

Subscribe to RSS
DOI: 10.1055/s-0045-1813646
Comparison of Antiplatelets and Anticoagulants for Secondary Stroke Prevention in Ischemic Stroke Patients with Cancer: A Meta-analysis
Authors

Abstract
This study aims to assess the efficacy and safety of antiplatelets (oral and subcutaneous) and anticoagulants for secondary stroke prevention in ischemic stroke patients with cancer, where the optimal antithrombotic strategy remains unclear. A systematic review and meta-analysis were conducted using PubMed, Cochrane Library, and Scopus (inception to June 2024). Studies were screened based on predefined criteria and assessed with the Newcastle-Ottawa Scale. A random-effects model (R 4.1.2) was used to calculate odds ratios (OR) with 95% confidence intervals (CI). A total of four studies were included in the final analysis. The cumulative sample size was 2,781 participants: 2,204 (79.2%) were treated with antiplatelets and 577 (20.7%) were treated with anti-coagulants. The mean age (± SD) of the patients was 69.56 (±9.88) years, and 65.7% were men. There was no difference in the risk of recurrent ischemic stroke between antiplatelets and anticoagulants (OR = 0.74, 95% CI: 0.31–1.77, 3 studies with 700 patients). There were no differences in the risk of gastrointestinal hemorrhage (OR = 1.74, 95% CI: 0.17–17.46, 2 studies with 2,101 patients) and any major hemorrhage (OR = 0.70, 95% CI: 0.24–2.05, 4 studies with 2781 patients). The odds of all-cause mortality were lower in patients treated with antiplatelets (OR = 0.73, 95% CI: 0.59–0.90, 4 studies involving 2,781 patients). Antiplatelets and anticoagulants showed no difference in recurrent stroke or major hemorrhagic events, but antiplatelets were associated with lower mortality. However, due to limited data, these findings may not fully answer the clinical question, highlighting the need for further high-quality studies.
Introduction
Approximately 15% of patients with ischemic stroke and cardiovascular disease have underlying systemic cancer.[1] The proportion of patients with ischemic stroke and underlying cancer is increasing in the United States, compared with a decrease in patients with ischemic stroke without cancer.[2] Patients with acute ischemic stroke in the setting of active cancer have a higher risk of recurrent ischemic stroke and other types of thromboembolism (34%; 95% confidence interval 28–40%).[3] Both oral anticoagulants and antiplatelet agents are considered treatment options in patients with ischemic stroke with underlying cancer.[4] The current American Heart Association and the American Stroke Association guidelines do not provide any specific recommendations for secondary prevention in patients with acute ischemic stroke with underlying cancer.[5] The guidelines from the American College of Chest Physicians, the American Society of Clinical Oncology, the National Comprehensive Cancer Network, and the International Clinical Practice Guidelines recommend low-molecular-weight heparin (LMWH) for the initial and long-term treatment of cancer patients with venous thromboembolic events, although no recommendations are provided for patients with ischemic stroke.[6] [7] [8] [9] We performed this analysis to compare the efficacy and risk of antiplatelets and anticoagulants in patients with ischemic stroke and underlying malignancy.
Materials and Methods
This meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines[10] and was registered on PROSPERO (ID: CRD42024574029).
Data Sources
A comprehensive literature search was conducted using databases such as MEDLINE (via PubMed), Cochrane Library, and Scopus. The search targeted all relevant English-language articles from the inception of each database until June 2024.
Search Strategy
The search strategy incorporated both Medical Subject Headings (MeSH) and non-MeSH terms pertinent to cancers, strokes, antiplatelet agents, and anticoagulants. Detailed search strategies for each database are provided in [Supplementary File S1] (available in the online version). Additionally, manual search techniques, including snowballing through references of relevant literature, were used to identify additional articles.
Eligibility Criteria
The Population, Intervention, Comparison, and Outcome (PICO) question for this study was defined as follows:
-
P: Patients with ischemic stroke and underlying cancer.
-
I: Antiplatelet treatment.
-
C: Anticoagulant treatment.
-
O: Safety and efficacy of antiplatelet or anticoagulants in preventing recurrent stroke and all-cause mortality.
Inclusion Criteria
-
Studies evaluate the outcomes of antiplatelet and anticoagulant therapy in ischemic stroke patients with underlying cancer in any age group or geographic location.
-
Any study designs, including observational studies, cohorts, and randomized and non-randomized controlled trials (non-RCTs).
Exclusion Criteria
-
Studies focusing on management strategies other than antiplatelets or anticoagulant treatments.
-
Reviews, case series (n < 5 patients), editorials, letters to editors, commentaries, articles published only as abstracts, and non-English publications.
