

Subscribe to RSS
DOI: 10.1055/s-0044-1782692
Outcome of Secondary Interval Rheolytic Thrombectomy after Localized Intra-Arterial Catheter-Directed Thrombolysis through Power-Pulse Spray Technique in Cases of Partially Successful or Failed Primary Rheolytic Thrombectomy
Authors


Abstract
Objectives The aim of this study was to evaluate the safety and effectiveness of secondary interval AngioJet rheolytic thrombectomy after localized intra-arterial catheter-directed thrombolysis (CDT) through power-pulse spray (PPS) technique in partially successful or failed primary AngioJet rheolytic thrombectomy cases of acute and subacute peripheral artery thrombosis.
Materials and Methods This retrospective study included 12 acute (< 2 weeks) and subacute (2–4 weeks) peripheral arterial thrombosis patients who underwent primary thrombectomy alone without CDT and patients who received secondary thrombectomy after CDT through PPS at our institute between May 2022 and December 2022. Technical success, procedure-related complications (local and systemic), amputations, and 1-year patency were evaluated.
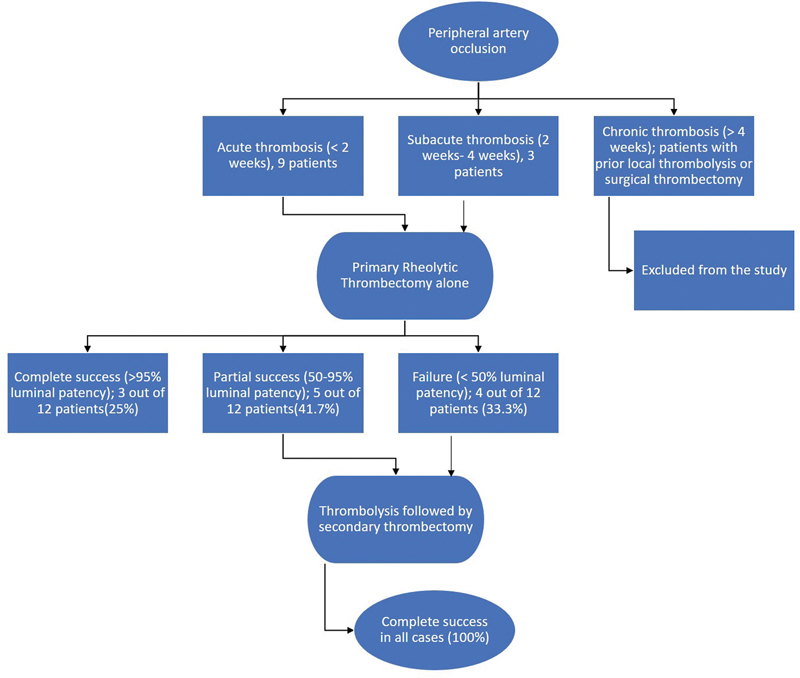
Results The angiographic success after primary thrombectomy was evaluated in 12 patients (9 acute and 3 subacute), and the results were categorized into three groups. Of 12 patients, complete success, partial success, and failure were noted in three (25%), five (41.7%), and four (33.3%) patients, respectively, after primary thrombectomy alone. Complete luminal patency was restored in all nine cases of partial success and failure in postprimary thrombectomy through adjunctive PPS thrombolysis and secondary thrombectomy. Technical and clinical success was achieved in all patients (100%). Transient hemoglobinuria was seen in five (41.7%) patients, and all had long-segment occlusion. At 1 year follow-up, no reocclusion, limb loss, or death was noted.
Conclusion Complete success after primary thrombectomy was more likely in the setting of short-segment occlusion and small-caliber arteries. In patients with partial success or failure after the primary thrombectomy alone, secondary thrombectomy may be performed after the adjuvant PPS thrombolysis to achieve complete recanalization.
