

Subscribe to RSS
DOI: 10.1055/s-0044-1787690
Role of Ultrasonography in the Evaluation of Retained Products of Conception
Authors
Funding None.

Abstract
“Retained products of conception” (RPOC) account for a significant number of radiology clinical visits in the postnatal or postabortive period. Any delay in receiving the necessary treatment can lead to further complications and may even prove lethal. On the other hand, overtreatment where none is required may also lead to complications and can affect future conceptions. Therefore, a timely and accurate detection of RPOC is essential in saving the life and preventing future complications. Ultrasonography helps in diagnosing and quantifying the RPOC and is, therefore, important when choosing the course of management for the patient. Various findings in pathologically confirmed cases of RPOC have been described in the literature. However, a significant overlap with the normal postnatal findings is seen. This article aims to describe the various features of RPOC on ultrasound, which may increase the diagnostic confidence of the radiologists in cases of RPOC. The RPOC mimics and features that may help differentiate them have also been briefly discussed.
Introduction
The term retained products of conception (RPOC) refers to placental and/or fetal tissue that remains in the uterus after a spontaneous pregnancy loss (miscarriage), planned pregnancy termination, or preterm/term delivery. The fact that RPOC are present after a spontaneous pregnancy loss differentiates an incomplete from a complete miscarriage. The prevalence of RPOC is approximately 2.7% in women after a third-trimester delivery. It is seen in approximately 40% of pregnancies terminating during the fourth to sixth month and in 17% of pregnancies terminating during the first 3 months.[1] The overall incidence of RPOC after a normal vaginal delivery lies around 3 to 5%.[2] Timely diagnosis is crucial for deciding the management of hemorrhage and for averting associated direct complications, which include perforation, infection, and future obstetric implications. Given that complications associated with surgical interventions, including infection, perforation, formation of the scar tissue, and Asherman's syndrome, can have long-term negative consequences on future gestations, precise diagnosis is essential.
Role of Ultrasonography
Grayscale Ultrasound
The most sensitive sign of RPOC at B-mode ultrasound (US) imaging is thickened “endometrial echo complex” (EEC; [Fig. 1]). The estimated cut-off of “thickened” EEC ranges in the previous studies from 8 to 13 mm, depending upon the level of clinical suspicion.[3] [4] Another B-mode US finding that may represent the RPOC is the visualization of an endometrial or an intrauterine mass.[5] [6] An intrauterine mass can be defined as an area separate from the underlying endometrium that is clearly differentiated in two perpendicular planes. The extent of invasion of the myometrium by the RPOC should also be evaluated to look for any possibility of placenta accreta, which, if present, changes the line of management.

