

Subscribe to RSS
DOI: 10.1055/s-0046-1815943
Extensive Calvarial Reconstruction for Recurrent Scalp Malignant Proliferating Trichilemmal Tumor: Case Report
Authors

Abstract
Malignant proliferating trichilemmal tumor (MPTT) is a rare cutaneous neoplasm that arises from the external root sheath of the hair follicles, typically affecting sun-exposed areas such as the scalp, neck, and forehead; it is also misdiagnosed due to its resemblance to other skin neoplasms. This report highlights a rare case of a MPTT with repeated local recurrences, despite undergoing wide surgical resections and adjuvant radiotherapy in two different occasions. We present a case of a 42-year-old African − American man diagnosed with a MPTT of the scalp in 2013, which was treated with surgical excision and adjuvant radiotherapy. In the following years, the patient experienced several local recurrences with deeper involvement of the calvarial bone, requiring multiple additional procedures. In 2023, he underwent bifrontal, biparietal, and right temporal craniectomy for complete tumor excision, followed by a second course of radiotherapy and a further scalp reconstruction in early 2024. Subsequent imaging studies revealed no signs of recurrence, and biopsy results confirmed absence of residual tumor. This case exposes an unusually aggressive and treatment-refractory MPPT, which required multiple surgical procedures for wide resection, as well as two complete courses of radiotherapy, to achieve tumor control; these characteristics place this presentation among the most treatment-refractory forms of the disease reported to date. While radiotherapy has been reported as an effective alternative in cases of tumors resistant to surgery, our experience emphasizes the need for a multimodal strategy when recurrence is suspected, whether based on histopathological features or clinical presentation. This underscores the importance of early surgical intervention, multidisciplinary management, and close long-term follow-up in such rare and challenging tumors.
Introduction
Malignant proliferating trichilemmal tumor (MPTT) is a rare cutaneous neoplasm derived from the outer root sheath of hair follicles. It was first described by Wilson-Jones in 1966 as a neoplastic transformation of trichilemmal cysts, and since then, it has been recognized as a distinct pathology. MPTT typically arises from long-standing trichilemmal cysts that undergo progressive and rapid epithelial proliferation, up to malignant transformation.[1] Despite this, it is often misdiagnosed due to its clinical and histological resemblance to squamous cell carcinoma.[2]
These tumors most frequently arise on sun-exposed areas of the scalp and are predominantly seen in elderly women, although cases in younger individuals and men have been also documented.[3] Clinically, MPTT presents as a solitary nodule, often firm or ulcerated, with variable growth behavior. Some lesions remain indolent for years, while others demonstrate rapid expansion and aggressive local invasion.[4]
Histologically, MPTTs exhibit lobular proliferation of squamous epithelial cells with abrupt trichilemmal keratinization, nuclear pleomorphism, a high mitotic index, and absence of granular cell layer. In more aggressive forms, features such as necrosis, infiltrative margins, and stromal desmoplasia may also be present.[5] [6] These histologic characteristics are essential to distinguish MPTT from its benign counterpart and from other cutaneous neoplasms such as squamous cell carcinoma.[5] Immunohistochemistry can support diagnosis in uncertain cases; although not always necessary, markers such as p63, p53, CK 5,6,7,17, and Ki-67 have been reported as useful in confirming trichilemmal differentiation[7] [8]
There are no standardized treatment protocols for this pathology; surgical local excision with wide margins (1 cm) remains the cornerstone of treatment, as recurrences are common when margins are insufficient.[8] In selected patients with deep invasion or multiple recurrences, adjuvant radiotherapy has been employed with better results.[9] Here we present a case of a middle-aged African − American man with a particularly aggressive and recurrent MPTT of the scalp that required multiple surgical procedures and two courses of radiotherapy to achieve tumor control. This case highlights the therapeutic complexity of MPTT and the importance of multidisciplinary management in difficult presentations.
Case Report
A 42-year-old African − American man with a longstanding history of a scalp tumor lesion initially localized to the right temporal region was referred from dermatology. He had a history of a MPTT of the scalp, which was surgically resected in 2013 followed by 22 sessions of radiotherapy, the last of which was administered in November of the same year. Since then, he had been under regular dermatologic follow-up until 2019, when he developed an alopecic scar at the surgical site, which was subsequently biopsied ([Fig. 1]).

