

Subscribe to RSS
DOI: 10.1055/s-0045-1814760
Intradural Capillary Hemangioma: Case Report of a Rare Tumor of Cauda Equina
Authors

Abstract
Intradural extramedullary capillary hemangiomas of the cauda equina are very rare. Radiographically, they may mimic other intradural tumors like meningioma or nerve sheath tumors. Here, we present a case of a young woman who presented with low back and left leg radicular pain. Magnetic resonance imaging showed an enhancing lesion in the intradural space at the L4/L5 level. Initially, a diagnosis of meningioma with differential diagnosis of schwannoma was suspected; however, histopathology revealed it to be a capillary hemangioma. Although rare, because of its similar clinico-radiographical features to other common intradural tumors and high risk of intraoperative bleeding, capillary hemangioma should be included in the differential diagnosis when planning surgical excision.
Keywords
benign spinal tumor - capillary hemangioma - intradural extramedullary - cauda equina syndrome - vascular malformationIntroduction
Capillary hemangiomas are common cutaneous or soft tissue lesions usually seen in the pediatric population.[1] In the central and peripheral nervous systems, these tumors are rare but can occasionally arise from the dura or spinal nerve roots, specifically from the vasa nervorum.[1] [2] [3] In the intradural space, only a few cases of capillary hemangiomas are reported in the literature. To date, less than 25 cases of capillary hemangiomas in the cauda equina have been reported.[4] ([Table 1]). Tunthanathip et al proposed a new classification system based on 64 reported cases of capillary hemangioma within the whole spinal axis.[5] We report yet another rare case of intradural capillary hemangioma in the cauda equina (L4 level) in a young woman that was resected en bloc without neurological deficit.
Case Presentation
A 25-year-old woman presented to us with recurrent low back pain and radicular left leg pain for the past 1 year. Pain started in the lower back, radiating down to the foot along the lateral aspect of the thigh and leg, associated with tingling and numbness. Bowel and bladder functions were normal. Previous medical history and family history were unremarkable. On clinical examination, there were no motor or sensory deficits, the deep tendon reflexes were normal, and a straight leg test was negative on both sides. Other biomedical and hematological laboratory tests showed no abnormalities. The patient was initially treated in keeping with lumbar degenerative spondylosis. Magnetic resonance imaging (MRI) of the lumbosacral spine was advised when the patient presented with recurrence of radicular pain, which was progressively worsening over the last 3 months. MRI showed a round, well-defined 13 mm × 9 mm intradural extramedullary mass lesion in the spinal canal at the L4/L5 level ([Fig. 1]). It was isointense on the T1-weighted sequence and slightly hyperintense on the T2-weighted sequence. The lesion enhanced homogeneously on the contrast study. Radiographically, a benign nerve sheath tumor was considered as a primary diagnosis. Capillary hemangioma was not considered in the differential, possibly because it is rare in this location and age group.

The surgery was completed under general anesthesia in the prone position through a posterior midline approach. A complete L4 laminectomy and L5 cranial hemilaminectomy, with midline durotomy, were performed. On gross appearance, the tumor was a highly vascular, reddish, spongy, oval mass, so biopsy was avoided due to the risk of potential bleeding ([Fig. 2]). Following meticulous arachnoid dissection, the cauda equina was separated from the tumor, except for a nerve root that was seen entering the lesion. We used intraoperative neurophysiological monitoring to avoid postoperative neurological deficit. Two nerve fascicles were going toward the tumor, densely adhered to the tumor capsule. Using continuous neuromonitoring, the ventral fascicle was separated from the tumor, but the dorsal fascicle was densely attached to the capsule. We noticed continuous oozing when we tried to separate the fascicle from the capsule; hence, we abandoned the attempt to free the fascicle from the tumor. The nerve fascicle was stimulated. When no signal was recorded, it was resected and the tumor was removed en bloc ([Fig. 3]). The patient had an uncomplicated postoperative course with no neurological deficit. The histopathology report later confirmed the diagnosis of capillary hemangioma.