Study Outcomes
We used the definitions of recurrent ischemic stroke, gastrointestinal hemorrhage, any major hemorrhage, and intracranial hemorrhage as defined by each study. In general, recurrent ischemic stroke and intracerebral hemorrhage (ICH) require confirmation by neuroimaging. Gastrointestinal hemorrhage included those events that required medical intervention or hospitalization. Any major hemorrhage included fatal bleeding, hemorrhages resulting in a hemoglobin decrease of ≥2 g/dL or necessitating transfusion of >2 units of packed cells or whole blood, bleeding in critical areas (e.g., intracranial, retroperitoneal), or requiring treatment cessation or surgical intervention. Death was ascertained through medical records or death certificates.
Article Screening and Selection
The identified articles were imported to Zotero for duplicate removal, followed by screening using the Rayyan software. Three reviewers (R.S., E.A.A., M.A.) independently assessed the titles, abstracts, and full text of the articles based on predefined eligibility criteria. Any disagreements between reviewers were resolved by a third reviewer (H.A.I.).
Data Extraction
Data from studies meeting the inclusion criteria were extracted independently by three authors (R.S., E.A.A., M.A.). Extracted data included study characteristics (author, year of publication, country of origin, study arm (antiplatelet and/or anticoagulants), study design, and sample size, patient characteristics (age, gender, and type of tumor), and outcomes (recurrent ischemic stroke, gastrointestinal hemorrhage, ICH, any major hemorrhage, and death). For each study, at least two authors independently reviewed and ascertained the data, and any conflicts were resolved by a third reviewer (H.A.I.). The refined data were processed using Google Sheets for further analysis.
Risk of Bias Assessment
Two independent reviewers (E.A.A., M.A.) independently evaluated the risk of bias of included studies using the Cochrane Risk of Bias Tool[11] for randomized studies and the Newcastle-Ottawa Scale (NOS) for observational studies. Scores across all domains were calculated, and any conflicts were resolved by a third reviewer (H.A.I.).
Statistical Analysis
The analysis was performed using the meta package in R (version 4.1.2, R Foundation for Statistical Computing). A random-effects model was used to account for variability among the included studies and to calculate pooled odds ratios (OR) for study outcomes. For each outcome, 95% confidence intervals (CIs) were computed to provide the precision of the estimates. Heterogeneity among studies was assessed using tau-squared (τ 2) and I-squared (I 2) statistics, where I 2 represents the percentage of total variation due to heterogeneity rather than chance. The Q-test was used to test the significance of heterogeneity. Differences in treatment effects across subgroups were explored through additional analyses. p-Values <0.05 were considered statistically significant.
Results
A total of four studies were included in the final analysis, as shown in the [Supplementary File S2] (available in the online version only). One study, conducted by Choi et al[12] using the National Health Insurance System (NHIS) Customized Research database, assessed 2,081 patients with cancer-related stroke: 1,829 were given only antiplatelet, 252 were given only anticoagulant drugs, and 204 received both types of antithrombotic drugs. The second study, a pilot, open-label randomized clinical trial by Navi et al[4] in the United States, enrolled 20 patients with active solid or hematological cancer. 10 patients were randomized to receive enoxaparin (1 mg/kg twice daily), and 10 to receive oral aspirin (81–325 mg/day). In the third study, a post hoc exploratory analysis by Martinez-Majander et al[13] of the multicenter NAVIGATE ESUS trial,[14] 3,609 patients (254 with cancer) were randomized to rivaroxaban, and 3,604 patients (289 with cancer) to aspirin. In the fourth study, a post hoc exploratory analysis by Navi et al[15] of the ARCADIA trial[16] (n = 1015), a subgroup of 137 patients with cancer were randomized to receive either apixaban (n = 61) or aspirin (n = 76). Martinez-Majander et al[13] reported a mean follow-up of 11 months, Navi et al[4] had a follow-up duration of 6 months, Navi et al[15] median (IQR) follow-up was 1.5 (0.6–2.5) years, whereas Choi et al[12] did not report the follow-up duration.
Choi et al,[12] Martinez-Majander et al,[13] and Navi et al[15] demonstrated good quality assessments with a low risk of bias, whereas Navi et al[4] raised some concerns due to deviations from the intended intervention and outcome measurement in the Cochrane Risk of Bias Tool.[11] The quality assessment of the trial and observational studies is presented in [Supplementary Fig. S1, S2], and [Supplementary Table S1] (available in the online version), respectively.