Keywords
AngioJet rheolytic thrombectomy - Pharmacologic thrombolysis - power-pulse spray technique - Recombinant human tissue-type plasminogen activator - peripheral arterial occlusionIntroduction
The sudden and severe reduction in blood flow to the limb is known as acute limb ischemia, and it is imperative to reinstate perfusion as early as possible. A major cause of limb ischemia is thrombotic blockage of the peripheral arteries or surgical bypass grafts. The mainstay of care has been primarily surgical; nevertheless, limb salvage rates and surgical mortality, particularly in the presence of severe ischemia, have been subpar.[1] [2] Pharmacologic thrombolysis is now frequently used as an alternate therapy for peripheral artery thrombosis; however, its effectiveness is frequently constrained by protracted infusion times, hemorrhagic complications, and insufficient outcomes.[3] [4] Various percutaneous mechanical thrombectomy devices (aspiration, rheolysis, or mechanical rotation) have been created to achieve fast reperfusion in the occluded vessel and overcome the limitations of these surgical and pharmaceutical techniques.[5] These tools may reduce or altogether remove the need for thrombolytic drugs while being less intrusive than surgery.[6] AngioJet rheolytic thrombectomy system (Boston Scientific, Marlborough, Massachusetts, United States) uses high-velocity saline jets to macerate and evacuate thrombi. Clinical investigations have shown that AngioJet rheolytic thrombectomy is safe and effective for coronary applications, peripheral arterial thrombosis, deep vein thrombosis, and acute pulmonary embolism.[7] In most arterial thrombosis cases, rheolytic thrombectomy followed with or without thrombolysis gives satisfactory results. In contrast, adequate results are not achieved in a few cases, such as long-segment occlusion or high thrombus burden. In those cases, catheter-directed thrombolysis (CDT) using the power-pulse spray (PPS) technique followed by secondary thrombectomy can be performed to obtain a good outcome, which we have described in the present article.
Materials and Methods
Study Population
It is a retrospective study, so the institute's ethical committee has waived the need for de novo consent. All the patients had given consent for the procedures. Twelve patients with acute (< 2 weeks) and subacute (2–4 weeks) occlusion of the peripheral arteries who underwent rheolytic thrombectomy with or without thrombolysis between May 2022 and December 2022 were included. Patients with prior local thrombolysis, surgical thrombectomy, or chronic occlusion (> 4 weeks) were excluded from our study. A flowchart to show the patient selection and results is presented in [Fig. 1].
Procedure Protocol
The interventions were performed by interventional radiologists with more than 7 years of experience. All the patients underwent a preliminary Doppler study followed by computed tomography angiography for better delineation of the location and extent of the thrombus. Depending upon the case, a 6 Fr introducer sheath was inserted in the right or left common femoral artery, and a 5,000 IU bolus of heparin was given through the sheath at the start of the intervention, followed by an additional 1,000 IU at every hour of the procedure. The thrombosed arterial segment was negotiated using a 5F Multipurpose Angiographic catheter (Cook, United States) and hydrophilic 0.035/0.014-inch guidewires (Terumo, Japan). Next, the rheolytic thrombectomy catheter (Solent Omni/Solent Dista, Boston Scientific, Marlborough, Massachusetts, United States) was advanced into the thrombotic vessel over the hydrophilic guidewires with its tip in the normal vascular segment distal to the thrombotic segment. Thrombectomy alone was performed in multiple passes (2–4) using saline to extract the maximum volume of the thrombus, which hardly took 5 to 10 minutes. No further adjuvant thrombolytics were given if the lumen showed more than 95% luminal patency (complete success). In partial success (50–95% luminal patency) or unsuccessful (<50% luminal patency) cases after primary thrombectomy alone, we performed CDT through the PPS mode using reteplase (18 mg) followed by secondary thrombectomy using the same thrombectomy catheter. Thrombectomy time was kept within 10 minutes as per the manufacturer's guidelines. Reteplase is a recombinant human tissue-type plasminogen activator with peak response at 60 to 90 minutes. So, the clot is given a dwell time to lyse for 90 minutes of the PPS thrombolysis followed by secondary thrombectomy. For alteplase, it was 60 minutes. The patient was given intravenous heparin for 5 days and was discharged on dual antiplatelets (aspirin and clopidogrel). Balloon angioplasty with or without stenting was reserved for nonresponders to PPS thrombolysis and secondary thrombectomy. An algorithm for managing acute and subacute peripheral arterial occlusion is presented in [Fig. 2].