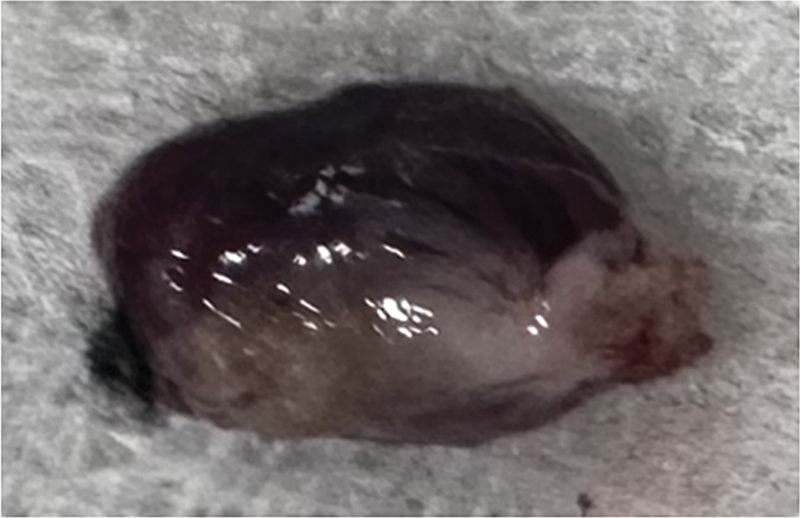
On gross appearance, a reddish brown, multilobular, spongy, oval mass measuring 1.0 × 0.7 cm was identified ([Fig. 3]). Histopathological examination of the specimen revealed proliferation of blood vessels forming aggregates of closely packed thin-walled capillaries, blood-filled and lined by a single layer of endothelial cells ([Figs. 4] and [5]). The perivascular stroma showed mild chronic inflammatory cell infiltrates. The adjacent area showed nerve fascicles and congested blood vessels. Atypical cell/mitosis/dysplasia was not seen. The report was a benign vascular lesion, suggestive of capillary hemangioma.


The patient was followed over a period of 3 months. Her radicular symptoms completely resolved, and she remains asymptomatic.
Discussion
Of all the CNS tumors, 5–12% are located in the spinal cord.[6] Furthermore, vascular tumors represent 2–7% of intraspinal tumors.[7] Within the spine, hemangiomas are usually seen in the vertebral bodies, but they are rarely encountered in the intradural space.[8] Intradural capillary hemangiomas can arise from the inner surface of the dura, the pia, or from the vasculature of the nerve roots.[9] Tunthanathip et al reported 2 cases and reviewed 64 cases of capillary hemangioma (total reported cases) within the spinal axis.[5] But, to date, only 25 cases of Intradural extramedullary capillary hemangiomas of the cauda equina were reported in the literature ([Table 1]). Of these reported cases, epidemiological findings demonstrate that the highest frequency of tumor occurrence is in males between the ages of 40 and 60 years, except for two patients who were 20 and 28 years old.[3] [8] [10] [11] Our particular case is unique due to the patient's gender and age being outside of the classic presentation.