Of the 2,781 patients in the included studies 2,204 (79.2%) and 577 (20.7%) were treated with antiplatelet and anticoagulant treatments, respectively. The mean age (±SD) of the patients was 69.56 (±9.88) years and 65.7% were men. Study characteristics and baseline patient data are presented in [Tables 1]. The eligibility criteria of the included studies are presented in the [Supplementary Table S2] (available in the online version)>. The most common cancer was lung cancer (16.3%), closely followed by colon (15.6%), prostate (11.2%), and breast (8.5%). Hematologic tumors were seen in 123 (6.4%) patients as shown in [Supplementary Table S3] (available in the online version).
|
Author et al |
Year |
Study type |
Comparison groups |
Sample size (n) |
Age (years) (mean ± SD or median (IQR)) |
Men (n (%)) |
Follow-up duration |
|---|---|---|---|---|---|---|---|
|
Choi et al[12] |
2023 |
Population-based cohort |
AP: 1829 AC:252 Total: 2081 |
AP: 69.05 ± 10.14 AC: 67.84 ± 10.86 |
AP: 1,294 (70.75) AC: 149 (59.13) |
NR |
|
|
Majander et al[13] |
2020 |
Post hoc exploratory analysis of NAVIGATE ESUS |
Antiplatelet (Aspirin 100 mg once daily) vs. Anticoagulant (Rivaroxaban 15 mg once daily) |
AP: 289 AC: 254 Total: 543 |
72.10 ± 8.20 |
318 (59.00) |
Mean 11 mo |
|
Navi et al[4] |
2018 |
Pilot RCT |
Antiplatelet (oral aspirin 81–325 mg/day) versus anticoagulant (Enoxaparin 1 mg/kg twice daily) |
AP: 10 AC: 10 Total: 20 |
AP: 71.00 (63.00–81.00) AC: 68.00 (54.00–75.00) |
AP: 3 (30.00) AC: 2 (20.00) |
6 mo |
|
Navi et al[15] |
2024 |
Post hoc analysis of ARCADIA |
Antiplatelet (oral aspirin 81 mg once daily) vs. anticoagulant (oral apixaban, 5 mg or 2.5 mg if criteria met, twice daily) |
AP: 76 AC: 61 Total: 137 |
AP: 74 (69–80) AC: 73 (68–79) |
AP: 38 (50.0) AC: 24 (39.3) |
Median (IQR): 1.5 (0.6–2.5) y |
Abbreviations: AC, anti-coagulant; AP, anti-platelet; ARCADIA, atrial cardiopathy and antithrombotic drugs in prevention after cryptogenic stroke; IQR, interquartile range; n, number; NR, not reported; RCT, randomized controlled trial; SD, standard deviation.
a Aspirin, clopidogrel, cilostazol, ticlopidine, triflusal, dipyridamole (dosage not mentioned).
b Warfarin, low-molecular-weight heparin (dalteparin, enoxaparin, nadroparin, parnaparin, bemiparin, reviparin), and direct oral anticoagulant (apixaban, dabigatran, rivaroxaban, edoxaban); dosage not mentioned.
Recurrent Ischemic Stroke
Martinez-Majander et al,[13] Navi et al,[4] and Navi et al[15] included 700 patients (375 and 325 patients were treated with antiplatelets and anticoagulants, respectively). A total of 45 recurrent ischemic strokes, which included 21 and 24 recurrent ischemic strokes, were observed in the antiplatelet and anticoagulant-treated patients, respectively. There was no difference in the risk of recurrent ischemic stroke between antiplatelets and anticoagulants (OR: 0.74, 95% CI: 0.31–1.77, p = 0.65, I 2 = 0%, 3 studies including 700 patients) as outlined in [Fig. 1].

Gastrointestinal Hemorrhage
Choi et al[12] and Navi et al[4] included 2101 patients (1,839 and 262 patients were treated with antiplatelets and anticoagulants, respectively). A total of 50 gastrointestinal hemorrhages were observed; 43 and 7 recurrent gastrointestinal hemorrhages were found in the antiplatelet and anticoagulant-treated patients, respectively. There were no differences in the risk of gastrointestinal hemorrhage (OR: 1.74, 95% CI: 0.17–17.46, p = 0.12, I 2 = 58%) as outlined in [Fig. 2].

Intracerebral Hemorrhage
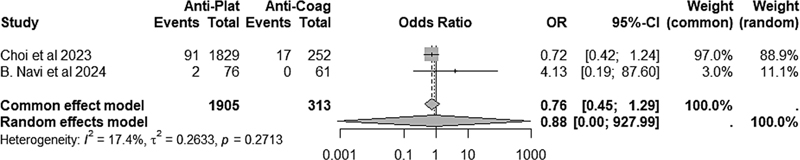
Choi et al[12] and Navi et al[15] included 2,218 patients, with 1,905 receiving antiplatelets and 313 treated with anticoagulants. A total of 110 ICHs were reported, including 93 ICH cases in the antiplatelet group and 17 in the anticoagulant group. No significant difference in ICH risk was observed between the two treatment groups (OR: 0.76, 95% CI: 0.45–1.29, I 2 = 17.4%), as illustrated in [Fig. 3].