Color Doppler Ultrasound
Color Doppler additionally increases the diagnostic confidence as blood clots will be avascular on color Doppler, while the detection of color flow in an endometrial mass or thickened EEC is more likely to correspond to RPOC.[7] To better elucidate typical color Doppler findings for RPOC, the degree of vascularity of the endometrial component can be equated with myometrial vascularity in the same section of the image and classified as type 0, 1, 2, or 3 ([Fig. 2]).[7]
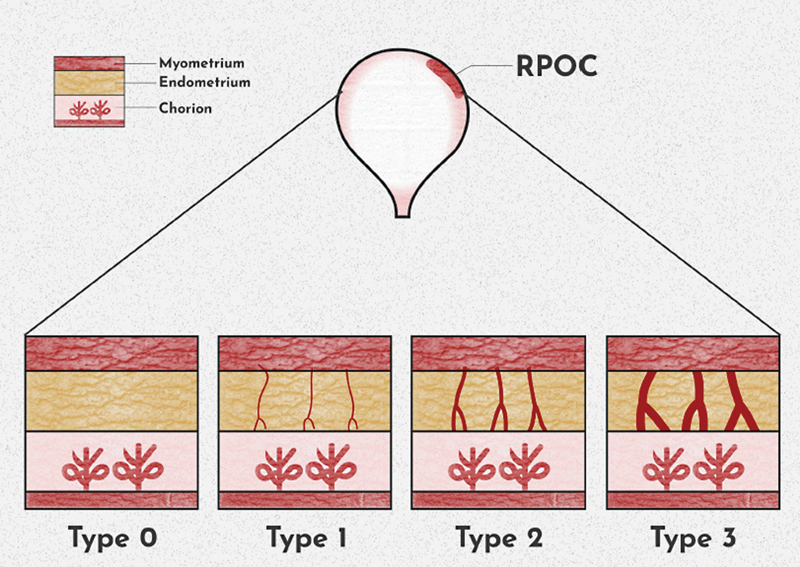
Type 0 vascularity indicates the absence of any detectable flow in a mass or thickened EEC, which could stem from either a clot or an avascular RPOC ([Figs. 3] and [4]).[7] While an avascular thickened endometrium may signify RPOC, it typically does not lead to significant bleeding and eliminates the necessity for surgical intervention. Type 1 denotes minimal vascularization, less than that in the myometrium, with a positive predictive value (PPV) exceeding 90% ([Fig. 5]).[7] Type 2, or moderate vascularity where flow in the endometrium is nearly equal to that in the myometrium, demonstrates a PPV of 100% ([Fig. 6]).[7] Type 3, characterized by marked/severe endometrial vascularity surpassing that of a normal myometrium, also exhibits a PPV of 100% ([Fig. 7]).[7] Notably, type 3 vascularity can be so robust that it resembles an arteriovenous malformation (AVM) on color Doppler. In type 3 RPOC, spectral waveform may show a very low-resistance pattern and, occasionally, dilated vessels may be visible ([Fig. 8]).[7] The key distinguishing feature is that in RPOC, vascularity is consistently observed to continue from the myometrium into the endometrium. Hence, if blood flow is confined to the myometrium, diagnoses other than RPOC should be considered. Obstetricians should be alerted to type 3 RPOC with marked vascularity, as inadvertent injury to a large vessel during dilation and curettage poses a high risk of hemorrhage.






Differential Diagnosis
Blood Clots
The most common difficulty in patients presenting with provisional diagnosis of RPOC is differentiating between avascular RPOC and blood clots. Few authors have suggested that such cases should be treated conservatively and followed up with sonographic evaluation during the follicular phase of the next menstrual cycle.[8]
Enhanced Myometrial Vascularity/Arteriovenous Malformation
The biggest difficulty in diagnosing RPOC is misidentifying the pronounced vascularity for an AVM (a rare entity, now also known as enhanced myometrial vascularity [EMV]). RPOC can be differentiated from AVMs on the basis of the extent of vascularity. Uterine AVMs mainly involve only the myometrium, whereas in RPOC, the vascularity will extend into the endometrium as well ([Fig. 9]).

Endometrial Diseases
Endometrial abnormalities, for example, an endometrial polyp ([Fig. 10]) or a submucosal fibroid ([Fig. 11]), are other potential mimics of RPOC because of a similar presentation of mass with vascularity.


Subinvolution of Placental Site
A rare postpartum condition, in which failure of involution of modified dilated spiral arteries is seen, is also a differential of RPOC as it presents with severe postpartum hemorrhage. In the absence of echogenic contents in endometrial cavity, US findings of hypoechoic tortuous vessels along the inner myometrium may raise the suspicion for subinvolution of placental site (SPS). However, these findings are nonspecific. It is usually a diagnosis of exclusion and needs histological confirmation.[9]
Invasive Moles
RPOC and invasive moles may show some similarity in imaging findings; however, the clinical features usually help in differentiation. Any history of previous molar pregnancy with persistently high and rising human chorionic gonadotropin (hugs) levels is important in diagnosing an invasive mole. On US, an invasive mole can be seen as an ill-defined mass in the uterus showing anechoic areas within ([Fig. 12]). Color Doppler findings reveal increased vascularity, particularly in the myometrium due to myometrial invasion ([Fig. 13]).