|
Sl. no. |
Author |
Number of cases |
Age (y) |
Gender |
Level |
|---|---|---|---|---|---|
|
1 |
Mastronardi et al[2] |
1 |
41 |
M |
L5 |
|
2 |
Zander et al[19] |
1 |
51 |
F |
L4–L5 |
|
3 |
Holtzman et al[8] |
1 |
56 |
F |
L4–L5 |
|
4 |
Roncaroli et al[20] |
9 |
40–62 |
9/10 (6M, 4F) hemangiomas are of the capillary type |
Not reported |
|
5 |
Ghazi et al[21] |
1 |
42 |
M |
L3–L4 |
|
6 |
Ganapathy et al[22] |
1 |
17 |
M |
L2–L3 |
|
7 |
Miri et al[9] |
1 |
20 |
M |
L3 |
|
8 |
Liu et al[10] |
1 |
53 |
M |
L3–L4 |
|
9 |
Pignotti et al[23] |
1 |
45 |
F |
L1–L2 |
|
10 |
Unnithan et al[24] |
1 |
54 |
F |
L4–L5 |
|
11 |
Fish et al[25] |
1 |
27 |
F |
L4–L5 |
|
12 |
Hughes et al[4] |
1 |
50 |
M |
L4 |
|
13 |
Johnson et al[11] |
1 |
14 |
F |
L2 |
|
14 |
Cai et al[26] |
4 |
25–40 |
2M, 2F |
L2–L4 |
|
15 |
This case, 2025 |
1 |
25 |
F |
L4–L5 |
|
Total |
26 |
Clinical features are secondary to the compressive mass effect on the spinal cord or the nerve root. Patients typically present with low back pain, radiculopathy, myelopathy, or cauda equina syndrome, depending on the location and degree of compression. The most common location for this type of lesion is the thoracic spine (60%), followed by the conus medullaris and lumbar spine at 18% each.[5] Paresthesia and back pain were the most common clinical presentations seen in 57 and 51% cases, respectively.[5] Our patient had a capillary hemangioma in the lumbar spine and presented with low back pain and paresthesia of the left lower limb. Clinically, capillary hemangiomas have a slower onset of symptoms with gradual progression in contrast to cavernous hemangioma (another similar vascular lesion). Capillary hemangiomas have a lower chance of bleeding and hence are less likely to present with acute deterioration of neurological function.[12] In our case, the patient had a 1-year history of low back pain, with radicular left leg pain, gradual onset with progressive pain for 6 months. MRI was advised for recurrent radicular leg pain, which showed an intradural extramedullary mass at L4, suggestive of a meningioma or nerve sheath tumor. Features of capillary hemangioma on MR images are an isointense lesion on T1-weighted images, hyperintense relative to the spinal cord on T2-weighted images, and homogenous, strong enhancement on contrast-enhanced T1-weighted images.[3] Since meningiomas and schwannomas are more common in the thoracolumbar region and their clinico-radiographical features are similar to capillary hemangioma, they could be easily missed or unnoticed. Despite the rarity of hemangiomas in this space, early recognition is important because of the risk of hemorrhage, albeit low, which may produce sudden neurologic deterioration and, more importantly, for surgical planning due to the risk of intraoperative bleeding if attempting piecemeal excision. In our case, the possibility of capillary hemangioma was not mentioned on imaging; rather, the diagnosis of capillary hemangioma was made after histological examination. Spinal angiography is a useful investigation to differentiate nonvascular tumors from vascular tumors, and thus can reduce the risk of intraoperative bleeding if preoperative embolization is considered. Abdullah et al reported a similar case with MR features of enlarged perimedullary veins indicating a vascular tumor and suggested preoperative spinal angiography.[13] Angiography was not done in our case.
Complete surgical resection is the treatment of choice for intradural extramedullary hemangioma.[7] [14] Because of the excessive vascularity of a capillary hemangioma, cutting into it should be avoided, as bleeding resulting in incomplete resection might occur; however, the extent of resection will be determined by the degree of nerve root involvement.[15] Intraoperative neuromonitoring is a very useful adjunct if available to avoid postoperative neurological deficit. We did an en bloc excision along with the nerve fiber attached to it. We used intraoperative monitoring in our case, which made us feel more confident to remove the tumor without any deterioration in neurology after surgery. After total resection, tumor recurrence has rarely been reported.[16] Abe et al reported no recurrence at 13 years after complete resection.[17] If partial resection is performed, regular follow-up is important to monitor for recurrence. Selective spinal angiography has shown to be sufficient to demonstrate the tumor's intense vascularity and feeding vessel(s), but only one case has been reported by Tunthanathip et al in which embolization was done before surgery.[5]
Based on case series of 64 patients, Tunthanathip et al propose a classification scheme for the spinal capillary hemangiomas comprising the following five types: pediatric type found in 5%; epidural type, found in 8%; intradural extramedullary type, found in 70%, which is the most common type of spinal capillary hemangioma; intramedullary type, found in 14%; and hemangiomatosis, found in 3%.[5] In our case, it was intradural extramedullary in location.
