

Subscribe to RSS
DOI: 10.1055/s-0044-1779709
Risk Factor Analysis for 30-day Mortality After Surgery for Infective Endocarditis
Authors
Abstract
Background Infective endocarditis (IE) remains a challenging disease associated with high mortality. Several scores have been suggested to assess surgical risk. None was sufficiently adequate. We therefore analyzed risk factors for 30-day mortality.
Methods A total of 438 consecutive patients had surgery for IE in our department between 2002 and 2020. Patients were divided into two groups, one consisting of 30-day survivors (362 patients; 82.6%) and one of nonsurvivors (76 patients; 17.4%). Logistic regression analysis on pre- and intraoperative risk factors was performed and the groups were compared by univariable analyses.
Results Patients in mortality group were older (69 [58, 77] vs. 63 [50, 72] years; p < 0.001), EuroSCORE II was higher (24.5 [12.1, 49.0] vs. 8.95 [3.7, 21.2]; p < 0.001) and there were more females. More frequently left ventricular function (below 30%), preoperative acute renal insufficiency, chronic dialysis, insulin-dependent diabetes mellitus, NYHA-class IV (New York Heart Association heart failure class IV), and cardiogenic shock occurred. Patients in the mortality group were often intensive care unit patients (40.8 vs. 22.4%; p < 0.001) or had a preoperative stroke (26.3 vs. 16.0%; p = 0.033). In the nonsurvivor group Staphylococcus aureus was prevalent. Streptococcus viridans was common in the survivor group as was isolated aortic valve endocarditis (32.9 vs. 17.1%; p = 0.006). Prosthetic valve endocarditis (PVE) and abscesses occurred more often in nonsurvivors. In the logistic regression analysis, female gender, chronic dialysis, cardiogenic shock, and NYHA IV and from intraoperative variables PVE, cardiopulmonary bypass time, and mitral valve surgery were the strongest predictors for 30-day mortality.
Conclusion This study indeed clearly indicates that significant risk factors for 30-day mortality cannot be changed. Nevertheless, they should be taken into account for preoperative counselling, and they will alert the surgical team for an even more careful management.
Introduction
Infective endocarditis (IE) remains one of the most challenging diseases of modern times. It is associated with high mortality and morbidity, although diagnostic and surgical skills as well as antibiotic pretreatment have substantially improved.[1]
Every study contributes to the knowledge of this frequently lethal disease, but one of the challenging questions remains which patients are likely to survive and how survival in general may be increased. At the current time between 52.9 and 58.9% of patients with IE have a theoretical indication for surgery. Yet, only in about 40% of the cases valve surgery is actually performed.[2] Several scores such as EuroScore I and II, PALSUSE, Risk-E, Costa, De Feo-Cotrufo, AEPEI, STS-risk, STS-IE, APORTEI, and ICE-PCS have been evaluated to approach the question of the operability of a given patient, yet the utility of these scores remains questionable.[3]
Although 30-day mortality seems an old tool for the evaluation of surgical quality and it was even suggested to abandon this concept, as mortality seems to increase after 30-days, we decided to use it nonetheless as none of the mentioned scores is sufficiently conclusive. To evaluate its justification for this study, all-hospital death was also included in the analysis. Thus, a retrospective analysis of our endocarditis registry was performed to evaluate risk factors for 30-day mortality and henceforth to approach the question of operability and benefit of surgical intervention for these critically ill patients.
Methods
Patients
Between the years 2002 and 2020 altogether 438 consecutive patients had surgery for IE at our department. All patients operated on IE were enrolled in our endocarditis registry. Patients treated with medication only were excluded. Data were retrospectively collected in a specially created database and retrieved from medical records. IE was located at least on one valve or valve prosthesis. This diagnosis was ensured intraoperatively and microbiologically. In this retrospective cohort study risk factors for 30-day mortality were analyzed and a comprehensive risk factor analysis performed. Patients were subsequently divided into two groups. One group consisted of 30-day survivors (362 patients; 82.6%) and one of nonsurvivors (76 patients; 17.4%). The local institutional ethics committee approved the study protocol and authorized its conduct (file number D 458/20). Individual patient's written informed consent for study participation was obtained.