The Dilemma
The plethora of normal postpartum findings seen in ultrasonography makes the diagnosis of RPOC more difficult. Various studies have tried to establish the cutoff values for labeling the RPOC; however, no consensus has been reached yet.
For instance, McEwing et al stated that a fluid collection within the uterine cavity after termination is normal and is likely to denote blood. Retained products have a more solid appearance, but blood clots and necrotic decidua within the cavity can mimic residual tissue. It was emphasized that thickened, heterogeneous endometrial contents, with or without increased color Doppler flow, should be taken as a part of the normal spectrum of post-termination US findings, and a more conservative approach should be used to report suspected RPOC after termination. Also, the US reports should be tailed by a disclaimer that these findings are commonly seen in asymptomatic women after termination.[10]
The major use of US after termination in the first trimester is for the confirmation of expulsion of gestational sac. However, the thickness of the endometrium is not a reliable predictor for the requirement of further surgical intervention when gestational sac expulsion has been established. Therefore, in managing early pregnancy failure, clinical presentation and not endometrial thickness should be utilized to define the requirement for intervention.[11] These findings were in agreement with those of Napolitano et al, who reported that sonographic suspicion of RPOC does not competently predict the need for surgery.[12]
Bar-Hava et al also found that the uterine cavity was rarely empty in the first few days following a first-trimester abortion. The intrauterine material tends to be hyperechoic to begin with and hypoechoic later in the week, indicating that the uterine content may be composed of liquefying or absorbing blood clots. The presence of thick heterogeneous intrauterine material is a finding that can be expected after a first-trimester abortion and does not incontrovertibly require intervention.[8]
RPOC can be treated conservatively with expectant management or with surgical intervention. Fujishima et al reported that in asymptomatic cases, intervention should be avoided and the patient should be managed conservatively.[13] Another study suggested a cutoff of 4.4 cm (long axis of RPOC) for deciding whether invasive procedures should be done or avoided. Proper guidelines regarding the sonographic indications for deciding the course of management are lacking in the literature and need further research.[14]
Conclusion
Thickened EEC and intrauterine mass with vascularity are suggestive of RPOC. The potential differentials have to be kept in mind while evaluating any patient with suspicion of RPOC. Nevertheless, US alone is seldom decisive and, therefore, clinical presentation and sonographic findings should together be considered to decide the lines of clinical management.
Conflict of Interest
None declared.
-
References
- 1 van den Bosch T, Daemen A, Van Schoubroeck D, Pochet N, De Moor B, Timmerman D. Occurrence and outcome of residual trophoblastic tissue: a prospective study. J Ultrasound Med 2008; 27 (03) 357-361
- 2 Epperly TD, Fogarty JP, Hodges SG. Efficacy of routine postpartum uterine exploration and manual sponge curettage. J Fam Pract 1989; 28 (02) 172-176
- 3 Sadan O, Golan A, Girtler O. et al. Role of sonography in the diagnosis of retained products of conception. J Ultrasound Med 2004; 23 (03) 371-374
- 4 Ustunyurt E, Kaymak O, Iskender C, Ustunyurt OB, Celik C, Danisman N. Role of transvaginal sonography in the diagnosis of retained products of conception. Arch Gynecol Obstet 2008; 277 (02) 151-154
- 5 Atri M, Rao A, Boylan C, Rasty G, Gerber D. Best predictors of grayscale ultrasound combined with color Doppler in the diagnosis of retained products of conception. J Clin Ultrasound 2011; 39 (03) 122-127
- 6 Alcázar JL, Baldonado C, Laparte C. The reliability of transvaginal ultrasonography to detect retained tissue after spontaneous first-trimester abortion, clinically thought to be complete. Ultrasound Obstet Gynecol 1995; 6 (02) 126-129
- 7 Kamaya A, Petrovitch I, Chen B, Frederick CE, Jeffrey RB. Retained products of conception: spectrum of color Doppler findings. J Ultrasound Med 2009; 28 (08) 1031-1041
