy of safe entry zones to the brainstem. J Neurosurg 2016;124:1359-76.
- 41 Frischer JM, Gatterbauer B, Holzer S, Stavrou I, Gruber A, Novak K, et al. Microsurgery and radiosurgery for brainstem cavernomas: Effective and complementary treatment options. World Neurosurg 2014;81:520-8.
- 42 Garrett M, Spetzler RF. Surgical treatment of brainstem cavernous malformations. Surg Neurol 2009;72 Suppl 2:S3-9.
- 43 Ohue S, Fukushima T, Kumon Y, Ohnishi T, Friedman AH. Surgical management of brainstem cavernomas: Selection of approaches and microsurgical techniques. Neurosurg Rev 2010;33:315-22.
- 44 Li H, Ju Y, Cai BW, Chen J, You C, Hui XH, et al. Experience of microsurgical treatment of brainstem cavernomas: Report of 37 cases. Neurol India 2009;57:269-73.
- 45 Ramina R, Mattei TA, de Aguiar PH, Meneses MS, Ferraz VR, Aires R, et al. Surgical management of brainstem cavernous malformations. Neurol Sci 2011;32:1013-28.
- 46 Lu XY, Sun H, Xu JG, Li QY. Stereotactic radiosurgery of brainstem cavernous malformations: A systematic review and meta-analysis. J Neurosurg 2014;120:982-7.
- 47 Chan AC, Li DY, Berg MJ, Whitehead KJ. Recent insights into cerebral cavernous malformations: Animal models of CCM and the human phenotype. FEBS J 2010;277:1076-83.
- 48 Li DY, Whitehead KJ. Evaluating strategies for the treatment of cerebral cavernous malformations. Stroke 2010;41:S92-4.
- 49 Faurobert E, Albiges-Rizo C. Recent insights into cerebral cavernous malformations: A complex jigsaw puzzle under construction. FEBS J 2010;277:1084-96.
- 50 Reinhard M, Schuchardt F, Meckel S, Heinz J, Felbor U, Sure U, et al. Propranolol stops progressive multiple cerebral cavernoma in an adult patient. J Neurol Sci 2016;367:15-7.
- 51 Zabramski JM, Kalani MY, Filippidis AS, Spetzler RF. Propranolol treatment of cavernous malformations with symptomatic hemorrhage. World Neurosurg 2016;88:631-9.
Address for correspondence
Publication History
Article published online:
09 September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Xie MG, Li D, Guo FZ, Zhang LW, Zhang JT, Wu Z, et al. Brainstem cavernous malformations: Surgical indications based on natural history and surgical outcomes. World Neurosurg 2018;110:55-63.
- 2 Gross BA, Du R. Hemorrhage from cerebral cavernous malformations: A systematic pooled analysis. J Neurosurg 2017;126:1079-87.
- 3 Scavo CG, Roperto R, Cacciotti G, Mastronardi L. Cystic progression of a cavernous malformation at the level of the trigeminal root entry zone presenting with sudden onset of trigeminal neuralgia. J Craniofac Surg 2018;1.
- 4 Taslimi S, Modabbernia A, Amin-Hanjani S, Barker FG 2nd, Macdonald RL. Natural history of cavernous malformation: Systematic review and meta-analysis of 25 studies. Neurology 2016;86:1984-91.
- 5 Arauz A, Patiño-Rodriguez HM, Chavarria-Medina M, Becerril M, Longo GM, Nathal E, et al. Rebleeding and outcome in patients with symptomatic brain stem cavernomas. Cerebrovasc Dis 2017;43:283-9.
- 6 Farhoud A, Aboul-Enein H. Surgical management of symptomatic brain stem cavernoma in a developing country: Technical difficulties and outcome. Neurosurg Rev 2016;39:467-73.
- 7 Ren Y, Li J, Tao C, Zheng J, Zhang S, Xiao A, et al. Surgical treatment of cavernous malformations involving the midbrain: A Single-center case series of 34 patients. World Neurosurg 2017;107:753-63.
- 8 Garcia RM, Ivan ME, Lawton MT. Brainstem cavernous malformations: Surgical results in 104 patients and a proposed grading system to predict neurological outcomes. Neurosurgery 2015;76:265-77.
- 9 Abla AA, Lekovic GP, Garrett M, Wilson DA, Nakaji P, Bristol R, et al. Cavernous malformations of the brainstem presenting in childhood: Surgical experience in 40 patients. Neurosurgery 2010;67:1589-98.
