
RSS-Feed abonnieren
DOI: 10.1055/s-0044-1788680
PL-TOSP, the Novel Entry Point in Transforaminal Endoscopic Spine Surgery: Radiological Analysis with Prospective Surgical Evaluation and Review of Literature of Various Skin Entry Points

Abstract
Objective Aim of this study was to analyze variation in angulation of trajectories of various skin entry points in transforaminal endoscopic spine surgery with change in the physical parameters, namely, weight, abdominal girth, and body mass index and to validate our hypothesis that posterolateral (PL)-tip of spinous process (TOSP) entry has minimal variation in the angle of trajectory as compared with currently available skin entry points. The study included an analysis of the functional outcomes of these patients who underwent transforaminal endoscopy using the novel PL-TOSP technique, assessing improvements in pain and disability. Entry point in transforaminal endoscopic lumbar discectomy (TELD) was taken as a rough distance of 10 to 12 cm from midline as proposed by Kambin whereas Yeung and Tsou advised entry point as distance between the center of the disc space and the posterior skin line measured on lateral. But entry points cannot be static as they tend to change according to changes in physical parameters.
Materials and Methods This study comprises of radiological analysis and a prospective evaluation of these patients operated on using the PL-TOSP entry point. Radiological analytic study was performed on 50 symptomatic preoperative patients who underwent transforaminal endoscopy using the novel PL-TOSP entry point. A lumbar spine magnetic resonance imaging (MRI) field of vision (MRI-FOV) was performed for the patients including the abdominal perimeter. Weight, height, and abdominal girth of the patients were noted prior to MRI. Angulation of trajectory made by four standard entry points used in TELD, namely, 45–45, PL, TOSP), dorsum of facet joint, and our proposed entry point PL-TOSP (which is a midpoint between PL and TOSP entry), were calculated using MRI-FOV at L45 and L5S1 level. For the functional outcome analysis of these 50 patients, preoperative Visual Analogue Score (VAS) for lower limb pain and Oswestry Disability Index (ODI) were recorded. Postoperative VAS and ODI scores were reassessed at 2, 6, and 12 weeks. Statistical analysis was conducted to evaluate the significance of changes in VAS scores and ODI preoperative versus postoperative. A p-value of < 0.05 was considered statistically significant.
Results Angle of trajectory with the horizontal for all five entry points varies with physical parameters. PL-TOSP entry point has the least variation with change in physical parameters as compared with other entry points. The range of angle for PL-TOSP entry was 21 to 29 degrees. In our study, there was improvement in postoperative VAS and ODI scoring systems which was statistically significant (p-value < 0.05). This suggests reliability of our proposed entry point with consistent postoperative improvement.
Conclusion The novel PL-TOSP entry point for transforaminal endoscopy demonstrates superior stability in trajectory angle despite variations in physical parameters, and is associated with significant improvements in functional outcomes and pain reduction for patients with lower limb radiculopathy. Angulation of PL-TOSP trajectory with horizontal also corresponds to current generation of endoscopes (25 or 30 degrees).
#
Introduction
Transforaminal endoscopic spine surgery provides safe passage through neural foramen to reach most of the lumbar disc pathologies without damaging the nerve roots and facet.[1] This safe posterolateral (PL) corridor between exiting and the traversing nerve root over the dorsolateral disc was first described by Kambin and Savitz.[2] This approach protects the neural structures and dura, thus preventing chronic nerve edema, epidural bleeding, and scarring.