Histopathological analysis revealed epithelial neoplasm consistent with MPTT and immunohistochemical studies demonstrated tumor cell positivity for p63 and CK5, CK6, meaning recurrence of the disease ([Fig. 2]). Given these findings in 2019, the patient underwent a second surgical procedure, consisting of wide excision of the alopecic scar with 1-cm clean margins followed by skin grafting. Histopathological examination once again confirmed MPTT, with a Ki-67 proliferative index of 30% ([Fig. 3]). However, wound healing was suboptimal over the right parietotemporal region and the patient developed skull bone exposure, which led to a new reconstructive surgery. This time, a free latissimus dorsi flap was performed. The procedure proceeded as planned, with adequate postoperative recovery, satisfactory healing, and negative pathology until June 2022.


Approximately 3 years after the last surgical intervention and flap reconstruction, in late 2022, a new subcutaneous cystic lesion developed on the scalp near the previous surgical site. The lesion showed progressive growth over the following months, where imaging studies, including soft tissue ultrasound, MRI, and CT scans, revealed irregular margins, increased soft tissue density, and underlying bone involvement suggestive of tumor recurrence and progression ([Fig. 4]) including bone infiltration ([Fig. 5]). Based on these findings, dermatologic oncology was consulted and recommended wide resection of the affected area with 2-cm margins, including deeper resection of the involved bone, followed by adjuvant radiotherapy.


Surgical Procedure
In March 2023, under general anesthesia and with the patient in the supine position and head in neutral alignment, a wide bicoronal incision was performed. Subperiosteal dissection was performed to expose the previous surgical site, and after mobilization of the anterior and posterior scalp flaps, a friable, ulcerated, yellowish tumor involving the frontoparietal region was revealed and resected en-bloc down to the dura mater; necrotic tissue was collected for histopathological analysis.
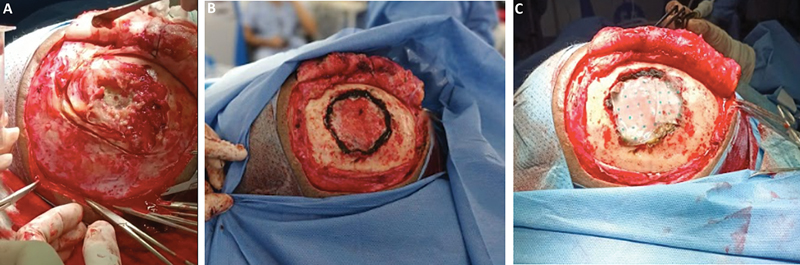
Upon evaluation of the bone, widespread infiltration was observed in the bifrontal and biparietal regions leading to a wide craniectomy using a high-speed drill and Kerrison rongeurs until macroscopically healthy bone margins were identified ([Fig. 6]). Tumor remnants involving the epidural space and the right frontobasal dura were carefully dissected and completely removed. The surgical field was thoroughly irrigated with an antiseptic solution, and hemostasis was achieved using hemostatic agents and Hemopatch application. Primary dural closure was performed, followed by multilayer scalp reconstruction, and both bone and soft tissue specimens were submitted for complete pathological evaluation. No intraoperative complications occurred, and the patient tolerated the procedure well.
Histopathological examination once again confirmed the diagnosis of MPTT; however, the surgical margins were free of tumor infiltration. Based on these findings, the patient underwent cranioplasty and a new scalp reconstruction with grafting.
Postoperative Period
Clinically, the patient experienced no further complications. Subsequent radiological follow-up in October 2024 showed no evidence of cerebrospinal fluid leak, infection, or radiological signs of tumor recurrence. Also, a follow-up biopsy confirmed the absence of tumor recurrence. As of the most recent evaluation, the patient has remained recurrence-free for two and a half years and continues under multidisciplinary follow-up.