- 10 Petr O, Lanzino G. Brainstem cavernous malformations. J Neurosurg Sci 2015;59:271-82.
- 11 Li D, Yang Y, Hao SY, Wang L, Tang J, Xiao XR, et al. Hemorrhage risk, surgical management, and functional outcome of brainstem cavernous malformations. J Neurosurg 2013;119:996-1008.
- 12 Abla AA, Lekovic GP, Turner JD, de Oliveira JG, Porter R, Spetzler RF, et al. Advances in the treatment and outcome of brainstem cavernous malformation surgery: A single-center case series of 300 surgically treated patients. Neurosurgery 2011;68:403-14.
- 13 Giliberto G, Lanzino DJ, Diehn FE, Factor D, Flemming KD, Lanzino G, et al. Brainstem cavernous malformations: Anatomical, clinical, and surgical considerations. Neurosurg Focus 2010;29:E9.
- 14 Negoto T, Terachi S, Baba Y, Yamashita S, Kuramoto T, Morioka M. Symptomatic brainstem cavernoma of elderly patients: Timing and strategy of surgical treatment. Two case reports and review of the literature. World Neurosurg 2018;111:227-34.
- 15 Zaidi HA, Mooney MA, Levitt MR, Dru AB, Abla AA, Spetzler RF, et al. Impact of timing of intervention among 397 consecutively treated brainstem cavernous malformations. Neurosurgery 2017;81:620-6.
- 16 Al-Shahi Salman R, Hall JM, Horne MA, Moultrie F, Josephson CB, Bhattacharya JJ, et al. Untreated clinical course of cerebral cavernous malformations: A prospective, population-based cohort study. Lancet Neurol 2012;11:217-24.
- 17 Horne MA, Flemming KD, Su IC, Stapf C, Jeon JP, Li D, et al. Clinical course of untreated cerebral cavernous malformations: A meta-analysis of individual patient data. Lancet Neurol 2016;15:166-73.
- 18 Al-Shahi Salman R, Berg MJ, Morrison L, Awad IA, Angioma Alliance Scientific Advisory Board. Hemorrhage from cavernous malformations of the brain: Definition and reporting standards. Angioma alliance scientific advisory board. Stroke 2008;39:3222-30.
- 19 Starke RM. Do brainstem cavernous malformations have a higher rate of hemorrhage? Expert Rev Neurother 2015;15:1109-11.
- 20 Ruggeri AG, Donnarumma P, Pichierri A, Delfini R. Two cystic cavernous angiomas after radiotherapy for atypical meningioma in adult woman: Case report and literature review. J Korean Neurosurg Soc 2014;55:40-2.
- 21 Li D, Hao SY, Jia GJ, Wu Z, Zhang LW, Zhang JT, et al. Hemorrhage risks and functional outcomes of untreated brainstem cavernous malformations. J Neurosurg 2014;121:32-41.
- 22 Li D, Hao SY, Tang J, Xiao XR, Jia GJ, Wu Z, et al. Surgical management of pediatric brainstem cavernous malformations. J Neurosurg Pediatr 2014;13:484-502.
- 23 Hu P, Liang J, Bao Y, Li M, Ling F. The pterional transsylvian transtentorial approach to ventrolateral pontine cavernomas: Indications and techniques. World Neurosurg 2014;82:1276-82.
- 24 Huang AP, Chen JS, Yang CC, Wang KC, Yang SH, Lai DM, et al. Brain stem cavernous malformations. J Clin Neurosci 2010;17:74-9.
- 25 Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, et al. Cavernous malformations of the brainstem: Experience with 100 patients. J Neurosurg 1999;90:50-8.
- 26 Wang CC, Liu A, Zhang JT, Sun B, Zhao YL. Surgical management of brain-stem cavernous malformations: Report of 137 cases. Surg Neurol 2003;59:444-54.
- 27 Porter PJ, Willinsky RA, Harper W, Wallace MC. Cerebral cavernous malformations: Natural history and prognosis after clinical deterioration with or without hemorrhage. J Neurosurg 1997;87:190-7.
- 28 Gross BA, Batjer HH, Awad IA, Bendok BR. Brainstem cavernous malformations. Neurosurgery 2009;64:E805-18.
- 29 Kupersmith MJ, Kalish H, Epstein F, Yu G, Berenstein A, Woo H, et al. Natural history of brainstem cavernous malformations. Neurosurgery 2001;48:47-53.