Patient Management
Antibiotic treatment was usually started as soon as endocarditis was plausible according to the modified Duke criteria. All patients had blood cultures taken to identify organisms according to species and sensitivities. The location and the size of vegetation, presence of valve insufficiencies or abscesses, and left ventricular ejection fraction (LVEF) were analyzed using a transthoracic or transesophageal echocardiogram. Coronary angiography and additional computed tomography (CT) including cerebral CT, thoracic CT, and whole-body CT scans were performed in high-risk or redo patients. Patients were referred to our department and scheduled for near-term surgery as soon as surgical treatment was indicated. Intravenous antibiotic treatment regime was maintained for 4 to 6 weeks postoperatively, if diagnosis was intraoperatively reaffirmed. All patients with neurological complications had an evaluation of neurological status by a consultant neurologist and a CT scan of the brain to estimate risks of bleeding and prognoses if patients were intubated.
Surgical Technique
All patients had a routine general anesthesia. As standard access median sternotomy was performed. Few patients with mitral valve endocarditis had minimally invasive anterolateral thoracotomy. Extracorporeal circulation with heart–lung machine with mild hypothermia (34°C) was installed. Usually, arterial cannulation of the aorta and a single venous cannulation of the right atrial appendage was installed. Double cannulation of superior and inferior vena cava was used if tricuspid valve or mitral valve were operated on. This was followed by cross-clamping. Antegrade and retrograde application of cold blood cardioplegic solution was used to achieve myocardial protection. The surgical method was depending on macroscopic degree of valve destructions and clinical judgement of the surgical team based on universally applicable guidelines. Depending on the individual patient's situation and the intracardiac findings, additional procedures were performed. Choice of prothesis (biological or mechanical) was left to patient's preference.
Data Collection
Data collection was prospective in our internal endocarditis registry, yet evaluation of 30-day mortality was performed in a retrospective manner. Pre-, intra-, and postoperative variables were taken from medical records. All data collected were documented in anonymized form in an Excel spreadsheet.
Statistical Analyses
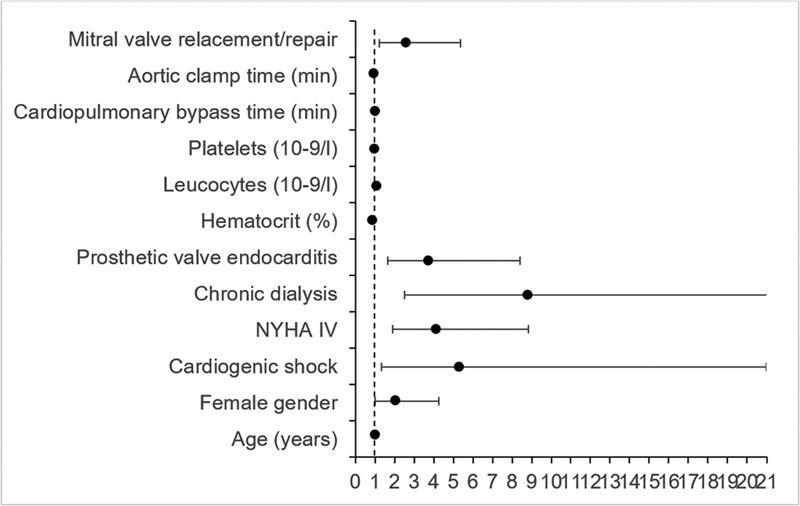
Statistical analysis was done using the IBM SPSS Statistics software (version 26.0). Normality of continuous variables was assessed by Lilliefors test/Kolmogorov–Smirnov test. Values of continuous data are presented as median with interquartile range or range as appropriate. Categorical variables are displayed as frequency distributions (n) and simple percentages (%). Categorical variables of the groups were compared by χ2 and the Fisher's exact test as appropriate. Normally distributed quantitative variables were compared by t-test and Mann–Whitney U test was used for non-normally distributed variables. Statistical significance was considered when p ≤ 0.05. Clinically relevant variables with at least eight events and less than 5.5% missing values except for LVEF (8.9% missing values) associated with 30-day mortality at p <0.1 were included into multivariable logistic regression analysis. Further variable selection was based on clinical relevance and stepwise selection. Model 1 included preoperative parameters, model 2 included intraoperative parameters, and model 3 combined pre- and intraoperative variables with a p-value ≤ 0.1 in models 1and 2, with a goodness of fit, described by Cox's and Snell's R-squared of 0.235, 0.123, and 0.283, respectively. The results of models 1 and 2 are shown as [Supplementary Tables S1] and [S2] (available in the online version). Model 1 is visualised in [Fig. 1], Model 2 is shown in [Fig. 2]. The results of model 3 are presented in [Table 6] and graphically demonstrated in [Fig. 3].