Capillary and cavernous hemangiomas arise from the same cell type. They can be differentiated on histopathology. Cavernous hemangiomas consist of diffusely arranged large dilated vascular channels, whereas the unique characteristic of capillary hemangioma is a capsulated nodular lesion composed of capillary-sized vascular channels, which are tightly packed into nodules separated by fibrous septa, and each of which is nourished by a single feeding vessel.[1] [18] Although rare and benign in nature, because of the high risk of intraoperative bleeding and incomplete excision, capillary hemangiomas should be considered in the differential diagnosis before surgical planning. En bloc resection should be a goal of surgery to prevent recurrence. Preoperative angiography and intraoperative neurophysiological monitoring should be considered (if available) to achieve this goal.
Conclusion
We report a rare case of an intradural capillary hemangioma of the cauda equina in a young woman, which was resected en bloc without perioperative complications. Despite the rarity of hemangiomas in this space, this should be considered in the differential diagnosis as early recognition is important because of the risk of hemorrhage.
Conflict of Interest
None declared.
-
References
- 1 Roncaroli F, Scheithauer BW, Krauss WE. Capillary hemangioma of the spinal cord. Report of four cases. J Neurosurg 2000; 93 (01) , suppl): 148-151
- 2 Mastronardi L, Guiducci A, Frondizi D, Carletti S, Spera C, Maira G. Intraneural capillary hemangioma of the cauda equina. Eur Spine J 1997; 6 (04) 278-280
- 3 Choi BY, Chang KH, Choe G. et al. Spinal intradural extramedullary capillary hemangioma: MR imaging findings. AJNR Am J Neuroradiol 2001; 22 (04) 799-802
- 4 Hughes LP, Largoza G, Montenegro TS. et al. Intradural extramedullary capillary hemangioma of the cauda equina: case report of a rare spinal tumor. Spinal Cord Ser Cases 2021; 7 (01) 21
- 5 Tunthanathip T, Rattanalert S, Oearsakul T, Kanjanapradit K. Spinal capillary hemangiomas: two cases reports and review of the literature. Asian J Neurosurg 2017; 12 (03) 556-562
- 6 Salari N, Ghasemi H, Fatahian R. et al. The global prevalence of primary central nervous system tumors: a systematic review and meta-analysis. Eur J Med Res 2023; 28 (01) 39
- 7 Nowak DA, Widenka DC. Spinal intradural capillary haemangioma: a review. Eur Spine J 2001; 10 (06) 464-472
- 8 Holtzman RN, Brisson PM, Pearl RE, Gruber ML. Lobular capillary hemangioma of the cauda equina. Case report. J Neurosurg 1999; 90 (02) , suppl): 239-241
- 9 Miri SM, Habibi Z, Hashemi M, Meybodi AT, Tabatabai SA. Capillary hemangioma of cauda equina: a case report. Cases J 2009; 2 (01) 80
- 10 Liu JJ, Lee DJ, Jin LW, Kim KD. Intradural extramedullary capillary hemangioma of the cauda equina: case report and literature review. Surg Neurol Int 2015; 6 (Suppl. 03) S127 –S131
- 11 Johnson WC, Espinosa J, Tavakoli S. et al. A case report of lobular intradural extramedullary capillary hemangioma in a 14-year-old patient: resection and reconstruction. J Spine Surg 2024; 10 (01) 152-158
- 12 Bruni P, Massari A, Greco R, Hernandez R, Oddi G, Chiappetta F. Subarachnoid hemorrhage from cavernous angioma of the cauda equina: case report. Surg Neurol 1994; 41 (03) 226-229