Definition of Outcome, Technical Success, Complications, and Follow-Up
The technical success was assessed based on angiographic images, hemodynamic and clinical parameters. The primary end-point of each intervention was angiographic success. More than 95% luminal patency was considered a complete success, while 50 to 95% and less than 50% luminal patency was considered partial success and failure, respectively.[8] Hemodynamic success was evaluated based on pre-and postprocedure pulse and Doppler examination. In addition to the demographics, periprocedural imaging, location of thrombus, and occlusion length were analyzed. Procedure-related complications (local and systemic), amputations, and 1-year patency were also evaluated.
Results
A detailed overview of each patient, the extent and location of the thrombus, and the effectiveness of primary thrombectomy alone and secondary thrombectomy are presented in [Table 1]. Of the 12 patients, 8 (66.7%) were female. Nine (75%) patients presented with acute thrombus (< 2 weeks), and 3 (25%) presented with subacute thrombus (between 2 and 4 weeks). We have categorized the results into three groups for simplification: complete success (> 95% luminal patency), partial success (50–95% luminal patency), and failure (< 50% luminal patency) after the primary thrombectomy alone. Complete success was seen in 3 (25%) of 12 patients after primary thrombectomy alone. These three patients presented with acute thrombosis of the distal brachial artery, popliteal artery, and distal superficial femoral artery with a length of the thrombotic segment of 4.0, 5.6, and 4.8 cm, respectively. Complete thrombus resolution was achieved after two to three passes of the thrombectomy catheter, and no thrombolysis was performed. Partial success was noted in 5 (41.7%) of 12 patients after primary thrombectomy alone. One patient had subacute thrombosis of the distal brachial artery, proximal ulnar artery, and proximal radial artery for a length of 15.0 cm and presented on day 25 of the onset of symptoms secondary to accidental needle injury to the brachial artery. We could achieve partial success after postprimary thrombectomy, so we performed the PPS technique using reteplase followed by secondary thrombectomy after 90 minutes to attain complete success ([Fig. 3]). In addition, two patients presented with subacute thrombosis of the superficial femoral artery (7.6 cm) and subclavian artery (5.0 cm). One presented with acute popliteal, anterior, and posterior tibial arteries thrombosis. One patient undergoing treatment for carcinoma stomach presented with acute thrombosis of her axillary artery (3.6 cm) and superficial femoral artery (7 cm). All these patients were offered PPS (reteplase) followed by secondary thrombectomy after a partially successful primary thrombectomy alone. Failure of thrombus evacuation (< 50% luminal patency) was seen in 4 (33.3%) of 12 patients after primary thrombectomy alone. One patient presented with acute occlusion of the axillary artery, brachial artery, proximal ulnar artery, and proximal radial artery for a length of 35 cm following trauma to the shoulder region. Primary thrombectomy was attempted but unsuccessful, so we performed PPS (reteplase) followed by secondary thrombectomy to attain complete success ([Fig. 4]). The second patient had acute thrombosis of the entire popliteal artery, anterior and posterior tibial arteries, with an additional short-segment (2.6 cm) discontinuous occlusion of the ipsilateral common femoral artery ([Fig. 5]). This patient was recently diagnosed with gallbladder carcinoma with liver metastasis. After the failure of the primary thrombectomy, we performed PPS (reteplase) followed by a secondary thrombectomy to attain complete success ([Fig. 6]). The third patient was diagnosed with dilated cardiomyopathy and had acute occlusion of the entire left lower limb arteries (superficial femoral artery, popliteal artery, anterior and posterior tibial arteries). The fourth patient presented with an acute thrombus of the superficial femoral and popliteal arteries (18 cm). Angiographic success was achieved in all 12 patients (100%). Five (41.7%) patients had transient hemoglobinuria, which resolved within 72 hours of the procedure. The basis for hemoglobinuria in these patients was probably because of long-segment occlusion or significant thrombus burden requiring more thrombectomy duration and so more hemolysis. None of the patients required postprocedure blood transfusions or infusion of thrombolytics. No distal embolization was noted in any patient during the procedure. All patients were discharged on a dual-antiplatelet regimen for 3 months or lifelong depending upon the cause of thrombotic occlusion, and physiotherapy was advised. At 3, 6, 9, and 12-month follow-ups, all these 12 patients had patent arteries on color Doppler without any evidence of reocclusion. Reperfusion edema was seen in all the patients resolved within 1 to 2 months of the procedure. No loss of limb or death was noted.
