

Subscribe to RSS
DOI: 10.1055/s-0045-1814425
Imaging and Endovascular Management of Complications of Dialysis Arteriovenous Fistula
Authors
Funding None.


Abstract
Patients with end-stage renal disease depend on maintenance hemodialysis when a renal transplant is not an option. However, the increasing number of patients undergoing dialysis through arteriovenous fistulas (AVFs) has brought about a noticeable increase in fistula-related complications. AVFs are prone to a lack of maturation, anastomotic stenosis, thrombosis, venous pseudoaneurysms, and central vein obstruction. These complications can be effectively addressed with various endovascular techniques, such as balloon angioplasty, stenting, embolization of early-draining collaterals, thrombolysis, and central vein recanalization, all aimed at extending the lifespan of vascular access sites. It is essential for endovascular interventionalists to be highly knowledgeable in the types of AVFs, their potential complications, and the available endovascular options. This article aims to review the different AVF types, their complications, clinical presentations, ultrasound imaging, and endovascular treatment options, providing a comprehensive guide for clinicians involved in the care of patients with AVFs.
Keywords
central venous stenosis - thrombolysis - venoplasty - cutting balloons - high-pressure balloonsIntroduction
End-stage renal disease (ESRD) accounts for ∼3% of premature adult deaths.[1] The incidence of ESRD is on the rise, with ∼232 out of every million patients requiring renal replacement therapy (RRT) each year.[2] [3] [4] Although renal transplantation is the definitive treatment, limitations of donor availability and high economic cost preclude this option for many. Hemodialysis, through an arteriovenous fistula (AVF), is the most common RRT. The creation and maintenance of vascular access (VA) pose significant challenges. AVFs are prone to complications such as lack of maturation, anastomotic and juxta-anastomotic stenosis, thrombosis, venous pseudoaneurysms, and outflow and central vein obstruction. Patients undergo active surveillance to detect AVF failure and complications early. Physical examination and duplex ultrasound are mainstays in identifying early-failing fistulas.[5] [6] Endovascular techniques such as balloon angioplasty, stenting, embolization of early-draining collaterals, thrombolysis, and central vein revascularization can treat these complications and prolong the lifespan of VA sites. Interventional radiologists must be aware of the problems specific to each type of fistulae and the endovascular treatment options. This article discusses various types of AVFs, their complications, clinical presentations, imaging findings, and endovascular treatment options.
Anatomy of Arteriovenous Fistula
Native AVFs are created surgically by connecting an artery with a vein. In an arteriovenous graft (AVG), a prosthetic conduit connects an artery to a vein. This is considered in cases where a suitable caliber vein is unavailable for fistula creation. One advantage of AVG is that it can be used immediately after creation, unlike an AVF, which requires fistula maturation before use for hemodialysis. Given their longer patency rates and lower infection rates, native AVFs are preferred over graft AVFs. Radiocephalic, brachiocephalic, and brachial transposed basilic vein fistulas (BTBs) are usually created in the nondominant upper limb ([Fig. 1]).[5] [6] A lower limb fistula has a higher rate of infection and thrombosis, and is considered if upper limb options are exhausted. Radiocephalic fistula (RCF) is preferred because it is easy to create, allows the placement of a future proximal brachiocephalic fistula (BCF), and has a low incidence of arterial steal and ischemic monomelic neuropathy.[7] However, its drawbacks are its low maturation and flow rates.[8] [9] BCF may be performed first in cases with multiple comorbidities due to its higher maturity and patency.[10] Though easy to create and has a faster maturation time, BCF has a higher rate of arterial steal and symptomatic central venous stenosis.[11] [12] In a BTB, the basilic vein is transposed to the subcutaneous plane in a single- or two-stage procedure.[13] [14] [15] A two-stage procedure is used in small basilic veins but delays hemodialysis by 4 to 8 weeks.

A matured functional hemodialysis fistula includes a fistula vein that is readily visible and a palpable thrill at the arteriovenous anastomosis that gradually diminishes along the course of the outflow vein. Pulsatility in the fistula vein, with no thrill, indicates a notable stenosis downstream, potentially accompanied by a thrill at the stenosis and a diminished thrill or venous collapse beyond it. Auscultation can be helpful in diagnosing central lesions, especially those located in the axillary area, where the vein is at a more profound level and cannot be palpated.[16] [17] Examining the peripheral arterial status of the hemodialysis access arm is essential: the brachial-digital index can predict the development of access-induced ischemic steal syndrome. A poor preprocedural peripheral pulse should discourage interventionalists from intervening aggressively on lesions of the main outflow vein, particularly if located near the arteriovenous anastomosis.[18]
Clinical Presentation
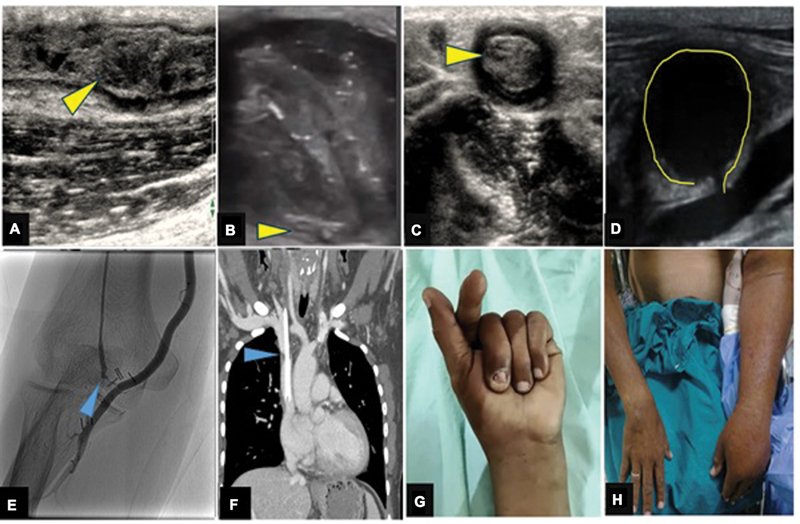
The clinical presentations are varied and depend on the stage of the fistula ([Table 1], [Fig. 2]).
-
Nonmaturation of fistula: It occurs if the arterial and venous diameters are inadequate (< 2 mm) or due to infection or stenosis at the anastomotic site. Maturation may take longer if veins are small-caliber or if an early-draining vein prevents arterialization. They also occur in people with diabetes and those with severe atherosclerotic arterial inflow narrowing.
-
Matured AVF failure due to stenosis or thrombosis: A mature fistula may fail and patients present with prolonged dialysis time (> 4 hours) and reduced thrill. An AVF may fail due to stenosis at the venous side, anastomotic site, or, rarely, due to arterial stenosis proximal to the fistula. Venous stenosis results from intimal hyperplasia, which can be due to surgical trauma at access creation, inflammation, uremia, hypoxia, hemodynamic shear stress, and vessel wall injury from needle punctures. Cellular mechanisms include leukocyte proliferation and smooth muscle cell migration from the media into the intimal layer, leading to venous stenosis.[19] A mature fistula may have reduced flow due to partial thrombosis of venous outflow. These patients must be identified early and treated since they are prone to acute fistula thrombosis. Other causes of acute fistula thrombosis include acute hypotension, venous stenosis with downstream occlusion, venous aneurysm, or infection.