- 13 Abdullah DC, Raghuram K, Phillips CD, Jane Jr JA, Miller B. Thoracic intradural extramedullary capillary hemangioma. AJNR Am J Neuroradiol 2004; 25 (07) 1294-1296
- 14 Alakandy LM, Hercules S, Balamurali G, Reid H, Herwadkar A, Holland JP. Thoracic intradural extramedullary capillary haemangioma. Br J Neurosurg 2006; 20 (04) 235-238
- 15 Shin JH, Lee HK, Jeon SR, Park SH. Spinal intradural capillary hemangioma: MR findings. AJNR Am J Neuroradiol 2000; 21 (05) 954-956
- 16 Kaneko Y, Yamabe K, Abe M. Rapid regrowth of a capillary hemangioma of the thoracic spinal cord. Neurol Med Chir (Tokyo) 2012; 52 (09) 665-669
- 17 Abe M, Tabuchi K, Tanaka S. et al. Capillary hemangioma of the central nervous system. J Neurosurg 2004; 101 (01) 73-81
- 18 Enzinger FM, Weiss SH. . ( 1995. ) Benign tumors and tumor-like lesions of blood vessels. In: Enzinger FM, Weiss SH (eds) Soft tissue tumors, 3rd edn. Mosby, St. Louis, pp 581–586
- 19 Zander DR, Lander P, Just N, Albrecht S, Mohr G. Magnetic resonance imaging features of a nerve root capillary hemangioma of the spinal cord: case report. Can Assoc Radiol J 1998; 49 (06) 398-400
- 20 Roncaroli F, Scheithauer BW, Krauss WE. Hemangioma of spinal nerve root. J Neurosurg 1999; 91 (02) , suppl): 175-180
- 21 Ghazi NG, Jane JA, Lopes MB, Newman SA. Capillary hemangioma of the cauda equina presenting with radiculopathy and papilledema. J Neuroophthalmol 2006; 26 (02) 98-102
- 22 Ganapathy S, Kleiner LI, Mirkin LD, Hall L. Intradural capillary hemangioma of the cauda equina. Pediatr Radiol 2008; 38 (11) 1235-1238
- 23 Pignotti F, Coli A, Fernandez E, Montano N. Capillary hemangioma of the cauda equina. Surg Neurol Int 2015; 6: 133
- 24 Unnithan AK, Joseph TP, Gautam A, Shymole V. Case report of lumbar intradural capillary hemangioma. Surg Neurol Int 2016; 7 (Suppl. 05) S139 –S141
- 25 Fish C, Sy J, Wong J. High mitotic activity in a capillary hemangioma of the cauda equina: case report and review of the literature. Clin Neuropathol 2020; 39 (03) 135-138
- 26 Cai Z, Hong X, Zhang Z, Ding X, Sun W, Hu G. Microsurgical treatment of spinal intradural capillary hemangioma: a consecutive case series of 18 patients and literature review. Clin Neurol Neurosurg 2024; 246: 108527
Address for correspondence
Publication History
Article published online:
22 January 2026
© 2026. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Roncaroli F, Scheithauer BW, Krauss WE. Capillary hemangioma of the spinal cord. Report of four cases. J Neurosurg 2000; 93 (01) , suppl): 148-151
- 2 Mastronardi L, Guiducci A, Frondizi D, Carletti S, Spera C, Maira G. Intraneural capillary hemangioma of the cauda equina. Eur Spine J 1997; 6 (04) 278-280
- 3 Choi BY, Chang KH, Choe G. et al. Spinal intradural extramedullary capillary hemangioma: MR imaging findings. AJNR Am J Neuroradiol 2001; 22 (04) 799-802
- 4 Hughes LP, Largoza G, Montenegro TS. et al. Intradural extramedullary capillary hemangioma of the cauda equina: case report of a rare spinal tumor. Spinal Cord Ser Cases 2021; 7 (01) 21
- 5 Tunthanathip T, Rattanalert S, Oearsakul T, Kanjanapradit K. Spinal capillary hemangiomas: two cases reports and review of the literature. Asian J Neurosurg 2017; 12 (03) 556-562
- 6 Salari N, Ghasemi H, Fatahian R. et al. The global prevalence of primary central nervous system tumors: a systematic review and meta-analysis. Eur J Med Res 2023; 28 (01) 39