Major Hemorrhage and Death
There was no difference in the rates of any major hemorrhage (OR = 0.70, 95% CI: 0.24–2.05, I 2 = 0%, 4 studies involving 2781 patients; [Fig. 4]). The odds of death were lower in patients treated with antiplatelets (OR = 0.73, 95% CI: 0.59–0.90, I 2 = 0%, 4 studies involving 2781 patients) as outlined in [Fig. 5].


Discussion
Cancer patients have hypercoagulability, which increases the risk for both recurrent ischemic strokes and mortality compared with those without cancer. Elevated D-dimer levels secondary to production of thrombin and urokinase-type plasminogen activators by tumor cells and platelet activation of these cells, a phenomenon known as tumor cell-induced platelet aggregation, are responsible for hypercoagulability.[17] There is a divergence in opinion regarding the choice between antiplatelet agents and anticoagulants. Based on the mechanisms discussed in the aforementioned literature, there is theoretical justification for the use of both options. Our meta-analysis included four studies, of which only one was a randomized clinical trial. The current data are limited and highlight the need for additional studies. There was no difference in the odds of recurrent ischemic stroke, gastrointestinal bleeding, ICH, or major hemorrhage in ischemic stroke patients with underlying cancer treated with anticoagulants compared with antiplatelets in our meta-analysis. However, the odds of mortality were lower among patients treated with antiplatelets compared with those treated with anticoagulants.
A recent abstract[18] reported upon 1,201 patients with cryptogenic stroke concurrent to active cancer, compared the rates of stroke recurrence and major bleeding, among patients receiving antiplatelet agents, LMWHs, warfarin, and novel oral anticoagulants, and found no differences in rates of stroke recurrence and risk of major bleeding. Additionally, it was found that antiplatelet therapy was associated with reduced risk of stroke recurrence when compared with no treatment (OR: 0.39 [95% CI: 0.17–0.89]).[18] Although we combined anticoagulants into a single group, there may be heterogeneity among various agents. The pharmacokinetic, pharmacodynamic profiles, and adverse effect profiles of agents such as direct oral anticoagulants differ considerably, which could mask clinically significant differences in efficacy and safety.[19] This variation suggests that an ideal approach would involve a larger-scale trial, similar in design to the TEACH trial,[4] to better assess individual agent effectiveness. Yamaura et al[20] demonstrated a lower rate of recurrent ischemic stroke with unfractionated heparins as compared with direct factor Xa inhibitors (competing risk analysis, p = 0.008) with no differences in cumulative rates of major bleeding complications between the two groups (p = 0.419 by competing risk analysis). However, Nam et al[21] found similar clinical and safety outcomes with both LMWHs and novel oral anticoagulants.
Our analysis contributes to the existing literature by offering a direct comparison of safety outcomes between antiplatelet and anticoagulant therapies, particularly focusing on mortality, which has not been addressed in previous studies. We also observed that ischemic stroke patients with cancer had reduced mortality when treated with antiplatelet medication compared with those treated with anticoagulants. A meta-analysis of 118 observational studies demonstrated that aspirin is associated with a 20% reduction in cancer mortality (pooled HR: 0.79; 95% CI: 0.73, 0.84 in 70 reports and a pooled OR: 0.67; 0.45, 1.00 in 11 reports) with a similar reduction also observed in all-cause mortality (HR: 0.80; 0.74, 0.86 in 56 studies and OR: 0.57; 0.36, 0.89 in seven studies).[22] This further supports our findings concerning the lower mortality rates associated with antiplatelet agents compared with anticoagulants. Two other meta-analyses (Ma et al[23] and Mädge et al[24]) have similarly shown that aspirin can reduce mortality associated with various forms of cancer. Ma et al[23] demonstrated that aspirin was associated with reduced mortality in patients with hepatocellular carcinoma (HR: 0.72, 95% CI: 0.60–0.87). Mädge et al[24] observed that aspirin use after diagnosis of colorectal cancer was associated with improved survival with a hazard ratio for cancer-related death of 0.74 (95% CI: 0.62–0.89). The underlying mechanism for this effect is unclear, and it also remains uncertain whether these effects extend to other antiplatelet agents. Nonetheless, some preclinical studies suggest a potential advantage of antiplatelets in inhibiting tumor growth and metastasis in murine melanoma and ovarian cancer models.[25] [26]
It is essential to consider potential confounding factors when interpreting our findings, such as the type of cancer treatment given to these patients. Specific cancer treatments can affect the stroke risk, complicating the assessment of antiplatelet versus anticoagulant efficacy. A 2020 study by Kitano et al[27] reported a higher stroke risk in cancer patients receiving chemotherapy versus cancer patients receiving no chemotherapy, though this association was attributed to advanced cancer stages rather than the chemotherapy itself. In contrast, a recent meta-analysis by Huang et al[28] found that patients receiving radiotherapy as part of their cancer treatment showed a twofold higher risk of subsequent stroke compared with those not undergoing radiotherapy. These factors suggest the importance of accounting for both cancer treatment type and stage in assessing the efficacy of secondary stroke prevention strategies in cancer patients.