Abbreviations: AA, axillary artery; ATA, anterior tibial artery; BA, brachial artery; CFA, common femoral artery; PA, popliteal artery; PTA, posterior tibial artery; RA, radial artery; SA, subclavian artery; SFA, superficial femoral artery; UA, ulnar artery.




Discussion
Peripheral arterial thrombotic events are an emergency and necessitate immediate treatment. It can be managed through surgical thrombectomy, balloon angioplasty, localized or systemic thrombolysis, or catheter-based thrombectomy techniques (e.g., aspiration thrombectomy, rheolytic thrombectomy).[1] [2] [9] Balloon angioplasty is usually avoided in acute and subacute thrombotic cases because of the risk of distal embolic showers, especially during the endovascular treatment of long occlusions, and it is not always feasible to use a peripheral protection device (filter).[10] [11] [12] Thrombolysis is also associated with limitations, such as the risk of severe hemorrhagic complications, inability to lyse hard thrombus, long-segment block, and a need for a dedicated care unit.[11] Catheter thrombectomy devices have significantly progressed over the last decade, but literature support for their success is limited. AngioJet rheolytic thrombectomy system is commonly used to remove fresh thrombus and is considered safe and effective. Thrombectomy is done by introducing a pressurized high-velocity saline jet stream through the catheter distal tip. This creates a localized extreme low-pressure (powerful vacuum effect) via the Bernoulli principle and the Venturi effect, which macerates the thrombus. The fragmented thrombus is removed through the catheter's side holes or outflow lumen. Treatment with the device takes approximately 5 to 10 minutes. It also contains a special mechanical function termed “power-pulse spray,” which simultaneously fragments the thrombus and infuses thrombolytic agents directly into the clot, where it is most effective, saturating, and softening tough thrombus for easier removal.[13] [14] The PPS technique augments and combines the advantages and reduces the disadvantages of pharmacologic thrombolysis and rheolytic thrombectomy. AngioJet rheolytic thrombectomy is commonly used to remove clots in arteriovenous fistulas for dialysis access, massive acute pulmonary embolism, lower extremity deep vein thrombosis, peripheral arteries, coronary arteries, and coronary bypass grafts.[15] [16] [17] [18] [19] [20] [21] [22] It is an effective method; however, it is also associated with some complications, such as acute renal failure, hemoglobinuria, and the risk of distal embolism. Moreover, achieving an acceptable outcome with rheolytic thrombectomy alone is challenging in long-segment occlusion cases and needs adjunctive intra-arterial thrombolysis or stenting after the thrombectomy. To avoid rheolytic thrombectomy complications, we adequately hydrated the patient and used the device for not more than 10 minutes within the artery to avoid excessive hemolysis and renal dysfunction as per the manufacturer's guidelines. We give adjunctive local thrombolytics or use a peripheral filter protection device whenever feasible to avoid distal embolization.[23] Another possible adverse effect of rheolytic thrombectomy is fluid overload from the saline jets. Although the rheolytic thrombectomy system works in an isovolumetric fashion, there is still a risk of congestive heart failure.[18] Hence, the procedure should be performed cautiously in patients with underlying renal insufficiency and cardiac failure. Rheolytic thrombectomy alone can be curative in a few selected cases when the thrombus load is nonsignificant or small. Few studies have reported that rheolytic thrombectomy alone without pharmacologic thrombolysis is effective in removing thrombus in a short time.[7] Adjunctive balloon angioplasty, stenting, or thrombolysis is required when there is significant postrheolytic thrombectomy residual stenosis or thrombus burden. Stents are used to enmesh the residual intraluminal thrombus that could affect limb perfusion in the future or are used when there is significant residual stenosis after balloon angioplasty. But, these patients need lifelong oral antiplatelets to maintain the stent patency. A review of the rheolytic thrombectomy literature reveals that AngioJet therapy can substantially remove thrombus burden in a majority of patients and serve as monotherapy stand-alone therapy in 20 to 50% of cases. However, at least 50% will also require adjuvant pharmacologic thrombolysis.[17] [18] [24] Additionally, the likelihood of significant improvement after adjunctive CDT in cases of failed rheolytic thrombectomy is negligible.[18]