Discussion
MPTT is an uncommon adnexal neoplasm that poses diagnostic and therapeutic challenges due to its histological similarity to squamous cell carcinoma and its unpredictable clinical course. While most cases follow an indolent behavior, some variants exhibit deep local invasion and resistance to the gold-standard treatment, which is the wide local excision with clean margins of healthy tissue.[3]
Recent reports have emphasized the role of histopathologic features—such as cytologic atypia, high mitotic index, necrosis, and infiltrative growth patterns—in identifying more aggressive forms.[6] In some instances, additional immunohistochemical findings, including p53 and p63 overexpression, elevated Ki-67, reduced CD34 expression, and CK5, CK6, CK7, and CK17 expression, have also supported malignant behavior and lower differentiation.[10] [11] Our case presented histopathological findings such as atypical nuclei and trichilemmal keratinization within the tumor cell nests, as well as sarcomatoid areas consistent with malignant transformation. The tumor cells were positive for periodic acid-Schiff staining, and immunohistochemical analysis demonstrated positivity for p63, CK5, CK6, and vimentin, with a Ki-67 proliferation index of 30% supporting the aggressive biological behavior of the lesion. There was negative expression for AML, desmin, and CD34—a profile that, although differing from the classical pattern of CD34 positivity, has been previously reported in MPTT with sarcomatoid components.[12] These aggressive histopathological features mentioned in the literature and also observed in our case, indicted a higher likelihood of aggressive behavior, which was the actual course of our case.
The patient underwent multiple surgical procedures including wide local excisions and extensive craniectomy, and proved to be refractory to standard management approaches with repeated recurrences despite performing local excisions with wide margins and using adjuvant radiotherapy, requiring multimodal treatment strategies. Abdelhammed et al described a case of high-risk MPTT also treated with surgery and adjuvant radiotherapy; although in their case no recurrences were observed during follow-up; the authors emphasized the importance of rigorous postoperative surveillance in tumors with aggressive histological and clinical features.[10] Radiological imaging plays an important role in this context. CT and MRI with contrast, as well as PET scan, are essential not only for local staging but also to assess deep extension, bone involvement, and potential distant spread in advanced disease.[11] [13]
When MPTT involves calvarial bone like the case presented above, a more extensive surgical procedure is required. In our case, as in the MPTT case reported by Kemaloğlu et al the patient had bone invasion requiring wide excision with 1-cm surgical margin followed by adjuvant postoperative radiotherapy, highlighting the complexity of managing malignant presentations of MPTT.[14] In our patient, progressive tumor invasion made necessary a bifrontal, biparietal, and right temporal craniectomy followed by cranioplasty and scalp reconstruction. For large previously irradiated scalp defects, the latissimus dorsi free flap has proven to be a reliable option, providing durable vascularized coverage with better functional and aesthetic outcomes.[15]
Although radiotherapy is not part of the standard management, it has been used in selected recurrent cases or when surgery is not completely effective. Sutherland et al reported a complete clinical response following radical radiotherapy alone in a case of MPTT,[16] [17] [18] [19] [20] [21] in addition to previously cited reports, most of which describe the use of surgery combined with radiotherapy. Still, the decision to use radiotherapy must be individualized. Primarily employed in malignant and recurrent presentations, in our case, the decision to initiate radiotherapy in our patient was based on the tumor's aggression, histopathological features, and repeated recurrences despite multiple surgical approaches, reflecting its refractory and locally infiltrative course.
While craniotomy combined with radiotherapy for MPTT has indeed been reported, the rarity of our case lies in the combination of clinical features: (1) repeated local recurrences despite wide-margin resections; (2) two complete courses of adjuvant radiotherapy; (3) progressive and extensive calvarial involvement requiring a bifrontal, biparietal, and right temporal craniectomy; and (4) the need for multiple reconstructive procedures, including free flap and subsequent cranioplasty. Few published cases describe such extensive bony involvement or the need for repeated oncologic and reconstructive procedures. To contextualize the present case within the existing literature, we compiled all previously reported cases of recurrent MPTT requiring multiple surgical resections or dual treatment with radiotherapy ([Table 1]). These reports demonstrate that, although recurrence is uncommon, tumors with aggressive histopathological features may require repeated excisions and, in rare cases, calvarial resection with adjuvant radiotherapy. However, this combined approach is usually sufficient to prevent recurrences, unlike our case, which required multiple surgical procedures and even two sessions of radiotherapy. These features highlight the exceptionally aggressive and treatment-refractory nature of this tumor, distinguishing it from previously reported MPTT cases requiring craniotomy.