Over the period after discovery of Kambin's triangle several innovative modifications in instrumentations of transforaminal endoscopy have taken place, thus adding to the efficacy of this approach. Technical modifications helped surgeons to better target each type of herniation and stenosis with precise needle trajectory and cannula positioning directed at the site of targeted decompression.[3]
Outcome of transforaminal endoscopy depends upon sufficient surgical decompression of the targeted nerve root. Thorough clinical examination is equally important to diagnose symptomatic nerve root. When it comes to surgical decompression of nerve root, surgeons should be able to reach compressive pathology with great precision. Optimized skin entry point selection, needle trajectory, and docking of the needle on the superior articular process (SAP) or annulus during outside-in or inside-out technique, respectively, help achieve the same.[4]
There are various described skin entry points in transforaminal endoscopic lumbar discectomy (TELD) ([Fig. 1]). Preoperative magnetic resonance imaging (MRI) and computerized tomography scan were used to determine skin entry point by measuring the distance from midline. Needle trajectory is aimed to target herniated fragments in such a way that it should not enter the peritoneal sac and damage the facet.[5] [6] All described skin entry points have their own set of advantages and disadvantages. PL and 45–45 entry points give steeper trajectories which do not provide direct access to epidural space. Thus, for the sake of complete nerve root decompression a significant amount of bony as well as ligamentary resection is required.[7] With increase in weight and body mass index (BMI), PL entry gives progressively steeper trajectory. Far lateral endoscopic approaches including dorsum of facet joint (DFJ) and tip of spinous process (TOSP) entry have direct visualization of protruded disc and epidural space. But at the same time there is increased risk of visceral and peritoneal rupture which is even more for upper lumbar levels.[8] With increase in weight and BMI, far lateral approaches become even more horizontal. Thus, it adds to the learning difficulty of transforaminal endoscopic spine surgery as patients' physical profile keeps changing.

It is the need of the hour to reduce this learning curve for beginners and improve accuracy. We need to have a unique entry point which has advantages of PL and far lateral entry points. At the same time, it should curtail down the disadvantages of both approaches. In addition to that it should provide a consistent trajectory to reach epidural space in spite of change in weight and BMI. This will be beneficial for all budding endoscopic spine surgeons to have a convenient and predictable learning curve in TELD.
We postulate that the PL-TOSP entry point proposed by us has the least variation in angular trajectory with changes in physical parameters such as weight and abdominal girth. This study aimed to analyze the variation in angulation of trajectories for various skin entry points in transforaminal endoscopic spine surgery, considering physical parameters including weight, abdominal girth, and BMI.
#
Materials and Methods
Patients and Study Design
This observational prospective study involves the radiological analysis and a prospective evaluation of the patients operated on using the PL-TOSP entry point. Institutional review board approval was obtained.
Inclusion criteria: All patients with lower limb radiculopathy who underwent MRI lumbar spine (LS) with field of vision (FOV) showing abdominal perimeter, MRI showing disc herniation or stenosis, and X-Ray showing less than grade 1 listhesis without instability were included in our study.
Exclusion criteria: Patients with more than grade 1 spondylolisthesis, infection, tumors, and deformity and MRI with inadequate FOV were excluded.
(1) Radiological analysis:
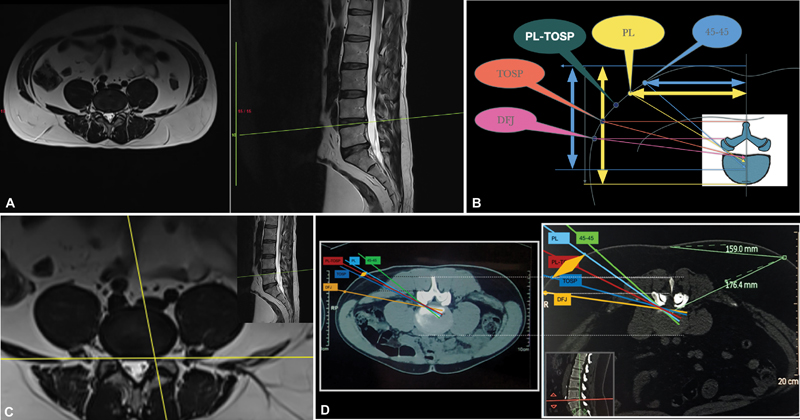
All the patients underwent measurements of height, weight, and abdominal girth prior to MRI. BMI was calculated in all patients. Radiological analysis was done as follows. MRI LS was done using SIEMENS Magnetom Spectra 3T machine. Medsynapse picture archiving and communication system was used to analyze MRI. MRI-FOV including abdominal perimeter was taken in axial T2-weighted images for measurements of angle of various skin entry point trajectories. Multiplanar reconstruction mode was used and sagittal and axial FOV image of lumbosacral spine was synchronized. Measurements were done for the last two motion segments irrespective of any transitional vertebra. MRI-FOV axial section at the level of lower discal margin of the motion segment was marked ([Fig. 2A]). Yeung endoscopic spine system (YESS) geometrical technique of drawing PL and 45–45 entry points was used for marking entry point over FOV. We marked DFJ and TOSP entry points as per Ruetten et al in every patient.[3] [6] We always measure our 5th entry point as midway between PL and TOSP ([Fig. 1E] and [F]) as per Patgaonkar et al[9] ([Fig. 2B]). Discal intersection point (DIP) is the intersection point between posterior vertebral line and medial pedicular line at lower discal margin ([Fig. 2C]). Trajectory line was drawn between the DIP and the respective skin entry point ([Fig. 2D]). Measurement of angle of trajectory with horizontal line was measured for all entry points.