In our study, we performed CDT using the PPS technique followed by secondary thrombectomy in partial success or failure of partial thrombectomy alone, especially in cases with long-segment occlusion, large-volume, or significant thrombus burden to achieve complete recanalization of the occluded artery. In previous studies, the waiting period to lyse the thrombus was variable and short (10–30 minutes), which could be a reason for unsatisfactory results. However, we followed the 90-minute waiting period in all of our cases because the age of the thrombus cannot be appropriately assessed.[13] [14] Also, there is a possibility of the coexistence of older more organized thrombus with fresh thrombus. The main disadvantage of doing a secondary thrombectomy is the increase in the total duration of the procedure, which is around 1 to 2 hours, depending upon the type of thrombolytic drug (reteplase/alteplase) used, which might cause discomfort to the patient.
Additionally, there is an increased risk of AngioJet rheolytic thrombectomy complications secondary to excessive hemolysis, which can be avoided through adequate hydration of the patient and the use of the device for not more than 10 minutes within the artery. Also, the radiation exposure to the patient is increased. However, the benefits of doing a secondary thrombectomy are more encouraging. First, we achieved complete success with wall-to-wall patency in all cases where primary thrombectomy alone failed or showed partial success, especially in long-segment occlusion, large-volume, or significant thrombus burden. Second, it avoided the use of metallic stents, which reduced the financial burden on the patient and avoided the need to take lifelong oral antiplatelets to maintain the patency of these stents. Third, when paired with CDT using PPS, rheolytic thrombectomy provides benefits such as rapid revascularization, lowering the dose and duration of thrombolytic drug infusions, and reduced hemorrhagic complications. Our study has several limitations, such as its retrospective nature and a relatively small number of patients with different thrombus ages, locations, and characteristics. Therefore, the outcome of our study may be viewed as a precursory study demonstrating the role of secondary thrombectomy after CDT in partially successful or failed primary thrombectomy alone cases.
Conclusion
Primary thrombectomy alone can reinstate the flow in a thrombosed artery, especially in a short-segment occlusion of a small-to-medium-caliber artery. Partial success or failure after primary thrombectomy with or without local thrombolysis is common in cases of high thrombus volume, long-segment occlusion, or large caliber arteries. In patients with partial success or failure after the primary thrombectomy, secondary thrombectomy may be performed safely and successfully after the adjuvant PPS thrombolysis to restore the luminal patency completely. Well-designed multicenter prospective studies must corroborate these precursory findings in a large cohort of patients to reveal the significance and efficacy of this technique and our findings.
Conflict of Interest
None declared.
Ethical Approval Statement
Ethical approval was waived by the local ethics committee of our institute in view of the retrospective nature of the study and all the procedures being performed were part of the routine care.
Authors' Contribution
B.S., P.S., S.M., S.S, and R.P.M. conceptualized and prepared the original draft preparation. M.K.N., R.P., M.K.P., P.K., S.M.A, N.D.B, S.K.M., S.K.B., S.D., S.K.D.M., and A.P. reviewed and edited the manuscript. All the authors have agreed with the submitted manuscript.