Results
Out of our endocarditis registry all 438 patients having had surgery due to IE were retrieved. They were divided into two groups: the group of survivors (n = 362) and the group of nonsurvivors (n = 76).
Patients' Baseline Characteristics and Clinical Presentation
Patients in the nonsurvivor group were significantly older (69 vs. 63 years; p < 0.001), had a higher proportion of female patients (p = 0.006), and a higher logistic EuroSCORE (45.2 vs. 21.3; p < 0.001) and EuroSCORE II (24.52 vs. 8.95; p < 0.001). In the study group reduced left ventricular function below 30% (22.2 vs. 7.3%; p < 0.001) was significantly more frequent as was diabetes type II (28.8 vs. 18.2%; p = 0.034) and insulin-dependent diabetes (21.1 vs. 9.7%; p = 0.005).
Also, significantly different were preoperative acute and chronic renal insufficiency and chronic dialysis and NYHA-class IV (New York Heart Association heart failure class IV). Patients who were not likely to survive were in a worse preoperative state: they were often transferred from intensive care unit (ICU; 40.8 vs. 22.4%; p < 0.001) and had more often a cardiogenic shock (14.5 vs. 2.8%; p < 0.001), were in a more critical preoperative state (32.9 vs. 16.3%; p < 0.001), and had more often emergency surgery (32.9 vs. 19.6%; p = 0.011). They had more likely a preoperative stroke (26.3 vs.16.0%; p = 0.033). Yet, preoperative embolization either cerebral or into other organs did not differ significantly. Patients of the 30-day mortality group had a shorter time from diagnosis to surgery (5 [1, 12] vs. 8 [3, 18] days) and more often a time period from diagnosis to surgery ≤1 day. Nonsurvivors had a median of 6 days of fever prior to surgery compared with 5 days in the group of 30-day survivors (p = 0.05). No differences were noted concerning commencement of antibiotic treatment. Differences could be seen concerning pathogen spectrum. Staphylococcus aureus was the most common proven germ and more frequent in the 30-day mortality group (p = 0.032), whereas viridans streptococci or gram-positive streptococci were mainly present in the survivor group (p = 0.003 and 0.010, respectively). No differences concerning any other germ was noted. Especially methicillin-resistant S. aureus was not significantly higher in any group. Affected valves were mainly the aortic valve (highly significant for the survivor group) and the mitral valve (dominant in the nonsurviving group), but the latter without reaching significance. Isolated prosthesis endocarditis occurred slightly more frequently in the 30-day nonsurvivor group (43.4 vs. 32.0%, p = 0.057). Isolated at least moderate valve insufficiency of the aortic valve was more common in the survivor group (28.2 vs. 11.8%, p = 0.003). Abscesses occurred more often in the nonsurvivor group (47.4 vs. 23.5%, p < 0.001).
In the 30-day nonsurvivor group preoperative laboratory parameters were significantly lower for hemoglobin, hematocrit, platelets, and glomerular filtration rate (GFR), whereas C-reactive protein, potassium, creatinine, leukocytes, urea, CK/CK-MB (creatine kinase/myocardial band), bilirubin, and international normalized ratio (INR) were significantly higher. An overview on demographic and preoperative clinical characteristics of the study population is outlined in [Tables 1], [2] and [3].
Abbreviations: CABG, coronary artery bypass grafting; COPD, chronic obstructive pulmonary disease; DES, drug eluting stent; EuroSCORE, European System for Cardiac Operative Risk Evaluation; IDDM, insulin-dependent diabetes mellitus; LVEF, left ventricular ejection fraction; NYHA IV, New York Heart Association heart failure stage IV; PCI, percutaneous coronary intervention; TAVI, transcatheter aortic valve implantation.
Abbreviations: AV, aortic valve; CPR, cardiopulmonary resuscitation; HACEK, Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella; MRSA, methicillin-resistant Staphylococcus aureus; MV, mitral valve; NYHA IV, New York Heart Association heart failure stage IV; TIA, transient ischemic attack; TV, tricuspid valve.
Abbreviations: ALT/GPT, alanine aminotransferase/glutamic pyruvic transaminase; CK/CK-MB, creatine kinase/myocardial band; CRP, C-reactive protein; GFR, glomerular filtration rate; INR, international normalized ratio.