Although our results suggested a lower mortality risk with antiplatelet agents compared with anticoagulants, it is uncertain if this effect translates to a reduced risk of recurrent ischemic stroke, bleeding events, or mortality directly related to cancer progression. While anticoagulant or antiplatelet therapy may reduce the likelihood of stroke, its potential benefit may be attenuated if patients face a significant risk of mortality from cancer progression or other causes before realizing the treatment's protective effects. We were unable to determine the cause of mortality in our cohort and thus could not determine whether the lower odds of mortality in patients treated with aspirin were due to lower rates of cancer-related, stroke-related, or cardiovascular mortality. This distinction is important to understand the mechanism of the observed benefit and inform clinical decision-making. Moreover, the type and stage of cancer may also play a significant role in both the likelihood and nature of thrombotic events. Zhang et al[29] found that survivors of head and neck, hematologic, lung, pancreas, and stomach cancer were at significantly higher risk of stroke when compared with patients without cancer, whereas other cancer types did not have significant differences. Cancer types may also influence whether a stroke arises due to direct vascular effects, such as carotid or vertebral artery involvement in atherosclerotic stroke, versus indirect effects like atrial fibrillation, potentially caused by cancer treatments.[1]
Anticoagulation therapy is indicated for certain atrial fibrillation patients to prevent cardioembolic stroke.[30] It is unclear whether anticoagulants provide the same benefit for stroke prevention in cancer. Additional studies are necessary to determine whether anticoagulation should be universally prescribed for cancer patients with atrial fibrillation, as treatment efficacy may differ based on cancer-related factors and the associated risk of bleeding complications. Overall, this points to a critical need for individualized risk assessment and targeted therapeutic strategies in cancer patients to balance the risks of bleeding, recurrent stroke, and cancer progression.
Limitations
Our ability to explore additional variables was constrained by the limited number of eligible studies meeting our strict inclusion and exclusion criteria. Of the four included studies, three were observational in design. While inherently subject to the risk of confounding factors due to many uncontrolled variables, the inclusion of observational studies is still important as they provide real-world insights in the absence of higher-quality multicenter randomized control trials.
Due to the small sample size, we may not have identified smaller differences in outcomes studied between patients treated with anticoagulants and those treated with antiplatelets. We also did not have detailed data regarding compliance with the allocated treatment. A large proportion of crossovers occurred in the TEACH (Trial of Enoxaparin vs. Aspirin in Patients with Cancer and Stroke) trial, which could have reduced the accuracy of the results.[4]
Our study did not focus exclusively on a specific type of cancer or cancers confined to one organ (e.g., brain, lung, or breast), which could have provided more focused insights. This introduces heterogeneity in the study population, as the risks of recurrent ischemic stroke, bleeding, and mortality vary significantly between different types of cancer.[31] The included studies also did not differentiate between the association of cancer and ischemic stroke by excluding other etiologies of ischemic stroke, leading to potential confounding. Furthermore, since this study is a meta-analysis, it is subject to publication bias. Hence, the perceived benefit associated with antiplatelet therapy should be interpreted with caution.
Conclusion
We did not identify any significant differences in rates of recurrent ischemic stroke or rates of intracranial hemorrhage, gastrointestinal hemorrhage, or any major hemorrhage in ischemic stroke patients with cancer treated with anticoagulants and those treated with antiplatelets. Antiplatelets were associated with reduced mortality compared with anticoagulants in this patient population. The current data suggest an equipoise between the two treatment options in ischemic stroke patients with underlying cancer and support conducting large randomized clinical trials to further determine the best treatment option in ischemic stroke patients, a population at high risk for recurrent ischemic stroke and death.
Conflict of Interest
None declared.