-
Venous hypertension-induced limb edema: Approximately 10% of dialysis AVF patients and 13% of tunneled central venous catheter (CVC) patients have central venous stenosis.[18] [19] [20] Prior use of central line catheter predisposes these patients to thrombosis or central vein narrowing. High-output cardiac failure, which presents similarly, should be differentiated from central venous stenosis. Cardiac failure presents as generalized edema compared with focal edema in venous hypertension.[21]
-
Limb claudication and ulceration: The arterial steal phenomenon can cause ischemic pain, gangrenous changes, or altered distal limb sensations. The larger diameters of proximal vessels make arterial steal more common in BCF than in RCF. Ischemic distal atherosclerotic disease can mimic steal. Improvement of symptoms upon fistula compression suggests true steal.[18] Uremic mononeuritis can also mimic digital ischemic symptoms. They, however, present primarily with numbness, and the Doppler examination shows good flow in the radial and ulnar vessels. Other presentations include swelling at the fistula site from seroma, abscess, hematoma, or pseudoaneurysm.
Abbreviations: AVF, arteriovenous fistula; USG, ultrasonography.
Imaging in a Dysfunctional Fistula
Prior to creating an AVF, it is highly recommended to obtain duplex ultrasound to ensure the artery diameter is more than 2 mm, the vein diameter is more than 2.5 mm, the depth from the skin is less than 5 mm, there are no early-draining veins, and there is no central vein obstruction. The absence or reduced transmitted venous pulsations from the heart is an indirect marker of central venous stenosis. While thrill and flow rate during dialysis are used to determine fistula maturity, ultrasound surveillance is increasingly important in detecting early malfunction. To ensure an adequate fistula, the ultrasound criteria can be summarized as the “rule of 6”—an access vein diameter more than 6 mm, a flow rate more than 600 mL/min, and a skin distance less than 6 mm ([Table 2]).[22] [23] A flow rate of less than 300 to 500 mL/min, fistula circuit narrowing, elevated peak systolic velocity (PSV) at the stenotic site (>375 cm/s), and PSV ratio (>2:1) between the suspicious segment and the vein 2 cm caudal to it suggest hemodynamically significant venous stenosis. Loss of jugular vein phasic variation can indicate central venous stenosis on ultrasound. This phasic variation may be more evident if AVF is compressed. Utilizing a suprasternal acoustic window with a steep angulation and a transducer with a small footprint can visualize the brachiocephalic veins to some extent. Thrombosis is characterized by low-level intraluminal echoes with no demonstrable flow on color flow imaging or spectral Doppler. High-flow fistulas causing high-output cardiac failure and have flow rates of 1,500 to 2,000 mL/min. Patients with central venous stenosis require vessel angioplasty or stenting, while those with high-output fistula need fistula reduction or closure.[24] [25]
Abbreviations: ECG, electrocardiogram; ESRD, end-stage renal disease.
Computed tomography (CT) or magnetic resonance (MR) venography offers a better assessment of the central veins. CT can determine the site and extent of occlusion, the distal stump, and the status of the contralateral brachiocephalic and subclavian veins. Dialysis after a CT scan can prevent contrast-induced osmotic fluid overload. Due to the risk of nephrogenic systemic fibrosis with gadolinium-contrast material, noncontrast MR venography techniques are recommended to evaluate central venous stenosis. Catheter angiography can demonstrate steal syndrome, distal arterial disease, and distal vasculature anatomy for surgical reconstruction.
Pre- and Intraprocedural Care during Endovascular Therapies
As patients with ESRD undergo hemodynamic and physiological changes, it is crucial to take all the necessary precautions during endovascular interventions ([Table 2]). To avoid volume overload and pulmonary edema, intravenous fluids must be used with utmost care. The daily fluid requirement can be easily calculated by adding the 24-hour urine output volume and 500 mL for basic metabolism/sweating. Distinguishing dyspnea caused by pulmonary edema from compensatory nonlabored hyperventilation due to metabolic acidosis is important. Only high-ceiling loop diuretics, such as furosemide, can effectively reduce pulmonary edema and preload by shifting fluid to the peripheral venous compartment, as the kidney has minimal to no diuretic function. The use of hyperosmolar contrast materials can lead to fluid overload. Hence, iso-osmolar contrast materials are preferred to prevent volume overload. Platelet dysfunction caused by elevated blood levels of uremic toxins requires careful use of antiplatelets such as aspirin, as they may increase bleeding. A more conservative loading dose of 60 units/kg and a maintenance dose of 12 units/kg/h of unfractionated heparin are preferred due to the prolonged half-life of heparin in chronic kidney disease.[26] Direct oral anticoagulants with renal excretion should also be avoided. Single antiplatelet, preferably clopidogrel 75 mg, is recommended by the European Society of Vascular Surgery 2023 guidelines as an antithrombotic regimen after venoplasty or stent placement.[27]
Endovascular Management
Nonmaturing Fistula
The treatment focuses on addressing the underlying cause of nonmaturation. Balloon angioplasty of the feeding artery or anastomotic stenosis can improve the arterial inflow. The balloon-assisted maturation of the fistula is possible when the parent vein is of a small caliber, specifically less than 2 mm ([Fig. 3]). Multiple sessions of balloon-assisted maturation may be required. Cui et al have developed a technique of ultrasonography-guided minimally invasive suture ligation of the early-draining vein (interrupting rivaling access flow with nonsurgical image-guided ligation), in which a surgical suture is advanced through a needle tunneled beneath the collateral vein under ultrasound guidance.[28] [29] Surgical ligation or endovascular coiling can treat any early-draining vein ([Fig. 3]).[21]
Venous Stenosis
A venous stenosis can occur just beyond the arteriovenous anastomosis, in the cephalic arch, or central veins. Juxta-anastomotic stenosis may be related to repeated same-site cannulation and neointimal hyperplasia. They respond to balloon angioplasty. Recurrent or resistant stenoses can be treated using high-pressure balloons (e.g., Conquest, Atlas balloon catheters, Bard Peripheral, Tempe, Arizona, United States), or cutting balloons. The balloon profile should be based on the native caliber of the treated vein in a non-post-stenotic dilation area and increased by 20%. The sizing of the cutting balloon differs from that of conventional balloons. It should match the expected native caliber of the vein at a 1:1 to 1.1:1 ratio, as oversizing increases the risk of venous rupture. The manufacturer advises against using the cutting balloon in tortuous venous segments due to the same problem. To achieve symmetrical intimal damage, the catheter shaft may be rotated between inflations. Unfortunately, the cutting balloon is unavailable in >8 mm diameter, rendering it ineffectual for resistant central venous lesions.[30] [31] Drug-coated balloon (DCB) angioplasty is the latest addition to the armamentarium to treat recurrent venous stenosis. Lookstein et al reported that the 6-month primary patency was superior with a DCB than standard balloon (82.2% [125 of 152] vs. 59.5% [88 of 148], p < 0.001).[32] The length of DCB used should be slightly longer than the balloon used for lesion preparation and should exceed the stenotic lesion by 5 mm on either side of the stenosis to ensure that the entire lesion is covered. It is recommended to predilate a stenotic lesion with a high-pressure or cutting balloon as lesion preparation and an adequate DCB inflation duration of at least 2 minutes to increase the drug deposition to the vessel wall. Abbreviated transit time (time from insertion through the sheath to balloon inflation across the stenosis), ideally less than 30 seconds, to reduce the drug loss in the blood is an essential practice to maximize the efficacy of DCBs.[33] [34] Complete intravascular or extravascular ultrasound-guided venoplasty has been attempted with good results to obviate the radiation and contrast material use.[35] [36]
Cephalic arch stenosis occurs at the cephalic-axillary vein junction due to extrinsic compression by deltopectoral and clavipectoral fascia and increased angulation of the cephalic arch segment. This is best treated with cephalic arch transposition after fascial division. Venoplasty and stenting as endovascular options may be attempted initially. Self-expanding bare-metal stents have a lower patency (6-month patency rate of 42%) than stent grafts (primary-assisted patency of 95% at 6 months).[37] Cephalic vein interventions for dysfunctional fistulas are shown in [Fig. 4]. The various types of VAs possible for fistula interventions are shown in [Fig. 5].