#
Surgical Steps
-
All surgeries were performed under monitored anesthesia care (MAC) in a prone position on a radiolucent table using horizontal bolsters with good padding around the knee and ankle.
-
PL and 45–45 entry points were marked using the YESS technique. Using lateral fluoroscopic view of lumbosacral spine, TOSP, and DFJ entry point were marked on skin. We marked our proposed entry point PL-TOSP as midpoint of PL and TOSP ([Fig. 2B]).
-
We used PL-TOSP entry in all cases for performing TELD.
-
An 18-G 20-cm needle was inserted in Kambin's triangle under fluoroscopic guidance till it entered the annulus near the targeted decompression site
We utilized inside-out and outside-in techniques of TELD. We used Maxmoore GmbH sequential reamer for the outside-in technique.
-
A guidewire is placed once needle placement is confirmed on anteroposterior and lateral fluoroscopy. Dilator and outer sheath are inserted with due care to avoid injuring the nerve root. Patients' intraoperative feedback of leg pain, numbness, or ankle dorsiflexion weakness and active toe movement while inserting the dilator and outer sheath is recorded.
-
We used a 30-degree 18-cm shaft of 3.75 working channel endoscope in all cases.
-
Endpoint of endoscopic decompression was confirmed based on fluttering of epidural fat from the tip of SAP to the middle of the caudal pedicle, visualized decompression of traversing nerve root, and patients' pain relief.
(2) Postoperative evaluation:
Prospective analysis of these patients was performed. Study was conducted with compliance to principles of the Declaration of Helsinki. All patients were treated using transforaminal endoscopic lumbar decompression under MAC using PL-TOSP entry point. For the functional outcome analysis, preoperative Visual Analogue Score (VAS) for lower limb pain and Oswestry Disability Index (ODI) were recorded for all patients. Postoperative VAS and ODI scores were reassessed at 2, 6, and 12 weeks. Statistical analysis was performed to evaluate the significance of changes in VAS scores and ODI from preoperative to postoperative assessments.
#
Statistical Analysis
Statistical analysis was performed by SPSS 23.0 version. Continuous variables were described as mean and variation of each observation from the mean value (standard deviation [SD]) represented as mean ± SD (analyzed using independent t-test) or median and interquartile range if they failed to follow a normal distribution (analyzed using Mann–Whitney U test). Correlation for continuous variables was done using Pearson's correlation test whereas correlation for categorical variables was done using Spearman's correlation test. Paired continuous data not following normal distribution was analyzed using Wilcoxon signed rank test. Categorical variables were described by taking percentages and were analyzed using chi-square test. Variables with p-value < 0.05 were considered as statistically significant.
#
#
Results
A total of 50 patients were included in the study. The study population included 28 males and 22 females. The mean age of patients was 39.5 ± 3.54 years.