-
References
- 1 Ouriel K, Shortell CK, DeWeese JA. et al. A comparison of thrombolytic therapy with operative revascularization in the initial treatment of acute peripheral arterial ischemia. J Vasc Surg 1994; 19 (06) 1021-1030
- 2 Ouriel K. Surgery versus thrombolytic therapy in the management of peripheral arterial occlusions. J Vasc Interv Radiol 1995; 6 (6 Pt 2, Suppl): 48S-54S
- 3 Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg 1994; 220 (03) 251-266 , discussion 266–268
- 4 Ouriel K, Veith FJ, Sasahara AA. Thrombolysis or Peripheral Arterial Surgery (TOPAS) Investigators. A comparison of recombinant urokinase with vascular surgery as initial treatment for acute arterial occlusion of the legs. N Engl J Med 1998; 338 (16) 1105-1111
- 5 Rilinger N, Görich J, Scharrer-Pamler R. et al. Short-term results with use of the Amplatz thrombectomy device in the treatment of acute lower limb occlusions. J Vasc Interv Radiol 1997; 8 (03) 343-348
- 6 Hynes BG, Margey RJ, Ruggiero II N, Kiernan TJ, Rosenfield K, Jaff MR. Endovascular management of acute limb ischemia. Ann Vasc Surg 2012; 26 (01) 110-124
- 7 Ansel GM, George BS, Botti CF. et al. Rheolytic thrombectomy in the management of limb ischemia: 30-day results from a multicenter registry. J Endovasc Ther 2002; 9 (04) 395-402
- 8 Kasirajan K, Ouriel K. Management of acute lower extremity ischemia: treatment strategies and outcome. Curr Interv Cardiol Rep 2000; 2 (02) 119-129
- 9 Tsetis D, Uberoi R. Quality improvement guidelines for endovascular treatment of iliac artery occlusive disease. Cardiovasc Intervent Radiol 2008; 31 (02) 238-245
- 10 Gardiner Jr GA, Meyerovitz MF, Stokes KR, Clouse ME, Harrington DP, Bettmann MA. Complications of transluminal angioplasty. Radiology 1986; 159 (01) 201-208
- 11 Karnabatidis D, Spiliopoulos S, Tsetis D, Siablis D. Quality improvement guidelines for percutaneous catheter-directed intra-arterial thrombolysis and mechanical thrombectomy for acute lower-limb ischemia. Cardiovasc Intervent Radiol 2011; 34 (06) 1123-1136
- 12 Spiliopoulos S, Katsanos K, Fragkos G, Karnabatidis D, Siablis D. Treatment of infrainguinal thromboembolic complications during peripheral endovascular procedures with AngioJet rheolytic thrombectomy, intraoperative thrombolysis, and selective stenting. J Vasc Surg 2012; 56 (05) 1308-1316
- 13 Shammas NW, Dippel EJ, Shammas G, Gayton L, Coiner D, Jerin M. Dethrombosis of the lower extremity arteries using the power-pulse spray technique in patients with recent onset thrombotic occlusions: results of the DETHROMBOSIS Registry. J Endovasc Ther 2008; 15 (05) 570-579
- 14 Allie DE, Hebert CJ, Lirtzman MD. et al. Novel simultaneous combination chemical thrombolysis/rheolytic thrombectomy therapy for acute critical limb ischemia: the power-pulse spray technique. Catheter Cardiovasc Interv 2004; 63 (04) 512-522
- 15 Lee HY, Kim CS, Han KD, Kim MJ. Comparison of the clinical outcomes between angiojet pharmacomechanical thrombectomy and hybrid surgical thrombectomy for thrombotic occlusion of hemodialysis access. Vasc Spec Int 2020; 36 (04) 241-247
- 16 Margheri M, Falai M, Vittori G. et al. Safety and efficacy of the AngioJet in patients with acute myocardial infarction: results from the Florence Appraisal Study of Rheolytic Thrombectomy (FAST). J Invasive Cardiol 2006; 18 (10) 481-486
- 17 Silva JA, Ramee SR, Collins TJ. et al. Rheolytic thrombectomy in the treatment of acute limb-threatening ischemia: immediate results and six-month follow-up of the multicenter AngioJet registry. Possis Peripheral AngioJet Study AngioJet Investigators. Cathet Cardiovasc Diagn 1998; 45 (04) 386-393