Central Venous Stenosis
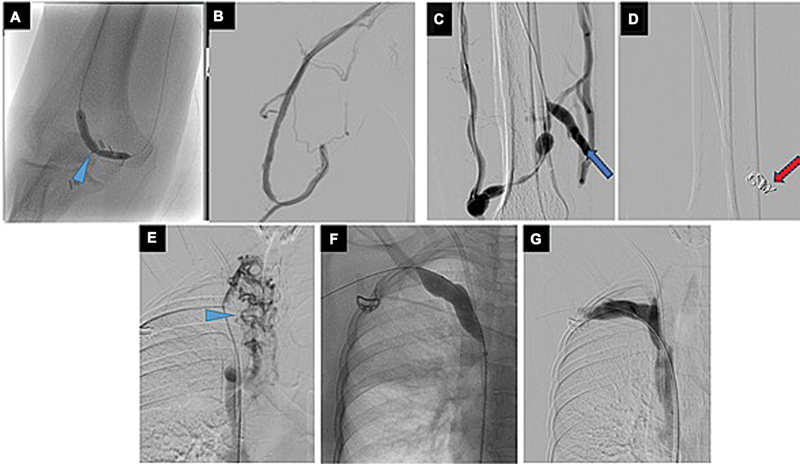
Central venous stenoses are usually induced by prior hemodialysis catheters. The presence of occult central venous lesions in a patient with prior central venous access has been estimated to be as high as 50%.[25] If the presence or hemodynamic significance of a lesion is in doubt, pullback pressure measurement is the gold standard evaluation tool, with gradients greater than 5 to 10 mm Hg considered significant. Rich collateral vessels peripheral to venous stenosis, as well as reflux of contrast material into the internal jugular vein in the presence of a stenosis central to its inflow level, is a telltale sign of hemodynamic significance.[28] [29] [37] The Society of Interventional Radiology reporting standards for thoracic central vein obstruction (TCVO) provides a well-structured classification of four anatomical patterns of obstruction that allow clinicians to describe in a reproducible and unambiguous manner ([Fig. 6]). The reporting standards help organize a patient's clinical characteristics in a clear and reproducible way. For central venous occlusions, recanalization is usually achievable using a stiff hydrophilic guidewire and angled catheter, followed by balloon angioplasty. The “snow-plough technique,” in which a Rosen wire is barely advanced to lead a trailing Teflon catheter, is another useful way to cross persistent venous occlusions. This approach also increases forward vector force, and using either or both will usually cross a chronic venous blockage. After crossing the lesion with the catheter, the wire can be exchanged for an Amplatz wire (Cook). Serial balloon angioplasty, especially with high-pressure balloons, can be performed, starting with smaller balloon sizes and ending with diameter 10 to 20% larger than the treated vein(s) ([Fig. 7]). VA can also be obtained via the internal/external jugular veins or suitable collaterals for central venous recanalization.


Sharp recanalization is only contemplated in cases of unsuccessful catheter/guidewire attempts to traverse chronic venous occlusions. The sharp devices that can be used for recanalization are the back end of a guidewire, the directional sheath needles from transjugular intrahepatic portosystemic shunt kits (Haskal and Rösch-Uchida sets, Cook Medical), and the Colapinto needle (Cook Medical). Another described method is to inflate an angioplasty balloon adjacent to the occlusion site. This allows for improved stability, pushability, and centering of the guidewire lumen to the long axis of the occluded vein segment. The back end of the guidewire can then be passed through the balloon wire lumen, centered through the lesion. Also, advancing a guiding catheter or long sheath up to the occlusion (“mother–child technique”) may provide the added support needed to cross the occlusion.[38] [39] [40]
The Power Wire device (Baylis Medical Company, Inc., Montreal, Quebec, Canada) is another newer endovascular alternative that facilitates crossing difficult TCVOs. When using this device, central venography is performed by simultaneous injections through brachial/basilic/jugular and femoral approaches. A semicurved diagnostic catheter with a straight Power Wire tip offers improved precision as the wire gently advances toward a snare, introduced through a 5-F diagnostic catheter through the opposite venous stump. Before the tip of the device is activated by the generator and advanced, its alignment with the snare must be checked in 30 degrees right/left anterior oblique and posteroanterior views. After crossing the occlusion, the radiofrequency wire is snared out and exchanged for a 260-cm stiff 0.035-inch wire.[41] Recent advances in the creation of alternative routes for hemodialysis in patients with chronically occluded thoracic central veins include the Surfacer Inside-Out Access Catheter System (Bluegrass Vascular Technologies, San Antonio, Texas, United States) and upper extremity Hemodialysis Reliable Outflow (HeRO) graft (Hemosphere, a CryoLife Inc Company, Eden Prairie, Minnesota, United States). Surfacer Inside-Out Access Catheter System uses a delivery system that directs a needle wire through an occluded superior vena cava or brachiocephalic veins via a 12-F femoral access sheath ([Fig. 8]). This is followed by placing an exchange wire across the needle over which a tunneled dialysis catheter or a HeRO graft can be placed. The sharp recanalization is navigated with the help of a radio-opaque exit target placed above the sternal end of the clavicle, through which the Surfacer device is advanced under fluoroscopic guidance with appropriate angulation of the image intensifier. The aim is to create a safe intrathoracic tract (vascular or extravascular) through which a tunneled catheter is placed with its tip ending in the mid-right atrium. HeRO graft is a modular system having an e-PTFE (polytetrafluoroethylene) graft component, which is surgically end-to-side anastomosed to the brachial artery with the other end connected to a venous outflow component with its tip in the right atrium. Surfacer device helps the placement of the venous outflow component in patients with chronically occluded central veins.[42] [43] [44] [45]

Stent Placement
Stents placed at the hemodialysis access do not provide better unassisted patency rates than angioplasty alone. They are only used for stenoses unresponsive to venoplasty or recur within 3 months of primary balloon angioplasty. The median primary and secondary patency rates at 1-year follow-up were 19 and 64%. Placing bare stents over the glenohumeral junction increases the risk of stent damage and thrombosis. Balloon-expandable stents should not be used in the costoclavicular space (bounded by the clavicle, first rib, subclavius muscle tendon, and costoclavicular ligament), as the extrinsic compression can cause irreversible deformity or fracture of the stent and vein occlusion.[46] [47] [48] Covered stent grafts have been proposed as an endovascular option for recalcitrant cases of hemodialysis-related central venous occlusive disease and in in-stent restenosis. Anaya-Ayala et al reported a 12-month primary patency of 56%, primary assisted patency of 86%, and secondary patency of 100% using covered stents to treat recurrent central vein obstruction.