Operative Data
Length of surgery differed significantly between the groups (p = 0.001) as did cardiopulmonary bypass time (p < 0.001). Cross-clamp time tended to be longer in the nonsurvivor group. The nonsurvivors received on average more red blood cell units, fresh-frozen plasma units (p < 0.001), and a higher number of platelet units (p < 0.001). The survivor group received more often biological aortic valve replacements (48.1 vs. 37.3%; p = 0.09). The nonsurvivor group had more often biological composite aortic root replacements (30.7 vs. 16.3%; p = 0.004). Mitral valve surgery was more common in the 30-day mortality group but did not reach significance nor did tricuspid valve surgery, which was more common in the survivor group. Valve surgery with pacemaker implantation was more common in the nonsurvivor group, yet not significant. Operative data are summarized in [Table 4].
Abbreviations: ACB, aortocoronary bypass; bio, biological; mech, mechanical.
Postoperative Data
Postoperative laboratory and clinical data and outcomes are summarized in [Table 5]. Differences in early and late postoperative complications were noticeable for both groups. Especially, laboratory parameters were significantly different after surgery. Hemoglobin and hematocrit (lowest values) after surgery were significantly different. Urea, lactate, sodium, potassium, creatinine, GFR, CK/CK-MB, aspartate transferase, alanine aminotransferase, bilirubin, leukocytes, and platelets differed significantly between the two groups. Not significantly different were C-reactive protein and INR until first postoperative day.
Abbreviations: AKI, acute kidney injury; ALT/GPT, alanine aminotransferase/glutamic pyruvic transaminase; AST/GOT, aspartate transferase/glutamic oxaloacetic transaminase; CPR, cardiopulmonary resuscitation; ICU, intensive care unit; INR, international normalized ratio; KDIGO, Kidney Disease: Improving Global Outcomes; MOF, multiple organ failure; postop, postoperative; preop, preoperative.
Moreover, acute kidney injury based on KDIGO (Kidney Disease: Improving Global Outcomes) stages was significantly different (60.6% nonsurvivors vs. 23.3% survivors; p < 0.001). Stage 3 occurred mainly in the 30-day mortality group (80 vs. 43.2%; p < 0.001). New onset on hemodialysis was more common in the nonsurvivor group (52.4 vs. 8.5%; p < 0.001). The reexploration rates due to profuse postoperative bleeding or cardiac tamponade within 3 days postoperative were higher in the 30-day mortality group (22.1 vs. 10.2%; p = 0.006). Twenty-four-hour drainage loss had the tendency to be more in the 30-day mortality group (600 [300–1,100] vs. 800 mL [450–1,350]; p < 0.09). Also, 24 and 48-hour numbers of packed red blood cells, fresh-frozen plasma units, as well as platelet units showed highly significant differences (p < 0.001 for all). Ventilation time was significantly longer in the nonsurvivor group (41 [19, 116] vs. 14 [8, 36] hours; p < 0.001). Reintubation was also significantly higher (21.9 vs. 10.2%; p = 0.008) and rate of bronchopulmonary infection (survivor 7.5 vs. nonsurvivor 24.6%, p < 0.001). Neither tracheostomy nor ICU stay in days was significantly different. Postoperative delirium did not show a significance. More nonsurviving patients developed a sepsis (57.1 vs. 4.4%; p < 0.001) and had to be resuscitated (18.8 vs. 3.0%; p < 0.001).
There were highly significant differences concerning 7-day mortality, which was 67.1% for the nonsurvivor group and due to study design 0% for the survivors p < 0.001). In-hospital mortality was 1.4% for the 30-day survivors and 85.5% for the nonsurvivors (p < 0.001).
In the final logistic regression analysis female gender (odds ratio [OR]: 2.070; 95% confidence interval [CI]: 1.008–4.249), chronic dialysis (OR: 8.797; 95% CI: 2.511–30.812; p < 0.001), cardiogenic shock (OR: 5.325; 95% CI: 1.351–20.998; p = 0.017), and NYHA class IV (OR: 4.110; 95% CI: 1.913–8.829; p < 0.001) were the strongest predictors for 30-day mortality. From the intraoperative variables prosthetic valve endocarditis (OR: 3.724; 95% CI: 1.651–8.401; p = 0.002), longer cardiopulmonary bypass time (OR: 1.030; 95% CI: 1.016–1.044; p < 0.001), and mitral valve replacement or repair (OR: 2.571; 95% CI: 1.234–5.356; p = 0.012) were risk factors for 30-day mortality.