- 18 Kasirajan K, Gray B, Beavers FP. et al. Rheolytic thrombectomy in the management of acute and subacute limb-threatening ischemia. J Vasc Interv Radiol 2001; 12 (04) 413-421
- 19 Villalba L, Nguyen T, Feitosa Jr RL, Gunanayagam P, Anning N, Dwight K. Single-session catheter-directed lysis using adjunctive power-pulse spray with AngioJet for the treatment of acute massive and submassive pulmonary embolism. J Vasc Surg 2019; 70 (06) 1920-1926
- 20 Mundhada RG, Rewatkar AD, Mundhada AR, Rewatkar AA, Chandak NN. Pharmacomechanical thrombectomy for acute limb threatening lower extremity arterial thrombosis secondary to COVID-19. J Clin Interv Radiol ISVIR 2022; 6: 170-176
- 21 Zeni Jr PT, Blank BG, Peeler DW. Use of rheolytic thrombectomy in treatment of acute massive pulmonary embolism. J Vasc Interv Radiol 2003; 14 (12) 1511-1515
- 22 Garcia MJ, Lookstein R, Malhotra R. et al. Endovascular management of deep vein thrombosis with rheolytic thrombectomy: final report of the prospective multicenter PEARL (Peripheral Use of AngioJet Rheolytic Thrombectomy with a Variety of Catheter Lengths) Registry. J Vasc Interv Radiol 2015; 26 (06) 777-785 , quiz 786
- 23 Müller-Hülsbeck S, Kalinowski M, Heller M, Wagner HJ. Rheolytic hydrodynamic thrombectomy for percutaneous treatment of acutely occluded infra-aortic native arteries and bypass grafts: midterm follow-up results. Invest Radiol 2000; 35 (02) 131-140
- 24 Reekers JA, Kromhout JG, Spithoven HG, Jacobs MJ, Mali WM, Schultz-Kool LJ. Arterial thrombosis below the inguinal ligament: percutaneous treatment with a thrombosuction catheter. Radiology 1996; 198 (01) 49-53
Address for correspondence
Publication History
Article published online:
19 April 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Ouriel K, Shortell CK, DeWeese JA. et al. A comparison of thrombolytic therapy with operative revascularization in the initial treatment of acute peripheral arterial ischemia. J Vasc Surg 1994; 19 (06) 1021-1030
- 2 Ouriel K. Surgery versus thrombolytic therapy in the management of peripheral arterial occlusions. J Vasc Interv Radiol 1995; 6 (6 Pt 2, Suppl): 48S-54S
- 3 Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann Surg 1994; 220 (03) 251-266 , discussion 266–268
- 4 Ouriel K, Veith FJ, Sasahara AA. Thrombolysis or Peripheral Arterial Surgery (TOPAS) Investigators. A comparison of recombinant urokinase with vascular surgery as initial treatment for acute arterial occlusion of the legs. N Engl J Med 1998; 338 (16) 1105-1111
- 5 Rilinger N, Görich J, Scharrer-Pamler R. et al. Short-term results with use of the Amplatz thrombectomy device in the treatment of acute lower limb occlusions. J Vasc Interv Radiol 1997; 8 (03) 343-348
- 6 Hynes BG, Margey RJ, Ruggiero II N, Kiernan TJ, Rosenfield K, Jaff MR. Endovascular management of acute limb ischemia. Ann Vasc Surg 2012; 26 (01) 110-124
- 7 Ansel GM, George BS, Botti CF. et al. Rheolytic thrombectomy in the management of limb ischemia: 30-day results from a multicenter registry. J Endovasc Ther 2002; 9 (04) 395-402
- 8 Kasirajan K, Ouriel K. Management of acute lower extremity ischemia: treatment strategies and outcome. Curr Interv Cardiol Rep 2000; 2 (02) 119-129
- 9 Tsetis D, Uberoi R. Quality improvement guidelines for endovascular treatment of iliac artery occlusive disease. Cardiovasc Intervent Radiol 2008; 31 (02) 238-245
- 10 Gardiner Jr GA, Meyerovitz MF, Stokes KR, Clouse ME, Harrington DP, Bettmann MA. Complications of transluminal angioplasty. Radiology 1986; 159 (01) 201-208
