

Subscribe to RSS
DOI: 10.1055/s-0044-1779630
Transnasal Endoscopic Repair of Posttraumatic Meningoencephalocele: A Rare Presentation
Authors


Abstract
Meningoencephalocele is a rare condition that results due to defect in skull base causing brain tissue to herniate along with meninges. We present a case of posttraumatic meningoencephalocele in an 11-year-old child, who presented with nasal mass and cerebrospinal fluid leak. A cribriform plate defect was detected on magnetic resonance imaging along with herniation of brain tissue. The big defect was successfully repaired endoscopically in multiple layers and without placement of a lumbar drain, thereby reducing the complications of an open transcranial surgery.
Keywords
CSF leak - endoscopic skull base surgery - meningitis - meningoencephalocele - nasal Mass - skull baseIntroduction
Nasal meningoencephalocele, also known as encephalocele or cephalocele, is an uncommon condition. In addition to congenital origin, it can also be caused by trauma or even spontaneously.[1] Meningoencephalocele can present as unilateral nasal mass leading to nasal obstruction.[2] Biopsy of such lesions without prior imaging is contraindicated because it carries a high risk of cerebrospinal fluid (CSF) leak and meningitis.[3] If such patients are misdiagnosed or incorrectly handled, it can lead to serious ascending infections and/or a constant CSF leak.[2] These complex lesions require a multidisciplinary approach for correct diagnosis and treatment.[2]
Recent technological advances have made endoscopic repairs as a first choice over traditional transcranial repairs. With the use of microdebrider and coblator procise intraoperative localization of CSF fistula and excision of big meningoencephalocele can be undertaken safely.[4]
Case Report
An 11-year-old boy presented to the Department of Otorhinolaryngology of Indus International Hospital Dera Bassi, with the complaints of nasal obstruction on right side with clear watery discharge from the right side since many years. Patient was receiving symptomatic treatment in form of antiallergics since many years. At the age of 3, the child fell from height with development of symptoms 2 years afterward. There were no episodes of fever with headache all these years.
Physical examination revealed no signs of meningitis or fever. Nasal endoscopy revealed a pulsating pinkish blue-colored mass on right side arising lateral to middle turbinate. To ascertain the presence of a CSF leak patient was asked to lean forward that resulted in dripping of clear fluid from the right nostril.
The child was subjected to computed tomography (CT) and magnetic resonance imaging (MRI) of nose, paranasal sinuses, and brain ([Fig. 1])
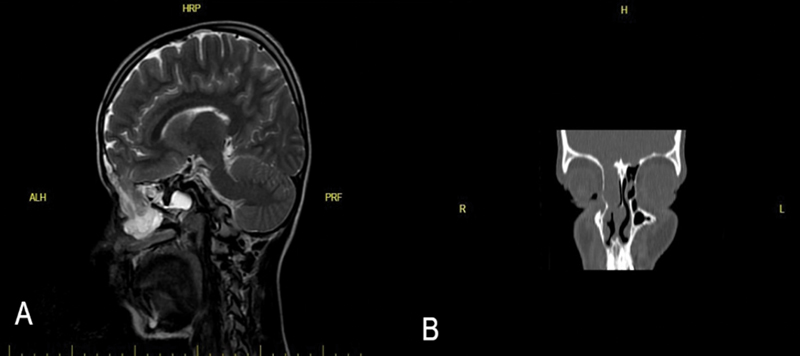
The MRI showed a defect in the cribriform plate of size approximately 1.75 × 1.5 cm with herniation of Basi-frontal brain parenchyma. In Sagittal T2, it was revealed that gliotic tissue and meninges had herniated into the nasal cavity through the bony defect. Coronal CT bone window shows defect in cribriform plate with opacification of ethmoidal air cells.
The patient was subjected to endoscopic skull base surgery for excision of meningoencephalocele and repair of skull base. Using a transnasal endoscopic approach, the surgical management was carried out in general anesthesia. Patient was placed in the reverse Trendelenburg position to decrease the capillary blood flow. Nasal cavity was decongested using topical adrenaline solutions in 1:4 dilution. Microdebrider was used for maxillary antrostomy and anterior and posterior ethmoidectomies. ArthroCare Coblation System with Procise max wand was used to ablate the tissue ([Fig. 2B]).

The precise ablation and excision of the tissue ([Fig. 2B]) revealed a skull base defect of size 1.7 × 1.3 ([Fig. 2C]). The margins of the defect were freshened and mucosa was meticulously removed from the margins. Intracranial side of defect was freed using an elevator and recipient bed was prepared for placement of graft. The defect was repaired using cartilage harvested from nasal septum and it was reinforced with fascia lata graft harvested from right thigh. After ensuring that there was no further leak, Tisseel fibrin glue was applied to hold the tissue and then rotated middle turbinate flap was put keeping the frontal sinus drainage intact. The entire repair was further supported with Surgicel Gelfoam patties. Patient did not require placement of any lumbar drain in the intraoperative or postoperative period. A complete bed rest was ensued for 5 days.
The excised sac was sent for histopathological examination.
The H/E slides showed herniated glial tissue along with meningeal tissue and confirmed the diagnosis of meningoencephalocele ([Fig. 3]).