[49] [50] In 2016, Falk et al[51] reported results of the RESCUE trial in which there was a greater patency after stent graft with 66 and 16% (6- and 12-month patency, respectively) with the device, and only 12 and 2.2% at 6- and 12-month patency for venoplasty.[52] [53] The placement of a covered stent offers a safety net for aggressive recanalization techniques and the use of high-pressure balloons to prevent life-threatening venous extravasation. Stent grafts provided superior 6-month patency rates than angioplasty (64.6 vs. 36.1%) in patients with stenosed/thrombosed hemodialysis grafts.[39] Stent grafts have a newfound role in the management of hemodialysis access with pseudoaneurysms and recurrent stenoses, especially in the basilic vein angle.[54] [55] [56] Braided nitinol stent (Supera, Abbot Vascular, Santa Clara, California, United States) with superior kink resistance and fracture resistance has shown promising results in the treatment of juxta-anastomotic stenosis with primary patency rates of 68.2, 53.3, and 46.2% at 12, 24, and 36 months, respectively.[57] A combined interventional approach of braided stent and DCB was studied by Tang et al in the treatment of cephalic arch stenosis; however, the results were subpar with primary patency of 55 and 31% at 6 and 12 months, respectively. The development of an intense inflammatory reaction within the stent was attributed to the reduced patency rates.[58]
Acute Thrombosis
Acute thrombosis is usually associated with underlying venous stenosis in ∼85 to 90% of cases. If the thrombus is acute (<2 weeks), thrombolysis can remove much of the thrombus. However, as the age of the thrombus increases, a mechanical device may be needed in addition to the pharmacotherapy. Treatment of thrombosis, preferably within 48 hours before the subsequent dialysis session is ideal. Early declotting eliminates the need for a CVC and permits immediate access use. Success rates for surgical thrombectomy ranges from 28 to 73%. A second option is percutaneous mechanical or/and pharmacomechanical thrombectomy. For best outcomes, the fistula outflow vein may need to be cannulated twice, in opposite orientations, toward the venous outflow and arterial inflow. A thrombolytic drug such as Atleplase (4 mg, divided into two doses with 2 mg injected through each VA sheath) may be given locally before mechanical intervention. Limited mechanical declotting performed initially increases the clot surface area and increases the efficiency of thrombolytic therapy that will be administered subsequently. Operator preference and familiarity may determine which mechanical declotting device is used (e.g., Angiojet, Possi, Minneapolis, Minnesota, United Stateas; Hydrolyzer, Cordis, Warren, New Jersey, United States; Cleaner XT Rotational Thrombectomy System, Argon Medical Devices, Plano, Texas, United States; Penumbra computer-assisted thrombectomy, Penumbra Inc, Alameda, California, United States). Thromboaspiration with a 7- or 8-F angled aspiration catheter can also be considered for fistula declotting. Declotting passes should always be done toward the venous outflow and never the arterial inflow to prevent arterial thromboembolism.[59] [60] Underlying stenotic lesions will become unmasked after declotting and should be treated with angioplasty. Failure of thrombolysis occurs in long-segment thrombus, large thrombus load, chronic thrombus, venous pouches with thrombus, and pseudoaneurysm with thrombus. Coagulopathy, fistula site infections, and intracardiac right to left shunt are absolute contraindications for thrombolysis.[61] [62] [63] [64] [65]
Distal Hypoperfusion Ischemic Syndrome (DHIS)
Distal hypoperfusion ischemic syndrome (DHIS) may be due to true steal caused by the shunting of blood into low-pressure outflow veins, causing ischemia distal to the anastomotic site. This can be due to arterial stenosis (above or below the anastomotic site), failure of vascular adaptation, or due to collateral development in the forearm preventing compensation for increased flow into the fistula.[1] Angiogram can confirm true steal syndrome from arterial disease. It also delineates the anatomy distal to the fistula for planning surgical correction. Tordoir et al included the assessment of fistula flow rate to plan additional management ([Table 3]). Arterial stenotic lesions causing steal can be treated with balloon angioplasty. However, surgery is indicated in true steal syndrome. The surgical procedures include banding/ligation of the outflow vein, distal revascularization with interval ligation, and revision using distal inflow ([Figs. 9] and [10]).[64] Endovascular techniques such as partially covering an anastomotic site with a stent graft have also been tried with limited success.[65] [66]


Pseudoaneurysm
Pseudoaneurysms occur commonly secondary to venous stenosis with increased pressures or at the access site due to loss of vessel wall integrity. They can be managed conservatively if the fistula is functioning well and the patient is asymptomatic. Surgery is preferred in these cases. Stent grafts have been used in cases of recurrent thrombosis, overlying skin compromise, and difficult puncture sites. However, stent grafts are less preferred due to the high chance of infection causing significant morbidity.
Complications of Endovascular Interventions
Complications usually manifest as extravasation, which is more common with repeated balloon inflations and the use of cutting balloons in resistant stenosis. Sharp recanalization techniques harbor a significant risk in the form of extravasation into the pericardial sac if perforation occurs in the intrapericardial portion of the superior vena cava, which can result in life-threatening cardiac tamponade ([Fig. 11]). Other complications include pulmonary embolism, infection, bleeding, and stent migration.

Conclusion
Knowledge of the hemodynamics and anatomy of native AVFs, their related complications, and endovascular therapeutic options for managing them is essential for an interventional radiologist.
Conflict of Interest
None declared.
Presentation at a Conference
Not presented at any conference.