|
Author, year |
Study sample |
Tumor location |
Number of surgeries |
Recurrence/radiotherapy |
Salient findings |
|---|---|---|---|---|---|
|
Park et al (1997)[17] |
One patient with MPTT of the scalp |
Occipital scalp |
Three (initial wide excision + two re-excisions for recurrence) |
Two local recurrences. RT: Not mentioned/No evidence |
Tumor evolved over 10 y with progressively aggressive behavior. After two local recurrences, developed multiple distant metastases (cervical lymph nodes, periparotid region, chest). Histology showed increasing nuclear atypia and rising Ki-67 positivity correlating with progression. |
|
Bae et al (2001)[18] |
One patient with MPTT of the scalp |
Occipital scalp |
Three (initial excision + re-excision at 4 mo + surgery for metastatic disease) |
One local recurrence, followed by metastatic progression. RT: No. Chemo: Yes (cisplatin + etoposide) |
Aggressive clinical course with early local recurrence and rapid progression to distant metastases including CNS involvement. Despite repeated surgeries and combination chemotherapy, disease continued to disseminate. Underscores potential for highly malignant behavior in MPTT including rapid recurrence, metastatic spread, and poor response to treatment. |
|
Rao et al (2011)[19] |
One patient with MPTT of the scalp and postauricular region |
Parieto-occipital and postauricular scalp |
Three procedures (prior benign excisions + wide excision for recurrent MPTT) |
Multiple local recurrences (tumor recurred within 2 mo after previous excision). RT: No |
Patient had history of multiple prior excisions of benign trichilemmal tumors. Most recent recurrence required wide excision for definitive management. No adjuvant therapy including radiotherapy or chemotherapy administered. Patient remained recurrence-free at 1-y follow-up. |
|
Fieleke et al (2015)[20] |
One patient with MPTT of the frontal scalp |
Frontal scalp |
Two (initial excision + Mohs re-excision) |
One (residual tumor addressed surgically − margins positive after initial excision). RT: Not specified |
Residual tumor present after initial excision with positive margins. Second surgery using Mohs micrographic technique performed to achieve clear margins. No recurrence reported after Mohs. Radiotherapy not specified for this patient, although adjuvant radiotherapy can be considered in MPTT due to tumor aggressiveness. |
|
Osto et al (2021)[4] |
65 patients with MPTT of the scalp |
Scalp |
Surgery in 61/65 patients (93.8%). Several patients required repeat surgeries for recurrences |
11/45 with follow-up (24.4%) had one or multiple recurrences (local, nodal, or metastatic). Pattern: One or multiple recurrences requiring repeat surgeries. RT: Yes (adjuvant in aggressive/recurrent cases) |
Systematic review of 65 MPTT cases. Patients typically presented with slow-growing scalp mass. Recurrence notable: 24.4% of followed patients had recurrences, often requiring repeat surgery. Regional lymph-node spread (15.4%) and distant metastasis (9.2%) also observed. Surgery—preferably Mohs—remains main treatment, with RT/chemo used in aggressive or recurrent cases. |
|
Virdi et al (2021)[21] |
One patient with MPTT of the scalp eroding calvarium and extending intracranially |
Scalp with full-thickness calvarial erosion and intracranial extension |
≥10 total (nine prior surgeries over 34 y + 1 diagnostic excision). Final surgery: limited excision only (patient declined wide excision) |
Multiple recurrences (benign-appearing lesions over 34 y, then malignant transformation). RT: Yes (66 Gy, definitive treatment) |
Patient had 10 prior scalp surgeries over 34 y for recurrent benign-appearing lesions. Bone erosion and intracranial extension highlight that recurrent trichilemmal lesions can undergo malignant transformation and invade deeply, requiring preoperative imaging, MDT management, and sometimes nonsurgical definitive therapy. Radical radiotherapy achieved good early response in this surgically high-risk case. |