- 7 Nowak DA, Widenka DC. Spinal intradural capillary haemangioma: a review. Eur Spine J 2001; 10 (06) 464-472
- 8 Holtzman RN, Brisson PM, Pearl RE, Gruber ML. Lobular capillary hemangioma of the cauda equina. Case report. J Neurosurg 1999; 90 (02) , suppl): 239-241
- 9 Miri SM, Habibi Z, Hashemi M, Meybodi AT, Tabatabai SA. Capillary hemangioma of cauda equina: a case report. Cases J 2009; 2 (01) 80
- 10 Liu JJ, Lee DJ, Jin LW, Kim KD. Intradural extramedullary capillary hemangioma of the cauda equina: case report and literature review. Surg Neurol Int 2015; 6 (Suppl. 03) S127 –S131
- 11 Johnson WC, Espinosa J, Tavakoli S. et al. A case report of lobular intradural extramedullary capillary hemangioma in a 14-year-old patient: resection and reconstruction. J Spine Surg 2024; 10 (01) 152-158
- 12 Bruni P, Massari A, Greco R, Hernandez R, Oddi G, Chiappetta F. Subarachnoid hemorrhage from cavernous angioma of the cauda equina: case report. Surg Neurol 1994; 41 (03) 226-229
- 13 Abdullah DC, Raghuram K, Phillips CD, Jane Jr JA, Miller B. Thoracic intradural extramedullary capillary hemangioma. AJNR Am J Neuroradiol 2004; 25 (07) 1294-1296
- 14 Alakandy LM, Hercules S, Balamurali G, Reid H, Herwadkar A, Holland JP. Thoracic intradural extramedullary capillary haemangioma. Br J Neurosurg 2006; 20 (04) 235-238
- 15 Shin JH, Lee HK, Jeon SR, Park SH. Spinal intradural capillary hemangioma: MR findings. AJNR Am J Neuroradiol 2000; 21 (05) 954-956
- 16 Kaneko Y, Yamabe K, Abe M. Rapid regrowth of a capillary hemangioma of the thoracic spinal cord. Neurol Med Chir (Tokyo) 2012; 52 (09) 665-669
- 17 Abe M, Tabuchi K, Tanaka S. et al. Capillary hemangioma of the central nervous system. J Neurosurg 2004; 101 (01) 73-81
- 18 Enzinger FM, Weiss SH. . ( 1995. ) Benign tumors and tumor-like lesions of blood vessels. In: Enzinger FM, Weiss SH (eds) Soft tissue tumors, 3rd edn. Mosby, St. Louis, pp 581–586
- 19 Zander DR, Lander P, Just N, Albrecht S, Mohr G. Magnetic resonance imaging features of a nerve root capillary hemangioma of the spinal cord: case report. Can Assoc Radiol J 1998; 49 (06) 398-400
- 20 Roncaroli F, Scheithauer BW, Krauss WE. Hemangioma of spinal nerve root. J Neurosurg 1999; 91 (02) , suppl): 175-180
- 21 Ghazi NG, Jane JA, Lopes MB, Newman SA. Capillary hemangioma of the cauda equina presenting with radiculopathy and papilledema. J Neuroophthalmol 2006; 26 (02) 98-102
- 22 Ganapathy S, Kleiner LI, Mirkin LD, Hall L. Intradural capillary hemangioma of the cauda equina. Pediatr Radiol 2008; 38 (11) 1235-1238
- 23 Pignotti F, Coli A, Fernandez E, Montano N. Capillary hemangioma of the cauda equina. Surg Neurol Int 2015; 6: 133
- 24 Unnithan AK, Joseph TP, Gautam A, Shymole V. Case report of lumbar intradural capillary hemangioma. Surg Neurol Int 2016; 7 (Suppl. 05) S139 –S141
- 25 Fish C, Sy J, Wong J. High mitotic activity in a capillary hemangioma of the cauda equina: case report and review of the literature. Clin Neuropathol 2020; 39 (03) 135-138
- 26 Cai Z, Hong X, Zhang Z, Ding X, Sun W, Hu G. Microsurgical treatment of spinal intradural capillary hemangioma: a consecutive case series of 18 patients and literature review. Clin Neurol Neurosurg 2024; 246: 108527