-
References
- 1 Gupta R, Woo K, Yi JA. Epidemiology of end-stage kidney disease. Semin Vasc Surg 2021; 34 (01) 71-78
- 2 Dare AJ, Fu SH, Patra J, Rodriguez PS, Thakur JS, Jha P. Million Death Study Collaborators. Renal failure deaths and their risk factors in India 2001-13: nationally representative estimates from the Million Death Study. Lancet Glob Health 2017; 5 (01) e89-e95
- 3 Rajapurkar MM, John GT, Kirpalani AL. et al. What do we know about chronic kidney disease in India: first report of the Indian CKD registry. BMC Nephrol 2012; 13: 10
- 4 Modi GK, Jha V. The incidence of end-stage renal disease in India: a population-based study. Kidney Int 2006; 70 (12) 2131-2133
- 5 National Kidney Foundation. KDOQI Clinical Practice Guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis 2015; 66 (05) 884-930
- 6 Lok CE, Huber TS, Lee T. et al; National Kidney Foundation. 2019 Update. Am J Kidney Dis 2020; 75 (4, suppl 2): S1-S164
- 7 Mammen S, Keshava SN, Moses V, Babu S, Varughese S. Pictorial essay: interventional radiology in the management of hemodialysis vascular access - a single-center experience. Indian J Radiol Imaging 2012; 22 (01) 14-18
- 8 Quencer KB, Arici M. Arteriovenous fistulas and their characteristic sites of stenosis. AJR Am J Roentgenol 2015; 205 (04) 726-734
- 9 Tordoir JHM, Rooyens P, Dammers R, van der Sande FM, de Haan M, Yo TI. Prospective evaluation of failure modes in autogenous radiocephalic wrist access for haemodialysis. Nephrol Dial Transplant 2003; 18 (02) 378-383
- 10 Gibson KD, Caps MT, Kohler TR. et al. Assessment of a policy to reduce placement of prosthetic hemodialysis access. Kidney Int 2001; 59 (06) 2335-2345
- 11 Robbin ML, Greene T, Allon M. et al; Hemodialysis Fistula Maturation Study Group. Prediction of arteriovenous fistula clinical maturation from postoperative ultrasound measurements: findings from the Hemodialysis Fistula Maturation Study. J Am Soc Nephrol 2018; 29 (11) 2735-2744
- 12 Jaffer O, Gibbs P, Gibson M. et al. A UK Expert Consensus Approach for managing symptomatic arteriovenous fistula (AVF) stenosis in haemodialysis patients. Cardiovasc Intervent Radiol 2021; 44 (11) 1736-1746
- 13 Trerotola SO, Kothari S, Sammarco TE, Chittams JL. Central venous stenosis is more often symptomatic in hemodialysis patients with grafts compared with fistulas. J Vasc Interv Radiol 2015; 26 (02) 240-246
- 14 Kakkos SK, Haddad GK, Weaver MR, Haddad RK, Scully MM. Basilic vein transposition: what is the optimal technique?. Eur J Vasc Endovasc Surg 2010; 39 (05) 612-619
- 15 Beaulieu MC, Gabana C, Rose C, MacDonald PS, Clement J, Kiaii M. Stenosis at the area of transposition - an under-recognized complication of transposed brachiobasilic fistulas. J Vasc Access 2007; 8 (04) 268-274
- 16 Cooper J, Power AH, DeRose G, Forbes TL, Dubois L. Similar failure and patency rates when comparing one- and two-stage basilic vein transposition. J Vasc Surg 2015; 61 (03) 809-816
- 17 Beathard GA. An algorithm for the physical examination of early fistula failure. Semin Dial 2005; 18 (04) 331-335
- 18 Tynan-Cuisinier GS, Berman SS. Strategies for predicting and treating access induced ischemic steal syndrome. Eur J Vasc Endovasc Surg 2006; 32 (03) 309-315
- 19 Clark TW, Hirsch DA, Jindal KJ, Veugelers PJ, LeBlanc J. Outcome and prognostic factors of restenosis after percutaneous treatment of native hemodialysis fistulas. J Vasc Interv Radiol 2002; 13 (01) 51-59
- 20 Remuzzi A, Ene-Iordache B. Novel paradigms for dialysis vascular access: upstream hemodynamics and vascular remodeling in dialysis access stenosis. Clin J Am Soc Nephrol 2013; 8 (12) 2186-2193
- 21 Tedla FM, Clerger G, Distant D, Salifu M. Prevalence of central vein stenosis in patients referred for vein mapping. Clin J Am Soc Nephrol 2018; 13 (07) 1063-1068
- 22 Turmel-Rodrigues L, Mouton A, Birmelé B. et al. Salvage of immature forearm fistulas for haemodialysis by interventional radiology. Nephrol Dial Transplant 2001; 16 (12) 2365-2371
- 23 Hakim AJ, Brooke BS, Beckstrom JL, Sarfati MR, Kraiss LW. Rules of 6 criteria predict dialysis fistula maturation but not all rules are equal. J Vasc Surg 2022; 76 (01) 232-238.e2
- 24 Schmidli J, Widmer MK, Basile C. et al; Esvs Guidelines Committee, Esvs Guidelines Reviewers. Editor's choice - vascular access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55 (06) 757-818
- 25 Murphy EA, Ross RA, Jones RG. et al. Imaging in vascular access. Cardiovasc Eng Technol 2017; 8 (03) 255-272
- 26 Hughes S, Szeki I, Nash MJ, Thachil J. Anticoagulation in chronic kidney disease patients-the practical aspects. Clin Kidney J 2014; 7 (05) 442-449
- 27 Twine CP, Kakkos SK, Aboyans V. et al; ESVS Guidelines Committee, Document Reviewers. Editor's choice - European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on antithrombotic therapy for vascular diseases. Eur J Vasc Endovasc Surg 2023; 65 (05) 627-689
- 28 Cui J, Freed R, Liu F, Irani Z. Interrupting rivaling access-flow with nonsurgical image-guided ligation: the “IRANI” procedure. Semin Dial 2015; 28 (06) E53-E57
- 29 Glanz S, Gordon DH, Butt KM, Hong J, Lipkowitz GS. The role of percutaneous angioplasty in the management of chronic hemodialysis fistulas. Ann Surg 1987; 206 (06) 777-781
- 30 Singer-Jordan J, Papura S. Cutting balloon angioplasty for primary treatment of hemodialysis fistula venous stenoses: preliminary results. J Vasc Interv Radiol 2005; 16 (01) 25-29
- 31 Trerotola SO, Stavropoulos SW, Shlansky-Goldberg R, Tuite CM, Kobrin S, Rudnick MR. Hemodialysis-related venous stenosis: treatment with ultrahigh-pressure angioplasty balloons. Radiology 2004; 231 (01) 259-262
- 32 Lookstein RA, Haruguchi H, Ouriel K. et al; IN.PACT AV Access Investigators. Drug-coated balloons for dysfunctional dialysis arteriovenous fistulas. N Engl J Med 2020; 383 (08) 733-742
- 33 Kitrou PM, Katsanos K, Karnabatidis D. New evidence to support the use of drug coated balloons in the treatment of dysfunctional vascular access. Eur J Vasc Endovasc Surg 2021; 61 (04) 540-541
- 34 Da Zhuang K, Irani FG, Gogna A, Too CW, Tan BS, Tay KH. The role of drug-coated balloon in haemodialysis arteriovenous fistula stenosis management. Cardiovasc Intervent Radiol 2023; 46 (09) 1144-1153
- 35 García-Medina J, García-Alfonso JJ. Ultrasound-guided angioplasty of dysfunctional vascular access for haemodialysis. the pros and cons. Cardiovasc Intervent Radiol 2017; 40 (05) 750-754