- 30 Gross BA, Batjer HH, Awad IA, Bendok BR, Du R. Brainstem cavernous malformations: 1390 surgical cases from the literature. World Neurosurg 2013;80:89-93.
- 31 Dukatz T, Sarnthein J, Sitter H, Bozinov O, Benes L, Sure U, et al. Quality of life after brainstem cavernoma surgery in 71 patients. Neurosurgery 2011;69:689-95.
- 32 Abla AA, Turner JD, Mitha AP, Lekovic G, Spetzler RF. Surgical approaches to brainstem cavernous malformations. Neurosurg Focus 2010;29:E8.
- 33 Pandey P, Westbroek EM, Gooderham PA, Steinberg GK. Cavernous malformation of brainstem, thalamus, and basal ganglia: A series of 176 patients. Neurosurgery 2013;72:573-89.
- 34 Chen L, Zhao Y, Zhou L, Zhu W, Pan Z, Mao Y, et al. Surgical strategies in treating brainstem cavernous malformations. Neurosurgery 2011;68:609-20.
- 35 Ferroli P, Sinisi M, Franzini A, Giombini S, Solero CL, Broggi G, et al. Brainstem cavernomas: Long-term results of microsurgical resection in 52 patients. Neurosurgery 2005;56:1203-12.
- 36 Zhang S, Li H, Liu W, Hui X, You C. Surgical treatment of hemorrhagic brainstem cavernous malformations. Neurol India 2016;64:1210-9.
- 37 Perrini P, Lanzino G. The association of venous developmental anomalies and cavernous malformations: Pathophysiological, diagnostic, and surgical considerations. Neurosurg Focus 2006;21:e5.
- 38 Knerlich-Lukoschus F, Steinbok P, Dunham C, Cochrane DD. Cerebellar cavernous malformation in pediatric patients: Defining clinical, neuroimaging, and therapeutic characteristics. J Neurosurg Pediatr 2015;16:256-66.
- 39 Zhang P, Liu L, Cao Y, Wang S, Zhao J. Cerebellar cavernous malformations with and without associated developmental venous anomalies. BMC Neurol 2013;13:134.
- 40 Cavalcanti DD, Preul MC, Kalani MY, Spetzler RF. Microsurgical anatomy of safe entry zones to the brainstem. J Neurosurg 2016;124:1359-76.
- 41 Frischer JM, Gatterbauer B, Holzer S, Stavrou I, Gruber A, Novak K, et al. Microsurgery and radiosurgery for brainstem cavernomas: Effective and complementary treatment options. World Neurosurg 2014;81:520-8.
- 42 Garrett M, Spetzler RF. Surgical treatment of brainstem cavernous malformations. Surg Neurol 2009;72 Suppl 2:S3-9.
- 43 Ohue S, Fukushima T, Kumon Y, Ohnishi T, Friedman AH. Surgical management of brainstem cavernomas: Selection of approaches and microsurgical techniques. Neurosurg Rev 2010;33:315-22.
- 44 Li H, Ju Y, Cai BW, Chen J, You C, Hui XH, et al. Experience of microsurgical treatment of brainstem cavernomas: Report of 37 cases. Neurol India 2009;57:269-73.
- 45 Ramina R, Mattei TA, de Aguiar PH, Meneses MS, Ferraz VR, Aires R, et al. Surgical management of brainstem cavernous malformations. Neurol Sci 2011;32:1013-28.
- 46 Lu XY, Sun H, Xu JG, Li QY. Stereotactic radiosurgery of brainstem cavernous malformations: A systematic review and meta-analysis. J Neurosurg 2014;120:982-7.
- 47 Chan AC, Li DY, Berg MJ, Whitehead KJ. Recent insights into cerebral cavernous malformations: Animal models of CCM and the human phenotype. FEBS J 2010;277:1076-83.
- 48 Li DY, Whitehead KJ. Evaluating strategies for the treatment of cerebral cavernous malformations. Stroke 2010;41:S92-4.
- 49 Faurobert E, Albiges-Rizo C. Recent insights into cerebral cavernous malformations: A complex jigsaw puzzle under construction. FEBS J 2010;277:1084-96.
- 50 Reinhard M, Schuchardt F, Meckel S, Heinz J, Felbor U, Sure U, et al. Propranolol stops progressive multiple cerebral cavernoma in an adult patient. J Neurol Sci 2016;367:15-7.
- 51 Zabramski JM, Kalani MY, Filippidis AS, Spetzler RF. Propranolol treatment of cavernous malformations with symptomatic hemorrhage. World Neurosurg 2016;88:631-9.