-
(1) Radiological analysis:
Mean height and weight was 159.2 ± 23.33 cm and 71.6 ± 9.33 kg, respectively, whereas mean BMI and abdominal girth was 29.1 ± 4.73 and 91.5 ± 0.71 cm, respectively. Average angles for 45–45, PL, PL-TOSP, TOSP, and DFJ entry point were 45.2 ± 1.03, 37.1 ± 2.4, 26.5 ± 2.58, 15.5 ± 1.56, and 6.9 ± 0.55, respectively. Range of angles for 45–45, PL, PL-TOSP, TOSP, and DFJ entry points was 36.5 to 56, 27 to 46.9, 21 to 29.7, 9 to 27, and 4.9 to 10, respectively. Average distances from midline for 45–45, PL, PL-TOSP, TOSP, and DFJ entry points were 8.4 ± 0.28, 10.28 ± 0.49, 13.45 ± 0.57, 16.63 ± 0.64, and 18.95 ± 0.57, respectively. Range of distance from the midline for 45–45, PL, PL-TOSP, TOSP, and DFJ entry points was 6.3 to 12.7, 7.6 to 14.8, 8.6 to 17.7, 8.7 to 22.6, and 11.6 to 24, respectively. Our study shows that an angle of trajectory with the horizontal for 45–45, PL, TOSP, and DFJ entry points has significant correlation with physical parameters with p-value < 0.05 whereas PL-TOSP entry has no statistically significant correlation with physical parameters. It means that the angle of trajectory with horizontal for PL-TOSP entry point does not change with patients' physical profile and it provides a fix range of angulation.
-
(2) Prospective evaluation:
The VAS showed a significant improvement from a preoperative median value of 8 to postoperative values of 3 at 2 weeks, 2 at 6 weeks, and 0 at 12 weeks (p < 0.001). Additionally, the ODI scores demonstrated a statistically significant enhancement from the preoperative period to 2, 6, and 12 weeks postoperatively (p < 0.001) ([Table 1]). Postoperative dysesthesia was observed in one patient.
Abbreviations: ODI, Oswestry Disability Index; VAS, Visual Analogue Score.
#
Discussion
Minimally invasive spine surgery has evolved over the years with several variations in approaching LS.[10] Hijikata described PL nucleotomy for lumbar disc herniations in 1975.[11] Based on the description of safe working zone between exiting and traversing nerve root by Kambin, the first endoscopic discectomy was performed in 1988.[12] In the era of minimally invasive spine surgery, TELD has become a standard procedure. Transforaminal endoscopy provides access to the intervertebral disc space through the Kambin's triangle between traversing and exiting nerve root without damaging the posterior bony or ligamentous structures.[13] [14] Generally, lumbar disc herniations are commonly found in lower lumbar disc levels.
Central and paracentral herniations and lateral recess stenosis are the most common indications for transforaminal endoscopic spine surgery.[3] [15] [16]
Transforaminal endoscopy generally has two approaches—intraforaminal intradiscal and intraforaminal extradiscal. The former is better accessed through PL entries like 45–45 and PL, whereas the latter is better accessed through far lateral entry points like DFJ and TOSP.[17] [18]
Entry point for TELD has always been a point of debate. Kambin et al has given a rough distance of 10 to 12 cm from midline as the entry point and the angle of trajectory around 35 to 45 degrees.[19] But entry points cannot be static as they tend to change according to changes in physical parameters and thus it affects the trajectory of the transforaminal approach.[9] Thus, a fix distance from the midline may have trajectory with different angles in different individuals.
Yeung and Tsou described radiology-based entry point as distance between the center of the disc space to the posterior skin line measured on lateral fluoroscopy. The same length is measured perpendicular from the midline to get the entry point. The access angle of Yeung's technique by 45–45 entry point has been considered to be between 25 and 30 degrees to the frontal plane. Ruetten et al described the inferior most limitation of entry point to be the dorsum of inferior articular process seen on lateral fluoroscopy. Extreme lateral approach described by Ruetten et al is considered to provide a trajectory of 10 degrees.[6] [20] [21] [22] [23] In our study, we found that range of angles for 45–45, PL, PL-TOSP, TOSP, and DFJ entry points was 36.5 to 56, 27 to 46.9, 21 to 29.7, 9 to 27, and 4.9 to 10 degrees, respectively. Average angle for 45–45, PL, PL-TOSP, TOSP, and DFJ entry point was 45.2 ± 1.03, 37.1 ± 2.4, 26.5 ± 2.58, 15.5 ± 1.56, and 6.9 ± 0.55, respectively. Hence, we found significant variation in 45–45 entry point with increasing abdominal girth. With change in physical parameters 45–45 and PL entries becomes more steeper whereas DFJ and TOSP get more shallower. Our proposed entry point PL-TOSP has the least variation in the angle of trajectory with variation in physical parameters. It also provides an average trajectory of 26 degrees which is also consistent with the current generations of endoscopes with optics of 25 to 30 degrees.