- 36 Ross JR, Franga DL, Gallichio M, Patel AJ, Ouriel K. Role of intravascular ultrasound imaging during endovascular interventions of failing hemodialysis access grafts. J Vasc Surg 2017; 65 (05) 1383-1389
- 37 Jones RG, Willis AP, Tullett K, Riley PL. Results of stent graft placement to treat cephalic arch stenosis in hemodialysis patients with dysfunctional brachiocephalic arteriovenous fistulas. J Vasc Interv Radiol 2017; 28 (10) 1417-1421
- 38 Farrell T, Lang EV, Barnhart W. Sharp recanalization of central venous occlusions. J Vasc Interv Radiol 1999; 10 (2 Pt 1): 149-154
- 39 Honnef D, Wingen M, Günther RW, Haage P. Sharp central venous recanalization by means of a TIPS needle. Cardiovasc Intervent Radiol 2005; 28 (05) 673-676
- 40 Gupta H, Murphy TP, Soares GM. Use of a puncture needle for recanalization of an occluded right subclavian vein. Cardiovasc Intervent Radiol 1998; 21 (06) 508-511
- 41 Guimaraes M, Schonholz C, Hannegan C, Anderson MB, Shi J, Selby Jr B. Radiofrequency wire for the recanalization of central vein occlusions that have failed conventional endovascular techniques. J Vasc Interv Radiol 2012; 23 (08) 1016-1021
- 42 Baetens TR, Rotmans JI, van der Meer RW, van Rijswijk CS. A novel technique to restore access in patients with central venous occlusion using the Surfacer® Inside-Out® Access Catheter System. J Vasc Access 2020; 21 (05) 778-782
- 43 Maqsood MH, Rubab K. Quality of life of patients using the hemodialysis reliable outflow (HeRO) graft in hemodialysis. Cureus 2019; 11 (01) e3915
- 44 Tabriz DM, Arslan B. HeRO graft: indications, technique, outcomes, and secondary intervention. Semin Intervent Radiol 2022; 39 (01) 82-89
- 45 Galas N, Shahverdyan R. Use of the Surfacer® Inside-Out® Catheter Access System to obtain central venous access in dialysis patients with thoracic venous obstructions: single-center series. Vasc Endovascular Surg 2021; 55 (03) 228-233
- 46 Bakken AM, Protack CD, Saad WE, Lee DE, Waldman DL, Davies MG. Long-term outcomes of primary angioplasty and primary stenting of central venous stenosis in hemodialysis patients. J Vasc Surg 2007; 45 (04) 776-783
- 47 Maya ID, Saddekni S, Allon M. Treatment of refractory central vein stenosis in hemodialysis patients with stents. Semin Dial 2007; 20 (01) 78-82
- 48 Bjarnason H, Hunter DW, Crain MR, Ferral H, Miltz-Miller SE, Wegryn SA. Collapse of a Palmaz stent in the subclavian vein. AJR Am J Roentgenol 1993; 160 (05) 1123-1124
- 49 Anaya-Ayala JE, Smolock CJ, Colvard BD. et al. Efficacy of covered stent placement for central venous occlusive disease in hemodialysis patients. J Vasc Surg 2011; 54 (03) 754-759
- 50 McLennan G. Role of stenting for maintenance of the extremity fistula/graft overview. Cardiovasc Diagn Ther 2023; 13 (01) 260-264
- 51 Falk A, Maya ID, Yevzlin AS. RESCUE Investigators. A prospective, randomized study of an expanded polytetrafluoroethylene stent graft versus balloon angioplasty for in-stent restenosis in arteriovenous grafts and fistulae: two-year results of the RESCUE study. J Vasc Interv Radiol 2016; 27 (10) 1465-1476
- 52 Vesely T, DaVanzo W, Behrend T, Dwyer A, Aruny J. Balloon angioplasty versus Viabahn stent graft for treatment of failing or thrombosed prosthetic hemodialysis grafts. J Vasc Surg 2016; 64 (05) 1400-1410.e1
- 53 Kinning AJ, Becker RW, Fortin GJ, Molnar RG, Dall'Olmo CA. Endograft salvage of hemodialysis accesses threatened by pseudoaneurysms. J Vasc Surg 2013; 57 (01) 137-143
- 54 Nassar GM, Beathard G, Rhee E, Khan AJ, Nguyen B. Management of transposed arteriovenous fistula swing point stenosis at the basilic vein angle of transposition by stent grafts. J Vasc Access 2017; 18 (06) 482-487
- 55 Mohr BA, Sheen AL, Roy-Chaudhury P, Schultz SR, Aruny JE. REVISE Investigators. Clinical and economic benefits of stent grafts in dysfunctional and thrombosed hemodialysis access graft circuits in the REVISE randomised trial. J Vasc Interv Radiol 2019; 30 (02) 203-211.e4
- 56 Zink JN, Netzley R, Erzurum V, Wright D. Complications of endovascular grafts in the treatment of pseudoaneurysms and stenoses in arteriovenous access. J Vasc Surg 2013; 57 (01) 144-148
- 57 Thomas SD, Peden S, Katib N, Crowe P, Barber T, Varcoe RL. Long-term results of interwoven nitinol stents to treat the radiocephalic anastomotic arteriovenous fistula stenosis. J Endovasc Ther 2023; 30 (02) 176-184
- 58 Tang TY, Soon SXY, Yap CJQ. et al. Use of the helical SUPERA™ stent and Passeo-18 Lux™ drug-coated balloon to treat recurrent cephalic arch stenosis for dysfunctional brachiocephalic fistulas: 1 year results of the Arch V SUPERA-LUX study. J Vasc Access 2023; 24 (04) 591-598
- 59 Yang CC, Yang CW, Wen SC, Wu CC. Comparisons of clinical outcomes for thrombectomy devices with different mechanisms in hemodialysis arteriovenous fistulas. Catheter Cardiovasc Interv 2012; 80 (06) 1035-1041
- 60 Vogel PM, Bansal V, Marshall MW. Thrombosed hemodialysis grafts: lyse and wait with tissue plasminogen activator or urokinase compared to mechanical thrombolysis with the Arrow-Trerotola Percutaneous Thrombolytic Device. J Vasc Interv Radiol 2001; 12 (10) 1157-1165
- 61 Kitrou PM, Katsanos K, Papadimatos P, Spiliopoulos S, Karnabatidis D. A survival guide for endovascular declotting in dialysis access: procedures, devices, and a statistical analysis of 3,000 cases. Expert Rev Med Devices 2018; 15 (04) 283-291
- 62 Almehmi A, Broce M, Wang S. Thrombectomy of prosthetic dialysis grafts using mechanical plus “no-wait lysis” approach requires less procedure time and radiation exposure. Semin Dial 2011; 24 (06) 694-697
- 63 Drouven JW, de Bruin C, van Roon AM, Oldenziel J, Bokkers RPH, Zeebregts CJ. Outcomes after endovascular mechanical thrombectomy in occluded vascular access used for dialysis purposes. Catheter Cardiovasc Interv 2020; 95 (04) 758-764
- 64 Varma R, Betancourt-Torres M, Bready E, Al-Balas A. Dialysis access-associated steal syndrome with percutaneous endovascular arteriovenous fistula creation. CVIR Endovasc 2022; 5 (01) 13
- 65 Malik J, Tuka V, Kasalova Z. et al. Understanding the dialysis access steal syndrome. A review of the etiologies, diagnosis, prevention and treatment strategies. J Vasc Access 2008; 9 (03) 155-166
- 66 Cornacchiari M, Mudoni A, Di Nicolò P. et al. Peripheral hypoperfusion syndrome and monomielic syndrome: from diagnosis to treatment. Case report with review of the literature. G Ital Nefrol 2019; 36 (04) 2019-vol4
Address for correspondence
Publication History
Article published online:
13 February 2026
© 2026. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Gupta R, Woo K, Yi JA. Epidemiology of end-stage kidney disease. Semin Vasc Surg 2021; 34 (01) 71-78
- 2 Dare AJ, Fu SH, Patra J, Rodriguez PS, Thakur JS, Jha P. Million Death Study Collaborators. Renal failure deaths and their risk factors in India 2001-13: nationally representative estimates from the Million Death Study. Lancet Glob Health 2017; 5 (01) e89-e95
- 3 Rajapurkar MM, John GT, Kirpalani AL. et al. What do we know about chronic kidney disease in India: first report of the Indian CKD registry. BMC Nephrol 2012; 13: 10
- 4 Modi GK, Jha V. The incidence of end-stage renal disease in India: a population-based study. Kidney Int 2006; 70 (12) 2131-2133
- 5 National Kidney Foundation. KDOQI Clinical Practice Guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis 2015; 66 (05) 884-930
- 6 Lok CE, Huber TS, Lee T. et al; National Kidney Foundation. 2019 Update. Am J Kidney Dis 2020; 75 (4, suppl 2): S1-S164
- 7 Mammen S, Keshava SN, Moses V, Babu S, Varughese S. Pictorial essay: interventional radiology in the management of hemodialysis vascular access - a single-center experience. Indian J Radiol Imaging 2012; 22 (01) 14-18
- 8 Quencer KB, Arici M. Arteriovenous fistulas and their characteristic sites of stenosis. AJR Am J Roentgenol 2015; 205 (04) 726-734
- 9 Tordoir JHM, Rooyens P, Dammers R, van der Sande FM, de Haan M, Yo TI. Prospective evaluation of failure modes in autogenous radiocephalic wrist access for haemodialysis. Nephrol Dial Transplant 2003; 18 (02) 378-383
- 10 Gibson KD, Caps MT, Kohler TR. et al. Assessment of a policy to reduce placement of prosthetic hemodialysis access. Kidney Int 2001; 59 (06) 2335-2345
- 11 Robbin ML, Greene T, Allon M. et al; Hemodialysis Fistula Maturation Study Group. Prediction of arteriovenous fistula clinical maturation from postoperative ultrasound measurements: findings from the Hemodialysis Fistula Maturation Study. J Am Soc Nephrol 2018; 29 (11) 2735-2744
- 12 Jaffer O, Gibbs P, Gibson M. et al. A UK Expert Consensus Approach for managing symptomatic arteriovenous fistula (AVF) stenosis in haemodialysis patients. Cardiovasc Intervent Radiol 2021; 44 (11) 1736-1746
- 13 Trerotola SO, Kothari S, Sammarco TE, Chittams JL. Central venous stenosis is more often symptomatic in hemodialysis patients with grafts compared with fistulas. J Vasc Interv Radiol 2015; 26 (02) 240-246
- 14 Kakkos SK, Haddad GK, Weaver MR, Haddad RK, Scully MM. Basilic vein transposition: what is the optimal technique?. Eur J Vasc Endovasc Surg 2010; 39 (05) 612-619
- 15 Beaulieu MC, Gabana C, Rose C, MacDonald PS, Clement J, Kiaii M. Stenosis at the area of transposition - an under-recognized complication of transposed brachiobasilic fistulas. J Vasc Access 2007; 8 (04) 268-274
- 16 Cooper J, Power AH, DeRose G, Forbes TL, Dubois L. Similar failure and patency rates when comparing one- and two-stage basilic vein transposition. J Vasc Surg 2015; 61 (03) 809-816
- 17 Beathard GA. An algorithm for the physical examination of early fistula failure. Semin Dial 2005; 18 (04) 331-335
- 18 Tynan-Cuisinier GS, Berman SS. Strategies for predicting and treating access induced ischemic steal syndrome. Eur J Vasc Endovasc Surg 2006; 32 (03) 309-315
- 19 Clark TW, Hirsch DA, Jindal KJ, Veugelers PJ, LeBlanc J. Outcome and prognostic factors of restenosis after percutaneous treatment of native hemodialysis fistulas. J Vasc Interv Radiol 2002; 13 (01) 51-59
- 20 Remuzzi A, Ene-Iordache B. Novel paradigms for dialysis vascular access: upstream hemodynamics and vascular remodeling in dialysis access stenosis. Clin J Am Soc Nephrol 2013; 8 (12) 2186-2193
- 21 Tedla FM, Clerger G, Distant D, Salifu M. Prevalence of central vein stenosis in patients referred for vein mapping. Clin J Am Soc Nephrol 2018; 13 (07) 1063-1068
- 22 Turmel-Rodrigues L, Mouton A, Birmelé B. et al. Salvage of immature forearm fistulas for haemodialysis by interventional radiology. Nephrol Dial Transplant 2001; 16 (12) 2365-2371
- 23 Hakim AJ, Brooke BS, Beckstrom JL, Sarfati MR, Kraiss LW. Rules of 6 criteria predict dialysis fistula maturation but not all rules are equal. J Vasc Surg 2022; 76 (01) 232-238.e2
- 24 Schmidli J, Widmer MK, Basile C. et al; Esvs Guidelines Committee, Esvs Guidelines Reviewers. Editor's choice - vascular access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55 (06) 757-818
- 25 Murphy EA, Ross RA, Jones RG. et al. Imaging in vascular access. Cardiovasc Eng Technol 2017; 8 (03) 255-272
- 26 Hughes S, Szeki I, Nash MJ, Thachil J. Anticoagulation in chronic kidney disease patients-the practical aspects. Clin Kidney J 2014; 7 (05) 442-449
- 27 Twine CP, Kakkos SK, Aboyans V. et al; ESVS Guidelines Committee, Document Reviewers. Editor's choice - European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on antithrombotic therapy for vascular diseases. Eur J Vasc Endovasc Surg 2023; 65 (05) 627-689
- 28 Cui J, Freed R, Liu F, Irani Z. Interrupting rivaling access-flow with nonsurgical image-guided ligation: the “IRANI” procedure. Semin Dial 2015; 28 (06) E53-E57
- 29 Glanz S, Gordon DH, Butt KM, Hong J, Lipkowitz GS. The role of percutaneous angioplasty in the management of chronic hemodialysis fistulas. Ann Surg 1987; 206 (06) 777-781
- 30 Singer-Jordan J, Papura S. Cutting balloon angioplasty for primary treatment of hemodialysis fistula venous stenoses: preliminary results. J Vasc Interv Radiol 2005; 16 (01) 25-29
- 31 Trerotola SO, Stavropoulos SW, Shlansky-Goldberg R, Tuite CM, Kobrin S, Rudnick MR. Hemodialysis-related venous stenosis: treatment with ultrahigh-pressure angioplasty balloons. Radiology 2004; 231 (01) 259-262
- 32 Lookstein RA, Haruguchi H, Ouriel K. et al; IN.PACT AV Access Investigators. Drug-coated balloons for dysfunctional dialysis arteriovenous fistulas. N Engl J Med 2020; 383 (08) 733-742
- 33 Kitrou PM, Katsanos K, Karnabatidis D. New evidence to support the use of drug coated balloons in the treatment of dysfunctional vascular access. Eur J Vasc Endovasc Surg 2021; 61 (04) 540-541
- 34 Da Zhuang K, Irani FG, Gogna A, Too CW, Tan BS, Tay KH. The role of drug-coated balloon in haemodialysis arteriovenous fistula stenosis management. Cardiovasc Intervent Radiol 2023; 46 (09) 1144-1153
- 35 García-Medina J, García-Alfonso JJ. Ultrasound-guided angioplasty of dysfunctional vascular access for haemodialysis. the pros and cons. Cardiovasc Intervent Radiol 2017; 40 (05) 750-754