|
Kemaloğlu et al (2022)[14] |
Four patients with MPTT of the scalp |
Scalp |
Case 2 (M, 69): two surgeries (initial excision with 2-mm positive margin + re-excision with 5-mm margin). Other cases (Cases 1, 3, 4): Single surgery with 1-cm margins + adjuvant RT |
Case 2: One local + metastatic recurrence at 20 mo. RT: Planned but not delivered. Chemo: Yes. Other cases: zero recurrences. RT: Yes (50–60 Gy) |
Only case 2 required more than one surgery and later developed metastatic recurrence despite re-excision and chemotherapy. The remaining three patients (cases 1, 3, 4), all of whom received adjuvant radiotherapy, showed no recurrence during follow-up. Authors emphasize that even tumors with low Ki-67 and no local invasion can behave aggressively, suggesting all MPTT patients may benefit from adjuvant radiotherapy. |
|
Kearns-Turcotte et al (2022)[6] |
Four cases of MPTT of the scalp and back |
Scalp/back |
Case 3: two surgeries (initial excision + Mohs + deep margin resection/reconstruction). Other cases (Cases 1, 2, 4): Single-session surgical management (wide local excision) |
Case 3: Zero recurrences. RT: No. Other cases: Zero recurrences. RT: No. Follow-up: 5–36 mo |
Across the series, no patient developed local recurrence during follow-up. Case 3 initially misdiagnosed as lipoma, requiring staged surgeries after MPTT discovered histologically, demonstrating how diagnostic uncertainty can lead to multiple procedures. Case 1 underwent extensive initial excisions of multiple tumors with flap and graft reconstruction (single-session). Although recurrence is absent in these cases, literature highlights MPTT can recur and occasionally metastasize, reinforcing need for complete margin control and close follow-up. |
Abbreviations: Chemo, chemotherapy; CNS, central nervous system; F, female; Gy, gray; M, male; MDT, multidisciplinary team; MPTT, malignant proliferating trichilemmal tumor; RT, radiotherapy.
Long-term follow-up is crucial given the potential for delayed recurrence of the MPTT. Several reports emphasize the importance of close clinical and radiological surveillance, particularly in patients with histologically and clinically aggressive features.[8] In our experience, multidisciplinary care and consistent monitoring were essential for achieving tumor control in this unusually aggressive case.
Conclusion
This case underscores that MPTT, though uncommon, can follow an unusually aggressive and unpredictable course. Beyond the well-documented potential for local invasion, our patient exhibited a rare combination of features—multiple recurrences despite wide resections, two full courses of radiotherapy, progressive calvarial destruction requiring bifrontal, biparietal, and temporal craniectomy, and the need for repeated reconstructive procedures. These characteristics place this presentation among the most treatment-refractory forms of the disease reported to date. Recognizing early histopathological markers of aggressiveness, ensuring complete excision with clear margins, and planning radiotherapy and reconstruction as part of a coordinated, staged strategy remain critical for optimizing outcomes in such complex cases. Continuous long-term surveillance is essential, as even initially controlled lesions may evolve toward extensive and structurally destabilizing involvement.
Conflict of Interest
None declared.
Authors' Contributions
F.A.-M. diagnosed the patient, supervised and contributed to the final version of the manuscript. P.A.V.-A. collected the data and wrote the first draft of the manuscript with the help of M.C.B.-L. and I.A.F.-F. M.C.B.-L. described the images used in the article with the help of I.A.F.-F. and P.A.V.-A. All authors provided critical feedback and contributed to the writing of the manuscript.
Ethical Approval
The study was conducted according to the principles established in the Declaration of Helsinki.
Patients' Consent
Informed consent was obtained from all the participants of the study.