Advantage of far lateral entry points like TOSP and DFJ is that central and paracentral disc herniations can be better accessed with optimum visualization. Hence, these entry points are advised for direct visualization of ventral epidural space. On the contrary, chances of exiting nerve root injury are high. In case of PL entry points like PL and 45–45, trajectory is dorsal to dorsolumbar fascia and peritoneum thus avoids damage to the visceral structures. Similarly, these entry points avoid damage to the exiting nerve root by being more vertical in trajectory. On the contrary, it does not provide sufficient access to the ventral epidural space which may lead to insufficient decompression in transligamentary and sequestered herniations and more foraminotomy and annulotomy are required to reach the offending pathology.
Large and sequestrated herniation in narrow foramen in the lower lumbar disc levels demands the need of more lateral approach but at the same time there is a risk of damaging internal organs because of more horizontal trajectory. Ideal endoscopic approach should impart minimum damage to the nonpathological anatomical structures but at the same time provide maximum visualization of pathoanatomy. For transforaminal endoscopic access entry point optimization is of utmost importance to reach the concerned pathology without damaging the nerve root, retroperitoneal space, or normal bony ligamentous anatomy.
PL-TOSP entry point provides a consistent middle path between PL and far lateral entry point trajectories having advantages of both minimizing risk and limitations of both the extreme approaches, thus with this novel entry point we are retaining advantages of both PL and TOSP entry points, minimizing the complications. The findings support the superior stability of the PL-TOSP entry point and its association with significant improvements in functional outcomes and pain reduction for patients with lower limb radiculopathy. This indicates that the PL-TOSP entry point is an effective and reliable technique for achieving better clinical results in lower lumbar endoscopic spine surgery. We encountered one complication in the form of dysesthesia. None of our patient had deterioration in neurology, discitis, dural tear, or bowel injury.
Beveled-shaped wide angle working channel endoscope and working sleeve provide direct visualization and access to the epidural space, annulus, and subannular intradiscal content just by maneuvering the endoscope in the line of trajectory. But to get optimum visualization, the trajectory should match the endoscope's angle of optics. Current generation transforaminal endoscopes are available in the range of 25- to 30-degree optics. Trajectory provided by the PL-TOSP entry corresponds to this current generation of endoscope on a consistent basis (p-value < 0.549).[24]
Patgaonkar et al[9] has suggested a formula to calculate PL-TOSP entry point from the midline based on physical parameters of weight and abdominal girth at the level of umbilicus.
Our study demonstrates significant improvements in functional outcomes and pain reduction in patients with lower limb radiculopathy who underwent transforaminal endoscopy using the novel PL-TOSP entry point. In our study, the VAS demonstrated a significant reduction from a preoperative median value of 8 to postoperative values of 3 at 2 weeks, 2 at 6 weeks, and 0 at 12 weeks (p < 0.001). Similarly, the ODI scores showed statistically significant improvements from the preoperative period to 2, 6, and 12 weeks postoperatively (p < 0.001). These findings are consistent with those of Knight et al, who reported substantial long-term improvements in VAS and ODI scores following transforaminal endoscopic lumbar decompression and foraminoplasty, with a majority of patients experiencing “excellent” or “good clinical impact” outcomes over a 10-year follow-up period.[25] Additionally, our results align with the study of Nair et al, who observed significant reductions in VAS and ODI scores in a rural Indian cohort undergoing transforaminal endoscopic discectomy, highlighting the procedure's effectiveness in diverse patient populations.[26] Furthermore, Wang et al reported better functional outcomes and pain relief with percutaneous endoscopic transforaminal discectomy compared with microdiscectomy, further supporting the efficacy of endoscopic approaches in spinal surgeries.[27]
#
Conclusion
The novel PL-TOSP entry point in transforaminal endoscopic spine surgery provides a consistent and predictable trajectory with an average angle of 26 degrees, yielding excellent functional outcomes. It is compatible with current generation working channel endoscopes equipped with 25- to 30-degree optics. Further clinical studies are necessary to validate the efficacy of the PL-TOSP entry in transforaminal endoscopic spine procedures.