Authors' Contributions
M.S. contributed to the conceptualization, methodology, writing (review and editing), supervision, project administration, and formal analysis. M.A. was responsible for data curation. H.A.I. contributed to methodology and writing (review and editing). R.S. and E.A.A. were involved in data curation and writing (original draft). D.E.F., D.F.H., D.R.M., C.S.K., and W.Z. contributed to writing (review and editing). A.I.Q. was involved in conceptualization, supervision, and writing (review and editing).
-
References
- 1 Bang OY, Chung JW, Lee MJ, Seo WK, Kim GM, Ahn MJ. OASIS-Cancer Study Investigators. Cancer-related stroke: an emerging subtype of ischemic stroke with unique pathomechanisms. J Stroke 2020; 22 (01) 1-10
- 2 Sanossian N, Djabiras C, Mack WJ, Ovbiagele B. Trends in cancer diagnoses among inpatients hospitalized with stroke. J Stroke Cerebrovasc Dis 2013; 22 (07) 1146-1150
- 3 Navi BB, Singer S, Merkler AE. et al. Recurrent thromboembolic events after ischemic stroke in patients with cancer. Neurology 2014; 83 (01) 26-33
- 4 Navi BB, Marshall RS, Bobrow D. et al. Enoxaparin vs aspirin in patients with cancer and ischemic stroke: the TEACH pilot randomized clinical trial. JAMA Neurol 2018; 75 (03) 379-381
- 5 Kleindorfer DO, Towfighi A, Chaturvedi S. et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke 2021; 52 (07) e364-e467
- 6 Key NS, Khorana AA, Kuderer NM. et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol 2020; 38 (05) 496-520
- 7 Mandalà M, Labianca R. European Society for Medical Oncology. Venous thromboembolism (VTE) in cancer patients. ESMO clinical recommendations for prevention and management. Thromb Res 2010; 125 (Suppl. 02) S117-S119
- 8 Streiff MB, Holmstrom B, Angelini D. et al. NCCN guidelines insights: cancer-associated venous thromboembolic disease, version 2.2018. J Natl Compr Canc Netw 2018; 16 (11) 1289-1303
- 9 Farge D, Bounameaux H, Brenner B. et al. International clinical practice guidelines including guidance for direct oral anticoagulants in the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol 2016; 17 (10) e452-e466
- 10 Cumpston M, Li T, Page MJ. et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev 2019; 10 (10) ED000142
- 11 Sterne JAC, Savović J, Page MJ. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366: l4898
- 12 Choi BK, Lee JS, Kim HR, Kim HS, Jung YH, Park YR. Bleeding risk and mortality according to antithrombotic agents' exposure in cancer-related stroke patients: nationwide population-based cohort study in South Korea. BMC Neurol 2023; 23 (01) 187
- 13 Martinez-Majander N, Ntaios G, Liu YY. et al; NAVIGATE ESUS investigators. Rivaroxaban versus aspirin for secondary prevention of ischaemic stroke in patients with cancer: a subgroup analysis of the NAVIGATE ESUS randomized trial. Eur J Neurol 2020; 27 (05) 841-848
- 14 Hart RG, Sharma M, Mundl H. et al; NAVIGATE ESUS Investigators. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. N Engl J Med 2018; 378 (23) 2191-2201
- 15 Navi BB, Zhang C, Miller B. et al. Apixaban vs aspirin in patients with cancer and cryptogenic stroke: a post hoc analysis of the ARCADIA randomized clinical trial. JAMA Neurol 2024; 81 (09) 958-965
- 16 Kamel H, Longstreth Jr WT, Tirschwell DL. et al; ARCADIA Investigators. Apixaban to prevent recurrence after cryptogenic stroke in patients with atrial cardiopathy: the ARCADIA randomized clinical trial. JAMA 2024; 331 (07) 573-581
- 17 Lee MJ, Chung JW, Ahn MJ. et al. Hypercoagulability and mortality of patients with stroke and active cancer: the OASIS-CANCER study. J Stroke 2017; 19 (01) 77-87
- 18 Pipek L, Nascimento R, Silva GD. Secondary prevention for ischemic stroke in patients with cancer: a systematic review and network meta-analysis (P3-5.024). Neurology 2024; Apr 14; 102 (7 suppl 1): 5688 . Hagerstown, MD: Lippincott Williams & Wilkins
- 19 Eriksson BI, Quinlan DJ, Weitz JI. Comparative pharmacodynamics and pharmacokinetics of oral direct thrombin and factor xa inhibitors in development. Clin Pharmacokinet 2009; 48 (01) 1-22