Taking the laboratory parameters into account high hematocrit had rather a protective effect (OR: 0.879; 95% CI: 0.819–0.945; p < 0.001), as had high platelet count (OR: 0.995; 95% CI: 0.991–0.998; p = 0.003), whereas high leukocytes were a risk factor for 30-day mortality (OR: 1.095; 95% CI: 1.021–1.175; p = 0.011). See [Table 6] for logistic regression analysis.
Abbreviation: NYHA IV, New York Heart Association heart failure stage IV.
Discussion
IE is one of the most challenging surgical diseases.[4] Although treatment options have improved, disease burden is generally increasing.[5] [6] Especially, since the modification of the endocarditis prophylaxis guidelines in 2002 patient numbers are continually rising.[7] Given scarce resources, it is eminent to evaluate which patients benefit mostly from early surgery and how survival might generally be improved.
Patients baseline characteristics differed significantly. As already known from other studies, patients in the nonsurvivor group were significantly older, yet age with an OR of 1.029 was not the strongest predictor for 30-day mortality looking at logistic regression analysis. Female gender has been shown to be an independent predictor for 30-day mortality in our previous study.[8] EuroScore II was significantly higher in our study group and was a good indicator for 30-day mortality. The EuroScore II in general is controversially discussed. While some researchers think it underestimates the mortality in cardiac surgery,[9] [10] others believe it to be an appropriate tool for estimating perioperative risks even in IE patients.[11] Our study supports this assessment.
As previously reported reduced left ventricular function below 30% is an exceptionally high-risk factor for perioperative death. In our study group significant more patients of the 30-day mortality group had reduced left ventricular functions. It becomes more and more obvious that chronic dialysis has an impact on left ventricular function and cardiovascular events.[12] The exact pathways are not yet fully understood. Not surprisingly in our 30-day mortality group more patients had a preoperative acute renal insufficiency and chronic dialysis. Taking our logistic regression analysis into account, chronic dialysis is the most eminent risk factor for 30-day mortality. It is followed by cardiogenic shock, which is defined by low blood pressure caused by low cardiac output. NYHA class IV as the highest clinical parameter of heart failure was a strong predictor for 30-day mortality in our study as well.
Diabetes type II and insulin-depending diabetes were more frequent in the 30-day mortality group. Obesity and diabetes are widely known as risk factor for mortality in cardiac surgery.[13]
Surgical timing is not yet fully understood and thus a question of debate. The American College of Cardiology/American Heart Association endocarditis guidelines and the European Society for Cardiology endocarditis guidelines recommend specific parameters to be met for performing early valve surgery.[14] [15] The time from diagnosis to surgery was significantly shorter in the nonsurvivor group. Also, significantly more patients had surgeries in less than 1 day from diagnosis in 30-day mortality group. The decision to perform early surgery is challenging, as there are numerable associated complications and the patient's response to antibiotic therapy is not predictable.[16] Bearing this in mind, it is also reasonable to understand that patients of the nonsurvivor group were in a worse preoperative state: they were often transferred from ICU and had more often emergency surgery. Thus, early surgery was in our analysis rather a necessity than a choice. In our study group, we could not demonstrate a survival benefit for early surgery in contrast to other groups.[16]
There were huge differences concerning pathogen spectrum. Staphylococcus aureus, which is deemed to be a predictor of late death and is discussed to increase risk of in-hospital mortality in the presence of decreased left ventricular function,[17] was significantly more common in the nonsurvivor group. Methicillin-resistant S. aureus, however, was not significantly higher. Streptococci (either viridans or gram-positive) were more common in the survivor group. In other centers Streptococci are the most common (up to 50%); we could not verify this finding.