#
#
Conflict of Interest
None declared.
Authors' Contributions
P.P. contributed to the concept and study design. K.D. was involved in the study design, manuscript writing, data analysis, and review of literature. S.K. took care of editing and proof reading, while V.G. managed data collection. Lastly, V.P. handled data analysis.
-
References
- 1 Yeung AT. The evolution and advancement of endoscopic foraminal surgery: one surgeon's experience incorporating adjunctive technologies. SAS J 2007; 1 (03) 108-117
- 2 Kambin P, Savitz MH. Arthroscopic microdiscectomy: an alternative to open disc surgery. Mt Sinai J Med 2000; 67 (04) 283-287
- 3 Yue JJ, Long W. Full endoscopic spinal surgery techniques: advancements, indications, and outcomes. Int J Spine Surg 2015; 9: 17
- 4 Datar G, Shinde A, Bommakanti K. Technical consideration of transforaminal endoscopic spine surgery for central herniation. Indian J Pain 2017; 31 (02) 86
- 5 Ahn Y. Transforaminal percutaneous endoscopic lumbar discectomy: technical tips to prevent complications. Expert Rev Med Devices 2012; 9 (04) 361-366
- 6 Ruetten S, Komp M, Godolias G. An extreme lateral access for the surgery of lumbar disc herniations inside the spinal canal using the full-endoscopic uniportal transforaminal approach-technique and prospective results of 463 patients. Spine 2005; 30 (22) 2570-2578
- 7 Kambin P, O'Brien E, Zhou L, Schaffer JL. Arthroscopic microdiscectomy and selective fragmentectomy. Clin Orthop Relat Res 1998; (347) 150-167
- 8 Lee JU, Park KJ, Kim KH, Choi MK, Lee YH, Kim DH. What is the ideal entry point for transforaminal endoscopic lumbar discectomy?. J Korean Neurosurg Soc 2020; 63 (05) 614-622
- 9 Patgaonkar P, Goyal V, Agrawal U, Marathe N, Patel V. Impact of body weight, height, and obesity on selection of skin entry point for transforaminal endoscopic lumbar discectomy. Asian J Neurosurg 2022; 17 (02) 262-267
- 10 Hult L. Retroperitoneal disc fenestration in low-back pain and sciatica; a preliminary report. Acta Orthop Scand 1951; 20 (04) 342-348
- 11 Hijikata S. Percutaneous nucleotomy. A new concept technique and 12 years' experience. Clin Orthop Relat Res 1989; (238) 9-23
- 12 Kambin P. Percutaneous lumbar discectomy (Triangular Working Zone). In: Current Practice Surgical Rounds in Orthopaedics. Clinical Orthopaedics and Related Research; Department of Orthopaedic Surgery, Graduate Hospital; Philadelphia, PA: 1988: 31-35
- 13 Kambin P. Arthroscopic microdiscectomy. In: Mayer HM. ed. Minimally Invasive Spine Surgery. Berlin, Heidelberg: Springer Berlin Heidelberg; 2000: 187-199
- 14 Savitz MH. Same-day microsurgical arthroscopic lateral-approach laser-assisted (SMALL) fluoroscopic discectomy. J Neurosurg 1994; 80 (06) 1039-1045
- 15 Kitagawa Y, Sairyo K, Shibuya I. et al. Minimally invasive and simultaneous removal of herniated intracanal and extracanal lumbar nucleus pulposus with a percutaneous spinal endoscope. Asian J Endosc Surg 2012; 5 (04) 183-186
- 16 Lübbers T, Abuamona R, Elsharkawy AE. Percutaneous endoscopic treatment of foraminal and extraforaminal disc herniation at the L5-S1 level. Acta Neurochir (Wien) 2012; 154 (10) 1789-1795
- 17 Yeung AT. The evolution of percutaneous spinal endoscopy and discectomy: state of the art. Mt Sinai J Med 2000; 67 (04) 327-332