- 11 Karnabatidis D, Spiliopoulos S, Tsetis D, Siablis D. Quality improvement guidelines for percutaneous catheter-directed intra-arterial thrombolysis and mechanical thrombectomy for acute lower-limb ischemia. Cardiovasc Intervent Radiol 2011; 34 (06) 1123-1136
- 12 Spiliopoulos S, Katsanos K, Fragkos G, Karnabatidis D, Siablis D. Treatment of infrainguinal thromboembolic complications during peripheral endovascular procedures with AngioJet rheolytic thrombectomy, intraoperative thrombolysis, and selective stenting. J Vasc Surg 2012; 56 (05) 1308-1316
- 13 Shammas NW, Dippel EJ, Shammas G, Gayton L, Coiner D, Jerin M. Dethrombosis of the lower extremity arteries using the power-pulse spray technique in patients with recent onset thrombotic occlusions: results of the DETHROMBOSIS Registry. J Endovasc Ther 2008; 15 (05) 570-579
- 14 Allie DE, Hebert CJ, Lirtzman MD. et al. Novel simultaneous combination chemical thrombolysis/rheolytic thrombectomy therapy for acute critical limb ischemia: the power-pulse spray technique. Catheter Cardiovasc Interv 2004; 63 (04) 512-522
- 15 Lee HY, Kim CS, Han KD, Kim MJ. Comparison of the clinical outcomes between angiojet pharmacomechanical thrombectomy and hybrid surgical thrombectomy for thrombotic occlusion of hemodialysis access. Vasc Spec Int 2020; 36 (04) 241-247
- 16 Margheri M, Falai M, Vittori G. et al. Safety and efficacy of the AngioJet in patients with acute myocardial infarction: results from the Florence Appraisal Study of Rheolytic Thrombectomy (FAST). J Invasive Cardiol 2006; 18 (10) 481-486
- 17 Silva JA, Ramee SR, Collins TJ. et al. Rheolytic thrombectomy in the treatment of acute limb-threatening ischemia: immediate results and six-month follow-up of the multicenter AngioJet registry. Possis Peripheral AngioJet Study AngioJet Investigators. Cathet Cardiovasc Diagn 1998; 45 (04) 386-393
- 18 Kasirajan K, Gray B, Beavers FP. et al. Rheolytic thrombectomy in the management of acute and subacute limb-threatening ischemia. J Vasc Interv Radiol 2001; 12 (04) 413-421
- 19 Villalba L, Nguyen T, Feitosa Jr RL, Gunanayagam P, Anning N, Dwight K. Single-session catheter-directed lysis using adjunctive power-pulse spray with AngioJet for the treatment of acute massive and submassive pulmonary embolism. J Vasc Surg 2019; 70 (06) 1920-1926
- 20 Mundhada RG, Rewatkar AD, Mundhada AR, Rewatkar AA, Chandak NN. Pharmacomechanical thrombectomy for acute limb threatening lower extremity arterial thrombosis secondary to COVID-19. J Clin Interv Radiol ISVIR 2022; 6: 170-176
- 21 Zeni Jr PT, Blank BG, Peeler DW. Use of rheolytic thrombectomy in treatment of acute massive pulmonary embolism. J Vasc Interv Radiol 2003; 14 (12) 1511-1515
- 22 Garcia MJ, Lookstein R, Malhotra R. et al. Endovascular management of deep vein thrombosis with rheolytic thrombectomy: final report of the prospective multicenter PEARL (Peripheral Use of AngioJet Rheolytic Thrombectomy with a Variety of Catheter Lengths) Registry. J Vasc Interv Radiol 2015; 26 (06) 777-785 , quiz 786
- 23 Müller-Hülsbeck S, Kalinowski M, Heller M, Wagner HJ. Rheolytic hydrodynamic thrombectomy for percutaneous treatment of acutely occluded infra-aortic native arteries and bypass grafts: midterm follow-up results. Invest Radiol 2000; 35 (02) 131-140
- 24 Reekers JA, Kromhout JG, Spithoven HG, Jacobs MJ, Mali WM, Schultz-Kool LJ. Arterial thrombosis below the inguinal ligament: percutaneous treatment with a thrombosuction catheter. Radiology 1996; 198 (01) 49-53