- 20 Yamaura G, Ito T, Miyaji Y. et al. Therapeutic efficacy of heparin and direct factor Xa inhibitors in cancer-associated cryptogenic ischemic stroke with venous thromboembolism. Thromb Res 2021; 206: 99-103
- 21 Nam KW, Kim CK, Kim TJ. et al. Treatment of cryptogenic stroke with active cancer with a new oral anticoagulant. J Stroke Cerebrovasc Dis 2017; 26 (12) 2976-2980
- 22 Elwood PC, Morgan G, Delon C. et al. Aspirin and cancer survival: a systematic review and meta-analyses of 118 observational studies of aspirin and 18 cancers. Ecancermedicalscience 2021; 15: 1258
- 23 Ma S, Qu G, Sun C. et al. Does aspirin reduce the incidence, recurrence, and mortality of hepatocellular carcinoma? A GRADE-assessed systematic review and dose-response meta-analysis. Eur J Clin Pharmacol 2023; 79 (01) 39-61
- 24 Mädge JC, Stallmach A, Kleebusch L, Schlattmann P. Meta-analysis of aspirin-guided therapy of colorectal cancer. J Cancer Res Clin Oncol 2022; 148 (06) 1407-1417
- 25 Cho MS, Noh K, Haemmerle M. et al. Role of ADP receptors on platelets in the growth of ovarian cancer. Blood 2017; 130 (10) 1235-1242
- 26 Mezouar S, Darbousset R, Dignat-George F, Panicot-Dubois L, Dubois C. Inhibition of platelet activation prevents the P-selectin and integrin-dependent accumulation of cancer cell microparticles and reduces tumor growth and metastasis in vivo. Int J Cancer 2015; 136 (02) 462-475
- 27 The Effect of Chemotherapy on Stroke Risk in Cancer Patients - PubMed. Accessed November 2, 2024 at: https://pubmed.ncbi.nlm.nih.gov/32289866/
- 28 Huang R, Zhou Y, Hu S, Ren G, Cui F, Zhou PK. Radiotherapy exposure in cancer patients and subsequent risk of stroke: a systematic review and meta-analysis. Front Neurol 2019; 10: 233
- 29 Risk of Stroke in Cancer Survivors. A Meta-analysis of Population-Based Cohort Studies - PubMed. . Accessed November 2, 2024 at: https://pubmed.ncbi.nlm.nih.gov/33277416/
- 30 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines - PubMed. Accessed November 2, 2024 at: https://pubmed.ncbi.nlm.nih.gov/38033089/
- 31 Andersen KK, Olsen TS. Risk of ischemic and hemorrhagic strokes in occult and manifest cancers. Stroke 2018; 49 (07) 1585-1592
Address for correspondence
Publication History
Article published online:
03 December 2025
© 2025. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Bang OY, Chung JW, Lee MJ, Seo WK, Kim GM, Ahn MJ. OASIS-Cancer Study Investigators. Cancer-related stroke: an emerging subtype of ischemic stroke with unique pathomechanisms. J Stroke 2020; 22 (01) 1-10
- 2 Sanossian N, Djabiras C, Mack WJ, Ovbiagele B. Trends in cancer diagnoses among inpatients hospitalized with stroke. J Stroke Cerebrovasc Dis 2013; 22 (07) 1146-1150
- 3 Navi BB, Singer S, Merkler AE. et al. Recurrent thromboembolic events after ischemic stroke in patients with cancer. Neurology 2014; 83 (01) 26-33
- 4 Navi BB, Marshall RS, Bobrow D. et al. Enoxaparin vs aspirin in patients with cancer and ischemic stroke: the TEACH pilot randomized clinical trial. JAMA Neurol 2018; 75 (03) 379-381
- 5 Kleindorfer DO, Towfighi A, Chaturvedi S. et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke 2021; 52 (07) e364-e467
- 6 Key NS, Khorana AA, Kuderer NM. et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO Clinical Practice Guideline Update. J Clin Oncol 2020; 38 (05) 496-520
- 7 Mandalà M, Labianca R. European Society for Medical Oncology. Venous thromboembolism (VTE) in cancer patients. ESMO clinical recommendations for prevention and management. Thromb Res 2010; 125 (Suppl. 02) S117-S119
- 8 Streiff MB, Holmstrom B, Angelini D. et al. NCCN guidelines insights: cancer-associated venous thromboembolic disease, version 2.2018. J Natl Compr Canc Netw 2018; 16 (11) 1289-1303
- 9 Farge D, Bounameaux H, Brenner B. et al. International clinical practice guidelines including guidance for direct oral anticoagulants in the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol 2016; 17 (10) e452-e466
- 10 Cumpston M, Li T, Page MJ. et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev 2019; 10 (10) ED000142