- 18 Ruetten S, Komp M, Merk H, Godolias G. Use of newly developed instruments and endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J Neurosurg Spine 2007; 6 (06) 521-530
- 19 Kambin P, Casey K, O'Brien E, Zhou L. Transforaminal arthroscopic decompression of lateral recess stenosis. J Neurosurg 1996; 84 (03) 462-467
- 20 Yeung AT, Yeung CA. Advances in endoscopic disc and spine surgery: foraminal approach. Surg Technol Int 2003; 11: 255-263
- 21 Lewandrowski KU. The strategies behind “inside-out” and “outside-in” endoscopy of the lumbar spine: treating the pain generator. J Spine Surg 2020; 6 (Suppl. 01) S35-S39
- 22 Gore S, Yeung A. The “inside out” transforaminal technique to treat lumbar spinal pain in an awake and aware patient under local anesthesia: results and a review of the literature. Int J Spine Surg 2014; 8: 28
- 23 Kim HS, Adsul N, Kapoor A. et al. A mobile outside-in technique of transforaminal lumbar endoscopy for lumbar disc herniations. J Vis Exp 2018; (138) 57999
- 24 Yeung AT, Tsou PM. Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases. Spine 2002; 27 (07) 722-731
- 25 Knight MTN, Jago I, Norris C, Midwinter L, Boynes C. Transforaminal endoscopic lumbar decompression & foraminoplasty: a 10 year prospective survivability outcome study of the treatment of foraminal stenosis and failed back surgery. Int J Spine Surg 2014; 8: 21
- 26 Nair VV, Kohli S, Vishwakarma N, Mhatre J. Outcome of transforaminal endoscopic discectomy in rural India in a single-level lumbar disc prolapse under local anesthesia. Asian J Neurosurg 2023; 18 (02) 312-320
- 27 Wang SF, Hung SF, Tsai TT. et al. Better functional outcome and pain relief in the far-lateral-outside-in percutaneous endoscopic transforaminal discectomy. J Pain Res 2021; 14: 3927-3934
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
30. Juli 2024
© 2024. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Yeung AT. The evolution and advancement of endoscopic foraminal surgery: one surgeon's experience incorporating adjunctive technologies. SAS J 2007; 1 (03) 108-117
- 2 Kambin P, Savitz MH. Arthroscopic microdiscectomy: an alternative to open disc surgery. Mt Sinai J Med 2000; 67 (04) 283-287
- 3 Yue JJ, Long W. Full endoscopic spinal surgery techniques: advancements, indications, and outcomes. Int J Spine Surg 2015; 9: 17
- 4 Datar G, Shinde A, Bommakanti K. Technical consideration of transforaminal endoscopic spine surgery for central herniation. Indian J Pain 2017; 31 (02) 86
- 5 Ahn Y. Transforaminal percutaneous endoscopic lumbar discectomy: technical tips to prevent complications. Expert Rev Med Devices 2012; 9 (04) 361-366
- 6 Ruetten S, Komp M, Godolias G. An extreme lateral access for the surgery of lumbar disc herniations inside the spinal canal using the full-endoscopic uniportal transforaminal approach-technique and prospective results of 463 patients. Spine 2005; 30 (22) 2570-2578
- 7 Kambin P, O'Brien E, Zhou L, Schaffer JL. Arthroscopic microdiscectomy and selective fragmentectomy. Clin Orthop Relat Res 1998; (347) 150-167
- 8 Lee JU, Park KJ, Kim KH, Choi MK, Lee YH, Kim DH. What is the ideal entry point for transforaminal endoscopic lumbar discectomy?. J Korean Neurosurg Soc 2020; 63 (05) 614-622