Significantly more often affected was the aortic valve alone in the survivor group, whereas prosthetic valve endocarditis occurred only marginally more frequently in the nonsurvivor group. Yet, prosthetic valve endocarditis was an independent risk factor for 30-day mortality. Taking preoperative laboratory parameters into account higher hematocrit and higher platelet counts seem to have a protective effect against mortality. Higher leukocytes and C-reactive protein values seem to be an expression of worse clinical status. In combination with the higher appearance of S. aureus, this might hint that conventional antibiotic therapy is not sufficient in these critically ill patients and a therapeutic attempt with Exebacase, an antistaphylococcal lysin, could be a good choice for this group.[18]
According to the higher complexity of surgeries performed in the 30-day mortality group and the higher degree of destruction around the concerned valves length of surgery differed significantly between the groups as did cardiopulmonary bypass time. In logistic regression analysis cardiopulmonary bypass time was not a strong predictor for 30-day mortality. Yet, prosthesis endocarditis and mitral valve reconstruction or replacement could be determined as risk factors for 30-day mortality, thus supporting the hypothesis that more complex surgeries account for higher rates of 30-day mortality. Nonsurvivors received on average more red blood cell units, fresh-frozen plasma units, and a higher number of platelet units probably as a necessity due to their worse preoperative state. Most likely every blood transfusion itself is a risk factor for mortality as other studies also suggest.[19]
Postoperative data support the hypothesis that nonsurvivors were in a worse pre- and postoperative state. As retention values and transaminases were eminently higher, organ damage was ubiquitous more present in the 30-day mortality group. Reinforcing this impression were anytime higher lactate values. Nonrecovering from acute kidney injury is known to be associated with higher lactate levels.[20] In line with this, KDIGO stage 3 occurred mainly in the 30-day mortality group. Other organ damages like higher ventilation time, bronchopulmonary infection, cardiopulmonary resuscitation, myocardial infarction, and sepsis were much more likely to occur in the 30-day mortality group. Thus, helping to explain the reasons for hospital mortality, which were mainly multiorgan failure, cardiac death, and sepsis.
There were highly significant differences concerning 7-day mortality for the nonsurvivor group, which was 67.1% already. Thus, leading to the assumption that most factors leading to death were already determined at this early stage. In-hospital mortality rates vary from 15 to 30%.[16] [21] In our study in-hospital mortality was 16.1% for all patients. This is comparable to other centers. In summary, this study indeed clearly indicates that significant risk factors for 30-day mortality cannot be changed. Nevertheless, they should be taken into account for preoperative counselling, and they will alert the surgical team for an even more careful management.
Limitations
Our results should be interpreted with caution and viewed as hypothesis generated in light of the retrospective study design from a single center. While treatment was performed according to guideline recommendations, it was still based on clinical judgment of the referring physicians and of the surgical team at our center.
Conclusion
In this study, several risk factors for 30-day mortality such as female gender, chronic dialysis, cardiogenic shock, prosthetic valve endocarditis, and NYHA class IV could be detected. They were partly depending not only on preoperative clinical status and pathogen spectrum, but also on surgical findings and variables. The strongest risk factors for 30-day mortality, which we found are not modifiable. However, female gender is associated with several modifiable parameters that should be taken into account. Yet, more ongoing multicenter studies are needed to evaluate intervention options.
Conflict of Interest
None declared.
Authors' Contribution
J.J.M. and C.F. shared the responsibility for conceptualization, methodology, validation, investigation, and project administration. J.J.M. was more responsible for data curation, whereas C.F. was mainly in charge of the formal analysis. They both wrote the original draft and did the review and editing.
* These authors share Equal authorship.
-
References
- 1 Lalanne S, Cattoir V, Guerin F, Verdier MC, Revest M. Differential response to antibiotic therapy in staphylococcal infective endocarditis: contribution of an ex vivo model. J Antimicrob Chemother 2023; 78 (07) 1689-1693