- 8 Bar-Hava I, Aschkenazi S, Orvieto R. et al. Spectrum of normal intrauterine cavity sonographic findings after first-trimester abortion. J Ultrasound Med 2001; 20 (12) 1277-1281
- 9 Petrovitch I, Beatty M, Jeffrey RB, Heerema-McKenney A. Subinvolution of the placental site. J Ultrasound Med 2009; 28 (08) 1115-1119
- 10 McEwing RL, Anderson NG, Meates JB, Allen RB, Phillipson GT, Wells JE. Sonographic appearances of the endometrium after termination of pregnancy in asymptomatic versus symptomatic women. J Ultrasound Med 2009; 28 (05) 579-586
- 11 Reeves MF, Fox MC, Lohr PA, Creinin MD. Endometrial thickness following medical abortion is not predictive of subsequent surgical intervention. Ultrasound Obstet Gynecol 2009; 34 (01) 104-109
- 12 Napolitano R, Ghosh M, Gillott DJ, Ojha K. Three-dimensional Doppler sonography in asymptomatic and symptomatic women after medical termination of pregnancy. J Ultrasound Med 2014; 33 (05) 847-852
- 13 Fujishima R, Kawasaki K, Moriuchi K, Shiro R, Yo Y, Matsumura N. Conservative management for retained products of conception in late pregnancy. Healthcare (Basel) 2023; 11 (02) 168
- 14 Kobayashi M, Nakagawa S, Kawanishi Y. et al. The RPOC long axis is a simple indicator for predicting the need of invasive strategies for secondary postpartum hemorrhage in either post-abortion or post-partum women: a retrospective case control study. BMC Pregnancy Childbirth 2021; 21 (01) 653
Address for correspondence
Publication History
Article published online:
18 June 2024
© 2024. Indographics. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 van den Bosch T, Daemen A, Van Schoubroeck D, Pochet N, De Moor B, Timmerman D. Occurrence and outcome of residual trophoblastic tissue: a prospective study. J Ultrasound Med 2008; 27 (03) 357-361
- 2 Epperly TD, Fogarty JP, Hodges SG. Efficacy of routine postpartum uterine exploration and manual sponge curettage. J Fam Pract 1989; 28 (02) 172-176
- 3 Sadan O, Golan A, Girtler O. et al. Role of sonography in the diagnosis of retained products of conception. J Ultrasound Med 2004; 23 (03) 371-374
- 4 Ustunyurt E, Kaymak O, Iskender C, Ustunyurt OB, Celik C, Danisman N. Role of transvaginal sonography in the diagnosis of retained products of conception. Arch Gynecol Obstet 2008; 277 (02) 151-154
- 5 Atri M, Rao A, Boylan C, Rasty G, Gerber D. Best predictors of grayscale ultrasound combined with color Doppler in the diagnosis of retained products of conception. J Clin Ultrasound 2011; 39 (03) 122-127
- 6 Alcázar JL, Baldonado C, Laparte C. The reliability of transvaginal ultrasonography to detect retained tissue after spontaneous first-trimester abortion, clinically thought to be complete. Ultrasound Obstet Gynecol 1995; 6 (02) 126-129
- 7 Kamaya A, Petrovitch I, Chen B, Frederick CE, Jeffrey RB. Retained products of conception: spectrum of color Doppler findings. J Ultrasound Med 2009; 28 (08) 1031-1041
- 8 Bar-Hava I, Aschkenazi S, Orvieto R. et al. Spectrum of normal intrauterine cavity sonographic findings after first-trimester abortion. J Ultrasound Med 2001; 20 (12) 1277-1281
- 9 Petrovitch I, Beatty M, Jeffrey RB, Heerema-McKenney A. Subinvolution of the placental site. J Ultrasound Med 2009; 28 (08) 1115-1119
- 10 McEwing RL, Anderson NG, Meates JB, Allen RB, Phillipson GT, Wells JE. Sonographic appearances of the endometrium after termination of pregnancy in asymptomatic versus symptomatic women. J Ultrasound Med 2009; 28 (05) 579-586
- 11 Reeves MF, Fox MC, Lohr PA, Creinin MD. Endometrial thickness following medical abortion is not predictive of subsequent surgical intervention. Ultrasound Obstet Gynecol 2009; 34 (01) 104-109
- 12 Napolitano R, Ghosh M, Gillott DJ, Ojha K. Three-dimensional Doppler sonography in asymptomatic and symptomatic women after medical termination of pregnancy. J Ultrasound Med 2014; 33 (05) 847-852
- 13 Fujishima R, Kawasaki K, Moriuchi K, Shiro R, Yo Y, Matsumura N. Conservative management for retained products of conception in late pregnancy. Healthcare (Basel) 2023; 11 (02) 168
- 14 Kobayashi M, Nakagawa S, Kawanishi Y. et al. The RPOC long axis is a simple indicator for predicting the need of invasive strategies for secondary postpartum hemorrhage in either post-abortion or post-partum women: a retrospective case control study. BMC Pregnancy Childbirth 2021; 21 (01) 653