- 11 Sterne JAC, Savović J, Page MJ. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366: l4898
- 12 Choi BK, Lee JS, Kim HR, Kim HS, Jung YH, Park YR. Bleeding risk and mortality according to antithrombotic agents' exposure in cancer-related stroke patients: nationwide population-based cohort study in South Korea. BMC Neurol 2023; 23 (01) 187
- 13 Martinez-Majander N, Ntaios G, Liu YY. et al; NAVIGATE ESUS investigators. Rivaroxaban versus aspirin for secondary prevention of ischaemic stroke in patients with cancer: a subgroup analysis of the NAVIGATE ESUS randomized trial. Eur J Neurol 2020; 27 (05) 841-848
- 14 Hart RG, Sharma M, Mundl H. et al; NAVIGATE ESUS Investigators. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. N Engl J Med 2018; 378 (23) 2191-2201
- 15 Navi BB, Zhang C, Miller B. et al. Apixaban vs aspirin in patients with cancer and cryptogenic stroke: a post hoc analysis of the ARCADIA randomized clinical trial. JAMA Neurol 2024; 81 (09) 958-965
- 16 Kamel H, Longstreth Jr WT, Tirschwell DL. et al; ARCADIA Investigators. Apixaban to prevent recurrence after cryptogenic stroke in patients with atrial cardiopathy: the ARCADIA randomized clinical trial. JAMA 2024; 331 (07) 573-581
- 17 Lee MJ, Chung JW, Ahn MJ. et al. Hypercoagulability and mortality of patients with stroke and active cancer: the OASIS-CANCER study. J Stroke 2017; 19 (01) 77-87
- 18 Pipek L, Nascimento R, Silva GD. Secondary prevention for ischemic stroke in patients with cancer: a systematic review and network meta-analysis (P3-5.024). Neurology 2024; Apr 14; 102 (7 suppl 1): 5688 . Hagerstown, MD: Lippincott Williams & Wilkins
- 19 Eriksson BI, Quinlan DJ, Weitz JI. Comparative pharmacodynamics and pharmacokinetics of oral direct thrombin and factor xa inhibitors in development. Clin Pharmacokinet 2009; 48 (01) 1-22
- 20 Yamaura G, Ito T, Miyaji Y. et al. Therapeutic efficacy of heparin and direct factor Xa inhibitors in cancer-associated cryptogenic ischemic stroke with venous thromboembolism. Thromb Res 2021; 206: 99-103
- 21 Nam KW, Kim CK, Kim TJ. et al. Treatment of cryptogenic stroke with active cancer with a new oral anticoagulant. J Stroke Cerebrovasc Dis 2017; 26 (12) 2976-2980
- 22 Elwood PC, Morgan G, Delon C. et al. Aspirin and cancer survival: a systematic review and meta-analyses of 118 observational studies of aspirin and 18 cancers. Ecancermedicalscience 2021; 15: 1258
- 23 Ma S, Qu G, Sun C. et al. Does aspirin reduce the incidence, recurrence, and mortality of hepatocellular carcinoma? A GRADE-assessed systematic review and dose-response meta-analysis. Eur J Clin Pharmacol 2023; 79 (01) 39-61
- 24 Mädge JC, Stallmach A, Kleebusch L, Schlattmann P. Meta-analysis of aspirin-guided therapy of colorectal cancer. J Cancer Res Clin Oncol 2022; 148 (06) 1407-1417
- 25 Cho MS, Noh K, Haemmerle M. et al. Role of ADP receptors on platelets in the growth of ovarian cancer. Blood 2017; 130 (10) 1235-1242
- 26 Mezouar S, Darbousset R, Dignat-George F, Panicot-Dubois L, Dubois C. Inhibition of platelet activation prevents the P-selectin and integrin-dependent accumulation of cancer cell microparticles and reduces tumor growth and metastasis in vivo. Int J Cancer 2015; 136 (02) 462-475
- 27 The Effect of Chemotherapy on Stroke Risk in Cancer Patients - PubMed. Accessed November 2, 2024 at: https://pubmed.ncbi.nlm.nih.gov/32289866/
- 28 Huang R, Zhou Y, Hu S, Ren G, Cui F, Zhou PK. Radiotherapy exposure in cancer patients and subsequent risk of stroke: a systematic review and meta-analysis. Front Neurol 2019; 10: 233
- 29 Risk of Stroke in Cancer Survivors. A Meta-analysis of Population-Based Cohort Studies - PubMed. . Accessed November 2, 2024 at: https://pubmed.ncbi.nlm.nih.gov/33277416/
- 30 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines - PubMed. Accessed November 2, 2024 at: https://pubmed.ncbi.nlm.nih.gov/38033089/
- 31 Andersen KK, Olsen TS. Risk of ischemic and hemorrhagic strokes in occult and manifest cancers. Stroke 2018; 49 (07) 1585-1592