- 2 Chu VH, Park LP, Athan E. et al; International Collaboration on Endocarditis (ICE) Investigators*. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis: a prospective study from the International Collaboration on Endocarditis. Circulation 2015; 131 (02) 131-140
- 3 Fernández-Cisneros A, Hernández-Meneses M, Llopis J. et al; Equip d'Endocarditis de l'Hospital Clínic de Barcelona. Risk scores' performance and their impact on operative decision-making in left-sided endocarditis: a cohort study. Eur J Clin Microbiol Infect Dis 2023; 42 (01) 33-42
- 4 Gaca JG, Sheng S, Daneshmand MA. et al. Outcomes for endocarditis surgery in North America: a simplified risk scoring system. J Thorac Cardiovasc Surg 2011; 141 (01) 98-106 .e1, 2
- 5 Scheggi V, Menale S, Tonietti B. et al. Impact of septic cerebral embolism on prognosis and therapeutic strategies of infective endocarditis: a retrospective study in a surgical centre. BMC Infect Dis 2022; 22 (01) 554
- 6 Durante-Mangoni E, Bradley S, Selton-Suty C. et al; International Collaboration on Endocarditis Prospective Cohort Study Group. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch Intern Med 2008; 168 (19) 2095-2103
- 7 Albes JM. Current practice in prophylaxis of endocarditis: are we running into trouble?. Eur J Cardiothorac Surg 2019; 56 (01) 1-6
- 8 Friedrich C, Salem M, Puehler T. et al. Sex-specific risk factors for short- and long-term outcomes after surgery in patients with infective endocarditis. J Clin Med 2022; 11 (07) 1875
- 9 Tu JV, Jaglal SB, Naylor CD. Steering Committee of the Provincial Adult Cardiac Care Network of Ontario. Multicenter validation of a risk index for mortality, intensive care unit stay, and overall hospital length of stay after cardiac surgery. Circulation 1995; 91 (03) 677-684
- 10 Patrat-Delon S, Rouxel A, Gacouin A. et al. EuroSCORE II underestimates mortality after cardiac surgery for infective endocarditis. Eur J Cardiothorac Surg 2016; 49 (03) 944-951
- 11 Gatti G, Perrotti A, Obadia JF. et al; Association for the Study and Prevention of Infective Endocarditis Study Group–Association pour l'Étude et la Prévention de l'Endocadite Infectieuse (AEPEI). Simple scoring system to predict in-hospital mortality after surgery for infective endocarditis. J Am Heart Assoc 2017; 6 (07) e004806
- 12 Imaizumi T, Fujii N, Hamano T. et al; CRIC Study Investigators. Excess risk of cardiovascular events in patients in the United States vs. Japan with chronic kidney disease is mediated mainly by left ventricular structure and function. Kidney Int 2023; 103 (05) 949-961
- 13 Pacholewicz J, Kuligowska E, Szylińska A. et al. The rate of postoperative mortality and renal and respiratory complications are increased in patients with extreme obesity undergoing cardiac surgery - a retrospective observational cohort study of 8848 patients. Diabetes Metab Syndr Obes 2023; 16: 1155-1166
- 14 Nishimura RA, Otto CM, Bonow RO. et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 2017; 135 (25) e1159-e1195
- 15 The 2015 ESC guidelines for the management of infective endocarditis. Eur Heart J 2015; 36 (44) 3036-3037
- 16 Anantha Narayanan M, Mahfood Haddad T, Kalil AC. et al. Early versus late surgical intervention or medical management for infective endocarditis: a systematic review and meta-analysis. Heart 2016; 102 (12) 950-957
- 17 Lauridsen TK, Park L, Tong SY. et al. Echocardiographic findings predict in-hospital and 1-year mortality in left-sided native valve Staphylococcus aureus endocarditis: analysis from the international collaboration on endocarditis-prospective echo cohort study. Circ Cardiovasc Imaging 2015; 8 (07) e003397
- 18 Fowler Jr VG, Das AF, Lipka-Diamond J. et al. Exebacase for patients with Staphylococcus aureus bloodstream infection and endocarditis. J Clin Invest 2020; 130 (07) 3750-3760
- 19 Kim HJ, Kim JE, Lee JY, Lee SH, Jung JS, Son HS. Perioperative red blood cell transfusion is associated with adverse cardiovascular outcomes in heart valve surgery. Anesth Analg 2023; 137 (01) 153-161
- 20 Kwak SH, Ahn S, Shin MH. et al. Identification of biomarkers for the diagnosis of sepsis-associated acute kidney injury and prediction of renal recovery in the intensive care unit. Yonsei Med J 2023; 64 (03) 181-190
- 21 Ostovar R, Schroeter F, Erb M, Kuehnel RU, Hartrumpf M, Albes JM. Endocarditis: who is particularly at risk and why? Ten years analysis of risk factors for in-hospital mortality in infective endocarditis. Thorac Cardiovasc Surg 2023; 71 (01) 12-21
Address for correspondence
Publication History
Received: 07 September 2023
Accepted: 01 December 2023
Article published online:
19 February 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Lalanne S, Cattoir V, Guerin F, Verdier MC, Revest M. Differential response to antibiotic therapy in staphylococcal infective endocarditis: contribution of an ex vivo model. J Antimicrob Chemother 2023; 78 (07) 1689-1693
- 2 Chu VH, Park LP, Athan E. et al; International Collaboration on Endocarditis (ICE) Investigators*. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis: a prospective study from the International Collaboration on Endocarditis. Circulation 2015; 131 (02) 131-140
- 3 Fernández-Cisneros A, Hernández-Meneses M, Llopis J. et al; Equip d'Endocarditis de l'Hospital Clínic de Barcelona. Risk scores' performance and their impact on operative decision-making in left-sided endocarditis: a cohort study. Eur J Clin Microbiol Infect Dis 2023; 42 (01) 33-42
- 4 Gaca JG, Sheng S, Daneshmand MA. et al. Outcomes for endocarditis surgery in North America: a simplified risk scoring system. J Thorac Cardiovasc Surg 2011; 141 (01) 98-106 .e1, 2
- 5 Scheggi V, Menale S, Tonietti B. et al. Impact of septic cerebral embolism on prognosis and therapeutic strategies of infective endocarditis: a retrospective study in a surgical centre. BMC Infect Dis 2022; 22 (01) 554
- 6 Durante-Mangoni E, Bradley S, Selton-Suty C. et al; International Collaboration on Endocarditis Prospective Cohort Study Group. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch Intern Med 2008; 168 (19) 2095-2103
- 7 Albes JM. Current practice in prophylaxis of endocarditis: are we running into trouble?. Eur J Cardiothorac Surg 2019; 56 (01) 1-6
- 8 Friedrich C, Salem M, Puehler T. et al. Sex-specific risk factors for short- and long-term outcomes after surgery in patients with infective endocarditis. J Clin Med 2022; 11 (07) 1875
- 9 Tu JV, Jaglal SB, Naylor CD. Steering Committee of the Provincial Adult Cardiac Care Network of Ontario. Multicenter validation of a risk index for mortality, intensive care unit stay, and overall hospital length of stay after cardiac surgery. Circulation 1995; 91 (03) 677-684
- 10 Patrat-Delon S, Rouxel A, Gacouin A. et al. EuroSCORE II underestimates mortality after cardiac surgery for infective endocarditis. Eur J Cardiothorac Surg 2016; 49 (03) 944-951
- 11 Gatti G, Perrotti A, Obadia JF. et al; Association for the Study and Prevention of Infective Endocarditis Study Group–Association pour l'Étude et la Prévention de l'Endocadite Infectieuse (AEPEI). Simple scoring system to predict in-hospital mortality after surgery for infective endocarditis. J Am Heart Assoc 2017; 6 (07) e004806
- 12 Imaizumi T, Fujii N, Hamano T. et al; CRIC Study Investigators. Excess risk of cardiovascular events in patients in the United States vs. Japan with chronic kidney disease is mediated mainly by left ventricular structure and function. Kidney Int 2023; 103 (05) 949-961
- 13 Pacholewicz J, Kuligowska E, Szylińska A. et al. The rate of postoperative mortality and renal and respiratory complications are increased in patients with extreme obesity undergoing cardiac surgery - a retrospective observational cohort study of 8848 patients. Diabetes Metab Syndr Obes 2023; 16: 1155-1166
- 14 Nishimura RA, Otto CM, Bonow RO. et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Circulation 2017; 135 (25) e1159-e1195
- 15 The 2015 ESC guidelines for the management of infective endocarditis. Eur Heart J 2015; 36 (44) 3036-3037
- 16 Anantha Narayanan M, Mahfood Haddad T, Kalil AC. et al. Early versus late surgical intervention or medical management for infective endocarditis: a systematic review and meta-analysis. Heart 2016; 102 (12) 950-957
- 17 Lauridsen TK, Park L, Tong SY. et al. Echocardiographic findings predict in-hospital and 1-year mortality in left-sided native valve Staphylococcus aureus endocarditis: analysis from the international collaboration on endocarditis-prospective echo cohort study. Circ Cardiovasc Imaging 2015; 8 (07) e003397
- 18 Fowler Jr VG, Das AF, Lipka-Diamond J. et al. Exebacase for patients with Staphylococcus aureus bloodstream infection and endocarditis. J Clin Invest 2020; 130 (07) 3750-3760
- 19 Kim HJ, Kim JE, Lee JY, Lee SH, Jung JS, Son HS. Perioperative red blood cell transfusion is associated with adverse cardiovascular outcomes in heart valve surgery. Anesth Analg 2023; 137 (01) 153-161
- 20 Kwak SH, Ahn S, Shin MH. et al. Identification of biomarkers for the diagnosis of sepsis-associated acute kidney injury and prediction of renal recovery in the intensive care unit. Yonsei Med J 2023; 64 (03) 181-190
- 21 Ostovar R, Schroeter F, Erb M, Kuehnel RU, Hartrumpf M, Albes JM. Endocarditis: who is particularly at risk and why? Ten years analysis of risk factors for in-hospital mortality in infective endocarditis. Thorac Cardiovasc Surg 2023; 71 (01) 12-21