-
References
- 1 Sau P, Graham JH, Helwig EB. Proliferating epithelial cysts. Clinicopathological analysis of 96 cases. J Cutan Pathol 1995; 22 (05) 394-406
- 2 Weiss J, Heine M, Grimmel M, Jung EG. Malignant proliferating trichilemmal cyst. J Am Acad Dermatol 1995; 32 (5 Pt 2): 870-873
- 3 Singh P, Usman A, Motta L, Khan I. Malignant proliferating trichilemmal tumour. BMJ Case Rep 2018; 2018: bcr2018224460
- 4 Osto M, Parry N, Rehman R, Ahmed U, Mehregan D. Malignant proliferating trichilemmal tumor of the scalp: a systematic review. Am J Dermatopathol 2021; 43 (12) 851-866
- 5 Kini JR, Kini H. Fine-needle aspiration cytology in the diagnosis of malignant proliferating trichilemmal tumor: report of a case and review of the literature. Diagn Cytopathol 2009; 37 (10) 744-747
- 6 Kearns-Turcotte S, Thériault M, Blouin MM. Malignant proliferating trichilemmal tumors arising in patients with multiple trichilemmal cysts: a case series. JAAD Case Rep 2022; 22: 42-46
- 7 Jiang XL, Yang Y, Lei SR. Proliferating trichilemmal tumor of the scalp: a case report and literature review. Clin Surg J 2022; 3 (03) 1-6
- 8 Joshi TP, Marchand S, Tschen J. Malignant proliferating trichilemmal tumor: a subtle presentation in an African American woman and review of immunohistochemical markers for this rare condition. Cureus 2021; 13 (08) e17289
- 9 Cavanagh G, Negbenebor NA, Robinson-Bostom L, Walker JL. Two cases of malignant proliferating trichilemmal tumor (MPTT) and review of literature. R I Med J (2013) 2022; 105 (01) 12-16
- 10 Abdelhammed MH, Siatecka H, Diwan AH. et al. A rare case of a malignant proliferating trichilemmal tumor: a molecular study harboring potential therapeutic significance and a review of literature. Dermatopathology (Basel) 2024; 11 (04) 354-363
- 11 Sun J, Zhang L, Xiao M. et al. Systematic analysis and case series of the diagnosis and management of trichilemmal carcinoma. Front Oncol 2023; 12: 1078272
- 12 Moran JMT, Hoang MP, Mariño-Enríquez A, DeSimone MS. Malignant proliferating pilar tumor with sarcomatous transformation (“carcinosarcoma”): case report with molecular profile. Am J Dermatopathol 2025; 47 (01) 65-69
- 13 Boeisa AN, Alkhars AM, Albaqshi AA, Al-Arbash MS, Alqatari MA, Mohammad Mousa IA. A proliferating trichilemmal tumor at an uncommon site treated with radical excision: a case report and literature review. Cureus 2024; 16 (07) e64803
- 14 Kemaloğlu CA, Öztürk M, Aydın B, Canöz Ö, Eğilmez O. Malignant proliferating trichilemmal tumor of the scalp: report of 4 cases and a short review of the literature. Case Reports Plast Surg Hand Surg 2022; 9 (01) 158-164
- 15 Islam AFMA, Ahmed MI, Uddin MS, Hamid MA. Outcome of latissimus dorsi free flap in-case of large scalp defect: a single center study. Int Surg J 2021; 8 (12) 3678-3682
- 16 Sutherland D, Roth K, Yu E. Malignant proliferating trichilemmal tumor treated with radical radiotherapy: A case report and literature review. Cureus 2017; 9 (01) e999
- 17 Park BS, Yang SG, Cho KH. Malignant proliferating trichilemmal tumor showing distant metastases. Am J Dermatopathol 1997; 19 (05) 536-539
- 18 Bae SB, Lee KK, Kim JS. et al. A case of malignant proliferating trichilemmoma of the scalp with multiple metastases. Korean J Intern Med (Korean Assoc Intern Med) 2001; 16 (01) 40-43
- 19 Rao S, Ramakrishnan R, Kamakshi D, Chakravarthi S, Sundaram S, Prathiba D. Malignant proliferating trichilemmal tumour presenting early in life: an uncommon feature. J Cutan Aesthet Surg 2011; 4 (01) 51-55
- 20 Fieleke DR, Goldstein GD. Malignant proliferating trichilemmal tumor treated with Mohs surgery: proposed protocol for diagnostic work-up and treatment. Dermatol Surg 2015; 41 (02) 292-294
- 21 Virdi A, Borghol K, Edwards B, Barnard N. Scalp malignant trichilemmal tumour with bony erosion: a new clinical entity. BMJ Case Rep 2021; 14 (05) e239161
Address for correspondence
Publication History
Article published online:
09 February 2026
© 2026. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Sau P, Graham JH, Helwig EB. Proliferating epithelial cysts. Clinicopathological analysis of 96 cases. J Cutan Pathol 1995; 22 (05) 394-406
- 2 Weiss J, Heine M, Grimmel M, Jung EG. Malignant proliferating trichilemmal cyst. J Am Acad Dermatol 1995; 32 (5 Pt 2): 870-873
- 3 Singh P, Usman A, Motta L, Khan I. Malignant proliferating trichilemmal tumour. BMJ Case Rep 2018; 2018: bcr2018224460
- 4 Osto M, Parry N, Rehman R, Ahmed U, Mehregan D. Malignant proliferating trichilemmal tumor of the scalp: a systematic review. Am J Dermatopathol 2021; 43 (12) 851-866
- 5 Kini JR, Kini H. Fine-needle aspiration cytology in the diagnosis of malignant proliferating trichilemmal tumor: report of a case and review of the literature. Diagn Cytopathol 2009; 37 (10) 744-747
- 6 Kearns-Turcotte S, Thériault M, Blouin MM. Malignant proliferating trichilemmal tumors arising in patients with multiple trichilemmal cysts: a case series. JAAD Case Rep 2022; 22: 42-46
- 7 Jiang XL, Yang Y, Lei SR. Proliferating trichilemmal tumor of the scalp: a case report and literature review. Clin Surg J 2022; 3 (03) 1-6
- 8 Joshi TP, Marchand S, Tschen J. Malignant proliferating trichilemmal tumor: a subtle presentation in an African American woman and review of immunohistochemical markers for this rare condition. Cureus 2021; 13 (08) e17289
- 9 Cavanagh G, Negbenebor NA, Robinson-Bostom L, Walker JL. Two cases of malignant proliferating trichilemmal tumor (MPTT) and review of literature. R I Med J (2013) 2022; 105 (01) 12-16
- 10 Abdelhammed MH, Siatecka H, Diwan AH. et al. A rare case of a malignant proliferating trichilemmal tumor: a molecular study harboring potential therapeutic significance and a review of literature. Dermatopathology (Basel) 2024; 11 (04) 354-363
- 11 Sun J, Zhang L, Xiao M. et al. Systematic analysis and case series of the diagnosis and management of trichilemmal carcinoma. Front Oncol 2023; 12: 1078272
- 12 Moran JMT, Hoang MP, Mariño-Enríquez A, DeSimone MS. Malignant proliferating pilar tumor with sarcomatous transformation (“carcinosarcoma”): case report with molecular profile. Am J Dermatopathol 2025; 47 (01) 65-69
- 13 Boeisa AN, Alkhars AM, Albaqshi AA, Al-Arbash MS, Alqatari MA, Mohammad Mousa IA. A proliferating trichilemmal tumor at an uncommon site treated with radical excision: a case report and literature review. Cureus 2024; 16 (07) e64803
- 14 Kemaloğlu CA, Öztürk M, Aydın B, Canöz Ö, Eğilmez O. Malignant proliferating trichilemmal tumor of the scalp: report of 4 cases and a short review of the literature. Case Reports Plast Surg Hand Surg 2022; 9 (01) 158-164
- 15 Islam AFMA, Ahmed MI, Uddin MS, Hamid MA. Outcome of latissimus dorsi free flap in-case of large scalp defect: a single center study. Int Surg J 2021; 8 (12) 3678-3682
- 16 Sutherland D, Roth K, Yu E. Malignant proliferating trichilemmal tumor treated with radical radiotherapy: A case report and literature review. Cureus 2017; 9 (01) e999
- 17 Park BS, Yang SG, Cho KH. Malignant proliferating trichilemmal tumor showing distant metastases. Am J Dermatopathol 1997; 19 (05) 536-539
- 18 Bae SB, Lee KK, Kim JS. et al. A case of malignant proliferating trichilemmoma of the scalp with multiple metastases. Korean J Intern Med (Korean Assoc Intern Med) 2001; 16 (01) 40-43
- 19 Rao S, Ramakrishnan R, Kamakshi D, Chakravarthi S, Sundaram S, Prathiba D. Malignant proliferating trichilemmal tumour presenting early in life: an uncommon feature. J Cutan Aesthet Surg 2011; 4 (01) 51-55
- 20 Fieleke DR, Goldstein GD. Malignant proliferating trichilemmal tumor treated with Mohs surgery: proposed protocol for diagnostic work-up and treatment. Dermatol Surg 2015; 41 (02) 292-294
- 21 Virdi A, Borghol K, Edwards B, Barnard N. Scalp malignant trichilemmal tumour with bony erosion: a new clinical entity. BMJ Case Rep 2021; 14 (05) e239161