- 36 Ross JR, Franga DL, Gallichio M, Patel AJ, Ouriel K. Role of intravascular ultrasound imaging during endovascular interventions of failing hemodialysis access grafts. J Vasc Surg 2017; 65 (05) 1383-1389
- 37 Jones RG, Willis AP, Tullett K, Riley PL. Results of stent graft placement to treat cephalic arch stenosis in hemodialysis patients with dysfunctional brachiocephalic arteriovenous fistulas. J Vasc Interv Radiol 2017; 28 (10) 1417-1421
- 38 Farrell T, Lang EV, Barnhart W. Sharp recanalization of central venous occlusions. J Vasc Interv Radiol 1999; 10 (2 Pt 1): 149-154
- 39 Honnef D, Wingen M, Günther RW, Haage P. Sharp central venous recanalization by means of a TIPS needle. Cardiovasc Intervent Radiol 2005; 28 (05) 673-676
- 40 Gupta H, Murphy TP, Soares GM. Use of a puncture needle for recanalization of an occluded right subclavian vein. Cardiovasc Intervent Radiol 1998; 21 (06) 508-511
- 41 Guimaraes M, Schonholz C, Hannegan C, Anderson MB, Shi J, Selby Jr B. Radiofrequency wire for the recanalization of central vein occlusions that have failed conventional endovascular techniques. J Vasc Interv Radiol 2012; 23 (08) 1016-1021
- 42 Baetens TR, Rotmans JI, van der Meer RW, van Rijswijk CS. A novel technique to restore access in patients with central venous occlusion using the Surfacer® Inside-Out® Access Catheter System. J Vasc Access 2020; 21 (05) 778-782
- 43 Maqsood MH, Rubab K. Quality of life of patients using the hemodialysis reliable outflow (HeRO) graft in hemodialysis. Cureus 2019; 11 (01) e3915
- 44 Tabriz DM, Arslan B. HeRO graft: indications, technique, outcomes, and secondary intervention. Semin Intervent Radiol 2022; 39 (01) 82-89
- 45 Galas N, Shahverdyan R. Use of the Surfacer® Inside-Out® Catheter Access System to obtain central venous access in dialysis patients with thoracic venous obstructions: single-center series. Vasc Endovascular Surg 2021; 55 (03) 228-233
- 46 Bakken AM, Protack CD, Saad WE, Lee DE, Waldman DL, Davies MG. Long-term outcomes of primary angioplasty and primary stenting of central venous stenosis in hemodialysis patients. J Vasc Surg 2007; 45 (04) 776-783
- 47 Maya ID, Saddekni S, Allon M. Treatment of refractory central vein stenosis in hemodialysis patients with stents. Semin Dial 2007; 20 (01) 78-82
- 48 Bjarnason H, Hunter DW, Crain MR, Ferral H, Miltz-Miller SE, Wegryn SA. Collapse of a Palmaz stent in the subclavian vein. AJR Am J Roentgenol 1993; 160 (05) 1123-1124
- 49 Anaya-Ayala JE, Smolock CJ, Colvard BD. et al. Efficacy of covered stent placement for central venous occlusive disease in hemodialysis patients. J Vasc Surg 2011; 54 (03) 754-759
- 50 McLennan G. Role of stenting for maintenance of the extremity fistula/graft overview. Cardiovasc Diagn Ther 2023; 13 (01) 260-264
- 51 Falk A, Maya ID, Yevzlin AS. RESCUE Investigators. A prospective, randomized study of an expanded polytetrafluoroethylene stent graft versus balloon angioplasty for in-stent restenosis in arteriovenous grafts and fistulae: two-year results of the RESCUE study. J Vasc Interv Radiol 2016; 27 (10) 1465-1476
- 52 Vesely T, DaVanzo W, Behrend T, Dwyer A, Aruny J. Balloon angioplasty versus Viabahn stent graft for treatment of failing or thrombosed prosthetic hemodialysis grafts. J Vasc Surg 2016; 64 (05) 1400-1410.e1
- 53 Kinning AJ, Becker RW, Fortin GJ, Molnar RG, Dall'Olmo CA. Endograft salvage of hemodialysis accesses threatened by pseudoaneurysms. J Vasc Surg 2013; 57 (01) 137-143
- 54 Nassar GM, Beathard G, Rhee E, Khan AJ, Nguyen B. Management of transposed arteriovenous fistula swing point stenosis at the basilic vein angle of transposition by stent grafts. J Vasc Access 2017; 18 (06) 482-487
- 55 Mohr BA, Sheen AL, Roy-Chaudhury P, Schultz SR, Aruny JE. REVISE Investigators. Clinical and economic benefits of stent grafts in dysfunctional and thrombosed hemodialysis access graft circuits in the REVISE randomised trial. J Vasc Interv Radiol 2019; 30 (02) 203-211.e4
- 56 Zink JN, Netzley R, Erzurum V, Wright D. Complications of endovascular grafts in the treatment of pseudoaneurysms and stenoses in arteriovenous access. J Vasc Surg 2013; 57 (01) 144-148
- 57 Thomas SD, Peden S, Katib N, Crowe P, Barber T, Varcoe RL. Long-term results of interwoven nitinol stents to treat the radiocephalic anastomotic arteriovenous fistula stenosis. J Endovasc Ther 2023; 30 (02) 176-184
- 58 Tang TY, Soon SXY, Yap CJQ. et al. Use of the helical SUPERA™ stent and Passeo-18 Lux™ drug-coated balloon to treat recurrent cephalic arch stenosis for dysfunctional brachiocephalic fistulas: 1 year results of the Arch V SUPERA-LUX study. J Vasc Access 2023; 24 (04) 591-598
- 59 Yang CC, Yang CW, Wen SC, Wu CC. Comparisons of clinical outcomes for thrombectomy devices with different mechanisms in hemodialysis arteriovenous fistulas. Catheter Cardiovasc Interv 2012; 80 (06) 1035-1041
- 60 Vogel PM, Bansal V, Marshall MW. Thrombosed hemodialysis grafts: lyse and wait with tissue plasminogen activator or urokinase compared to mechanical thrombolysis with the Arrow-Trerotola Percutaneous Thrombolytic Device. J Vasc Interv Radiol 2001; 12 (10) 1157-1165
- 61 Kitrou PM, Katsanos K, Papadimatos P, Spiliopoulos S, Karnabatidis D. A survival guide for endovascular declotting in dialysis access: procedures, devices, and a statistical analysis of 3,000 cases. Expert Rev Med Devices 2018; 15 (04) 283-291
- 62 Almehmi A, Broce M, Wang S. Thrombectomy of prosthetic dialysis grafts using mechanical plus “no-wait lysis” approach requires less procedure time and radiation exposure. Semin Dial 2011; 24 (06) 694-697
- 63 Drouven JW, de Bruin C, van Roon AM, Oldenziel J, Bokkers RPH, Zeebregts CJ. Outcomes after endovascular mechanical thrombectomy in occluded vascular access used for dialysis purposes. Catheter Cardiovasc Interv 2020; 95 (04) 758-764
- 64 Varma R, Betancourt-Torres M, Bready E, Al-Balas A. Dialysis access-associated steal syndrome with percutaneous endovascular arteriovenous fistula creation. CVIR Endovasc 2022; 5 (01) 13
- 65 Malik J, Tuka V, Kasalova Z. et al. Understanding the dialysis access steal syndrome. A review of the etiologies, diagnosis, prevention and treatment strategies. J Vasc Access 2008; 9 (03) 155-166
- 66 Cornacchiari M, Mudoni A, Di Nicolò P. et al. Peripheral hypoperfusion syndrome and monomielic syndrome: from diagnosis to treatment. Case report with review of the literature. G Ital Nefrol 2019; 36 (04) 2019-vol4