- 9 Patgaonkar P, Goyal V, Agrawal U, Marathe N, Patel V. Impact of body weight, height, and obesity on selection of skin entry point for transforaminal endoscopic lumbar discectomy. Asian J Neurosurg 2022; 17 (02) 262-267
- 10 Hult L. Retroperitoneal disc fenestration in low-back pain and sciatica; a preliminary report. Acta Orthop Scand 1951; 20 (04) 342-348
- 11 Hijikata S. Percutaneous nucleotomy. A new concept technique and 12 years' experience. Clin Orthop Relat Res 1989; (238) 9-23
- 12 Kambin P. Percutaneous lumbar discectomy (Triangular Working Zone). In: Current Practice Surgical Rounds in Orthopaedics. Clinical Orthopaedics and Related Research; Department of Orthopaedic Surgery, Graduate Hospital; Philadelphia, PA: 1988: 31-35
- 13 Kambin P. Arthroscopic microdiscectomy. In: Mayer HM. ed. Minimally Invasive Spine Surgery. Berlin, Heidelberg: Springer Berlin Heidelberg; 2000: 187-199
- 14 Savitz MH. Same-day microsurgical arthroscopic lateral-approach laser-assisted (SMALL) fluoroscopic discectomy. J Neurosurg 1994; 80 (06) 1039-1045
- 15 Kitagawa Y, Sairyo K, Shibuya I. et al. Minimally invasive and simultaneous removal of herniated intracanal and extracanal lumbar nucleus pulposus with a percutaneous spinal endoscope. Asian J Endosc Surg 2012; 5 (04) 183-186
- 16 Lübbers T, Abuamona R, Elsharkawy AE. Percutaneous endoscopic treatment of foraminal and extraforaminal disc herniation at the L5-S1 level. Acta Neurochir (Wien) 2012; 154 (10) 1789-1795
- 17 Yeung AT. The evolution of percutaneous spinal endoscopy and discectomy: state of the art. Mt Sinai J Med 2000; 67 (04) 327-332
- 18 Ruetten S, Komp M, Merk H, Godolias G. Use of newly developed instruments and endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J Neurosurg Spine 2007; 6 (06) 521-530
- 19 Kambin P, Casey K, O'Brien E, Zhou L. Transforaminal arthroscopic decompression of lateral recess stenosis. J Neurosurg 1996; 84 (03) 462-467
- 20 Yeung AT, Yeung CA. Advances in endoscopic disc and spine surgery: foraminal approach. Surg Technol Int 2003; 11: 255-263
- 21 Lewandrowski KU. The strategies behind “inside-out” and “outside-in” endoscopy of the lumbar spine: treating the pain generator. J Spine Surg 2020; 6 (Suppl. 01) S35-S39
- 22 Gore S, Yeung A. The “inside out” transforaminal technique to treat lumbar spinal pain in an awake and aware patient under local anesthesia: results and a review of the literature. Int J Spine Surg 2014; 8: 28
- 23 Kim HS, Adsul N, Kapoor A. et al. A mobile outside-in technique of transforaminal lumbar endoscopy for lumbar disc herniations. J Vis Exp 2018; (138) 57999
- 24 Yeung AT, Tsou PM. Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases. Spine 2002; 27 (07) 722-731
- 25 Knight MTN, Jago I, Norris C, Midwinter L, Boynes C. Transforaminal endoscopic lumbar decompression & foraminoplasty: a 10 year prospective survivability outcome study of the treatment of foraminal stenosis and failed back surgery. Int J Spine Surg 2014; 8: 21
- 26 Nair VV, Kohli S, Vishwakarma N, Mhatre J. Outcome of transforaminal endoscopic discectomy in rural India in a single-level lumbar disc prolapse under local anesthesia. Asian J Neurosurg 2023; 18 (02) 312-320
- 27 Wang SF, Hung SF, Tsai TT. et al. Better functional outcome and pain relief in the far-lateral-outside-in percutaneous endoscopic transforaminal discectomy. J Pain Res 2021; 14: 3927-3934