The postoperative phase went smoothly. On 5th postoperative day, the nasal packs were removed and child was finally discharged on 7th postoperative day. The child has been under a regular follow-up with no residual or recurrent symptoms.
Discussion
Meningoencephaloceles occur due to a bony defect in the skull base that results in herniation of brain tissue. They can be spontaneous or acquired. If acquired, they can occur secondary to trauma, infection, or neoplasia.[4] Majority of the acquired causes (96%) arise after trauma.[5]
Nasal cavity and ethmoidal sinuses are in close proximity with the skull base. Anteriorly the skull base gets perforated by olfactory fibers that renders it weaker. This part gets fractured in trauma with the resultant CSF leak and herniation of meninges and brain tissue into the sinuses.[5] Following a trauma, CSF leak may develop anytime within first few hours to months. In our case, CSF leak developed a couple of years later along with nasal obstruction. Although recurrent meningitis can develop in prolonged untreated cases, in our case patient never developed meningitis.
Beta-2 transferrin is usually required to establish the diagnosis of CSF leak, but our case had a big meningoencephalocele with CSF leak and the diagnosis was made by clinical and radiological examination alone.
Imaging techniques such as thin section CT, CT cisternography, MRI, and MR cisternography are used to determine fistula localization in patients with determined CSF leak.[6] In our case, thin-section CT followed by MR cisternography clinched the diagnosis along with size and site of the defect.
Encephaloceles are classified according to the anatomical area of bone defect. Gerhardt classification includes occipital, head dome, frontoethmoidal and basal encephalocoeles.[5] In our case, appearance of frontoethmoidal encephalocele was observed.
Since the pathology is progressive and potentially life threatening, more invasive procedures are required. Surgical treatment forms the mainstay of management of meningoencephalocele.
Repairing meningoencephalocele can be accomplished by different techniques like open transcranial and transfacial methods, pure endoscopic, or combined approaches. For larger defects, although endoscopic approach can be used, open approaches still remain more reliable technique.[7] Meningoencephalocele in children has been traditionally treated with transcranial approaches that are associated with higher complications. When left untreated, children can develop recurrent meningitis and epilepsy that might not respond well to medications.[8]
In the years since Wigand's first report in 1981, the use of transnasal endoscopic approach to repair CSF rhinorrhea has evolved greatly.[8]
The use of endoscopic technique for repair of skull base defects has been observed to greatly reduce postoperative morbidity as well as residual symptoms. In our case too, the patient was discharged on 7th postoperative day. Follow-up was uneventful till date. Additionally, the complications associated with craniotomy, such as anosmia and intense headaches, are also avoided. Weather the defect is small or large, endoscopic technique can be used for repair.[9] In our case, the defect was less than 2 cm so endoscopic approach was preferred.
Different techniques can be used to reconstruct skull-based defects. The type of filling materials is selected based on a number of factors, including the defect's size and localization, underlying pathology and surgical experience of the surgeon. There are a variety of materials that can be used for the two-layer reconstruction methods. Commonly used materials are fascia lata, fat graft, and septonasal flap.[10] In our case, we did a four-layered repair using cartilage, fascial lata, rotated middle turbinate flap and reinforced with Tisseel glue and Surgicel Gelfoam patty.
In conclusion, it can be said that frontoethmoidal meningoencephalocele is a rare entity. Such an entity if presents with only nasal obstruction and nasal discharge without any complications like fever, meningitis for years altogether makes in even rarer. In our case, the meningoencephalocele masqueraded a nasal polyp and patient never developed any complications in the period from trauma to treatment. Patient underwent a successful endoscopic repair without any significant intraoperative/postoperative complications, thereby ensuring an early recovery as compared to intracranial approaches. Also, no placement of lumbar drain ensued less complications in the postoperative period.
Conflict of Interest
None declared.
Authors' Contribution
All authors reported provision of study materials, medical writing by K.C., A.N., and T.S.J. All authors have contributed significantly to diagnosis and management of patient, along with compiling of academic text of the article.
-
References
- 1 Xue L, Gehong D, Ying W, Jianhua T, Hong Z, Honggang L. Nasal meningoencephalocele: a retrospective study of clinicopathological features and diagnosis of 16 patients. Ann Diagn Pathol 2020; 49: 151594
- 2 Bagger-Sjöbäck D, Bergstrand G, Edner G, Anggård A. Nasal meningoencephalocele. A clinical problem. Clin Otolaryngol Allied Sci 1983; 8 (05) 329-335
- 3 Mukerji SS, Parmar HA, Gujar S, Passamani P. Intranasal meningoencephalocele presenting as a nasal polyp–a case report. Clin Imaging 2011; 35 (04) 309-311
- 4 Liu S, Tang R, Mao S, Zhang W. Clinical outcomes of coblation-assisted pediatric endoscopic endonasal skull base surgery. Int J Pediatr Otorhinolaryngol 2022; 156: 111089
- 5 Muranjan SN, Singhal DD, Shah SH, Shah AK. Bilateral idiopathic temporal bone meningoencephaloceles - an unusual presentation. J Postgrad Med 2021; 67 (04) 228-231
- 6 Cullu N, Deveer M, Karakas E, Karakas O, Bozkus F, Celik B. Traumatic fronto-ethmoidal encephalocele: a rare case. Eurasian J Med 2015; 47 (01) 69-71
- 7 Geyik M, Erkutlu I, Alptekin M. et al. Anterior skull base defects reconstructed using three-layer method: 78 consecutive cases with long-term follow-up. J Neurol Surg B Skull Base 2016; 77 (06) 499-502
- 8 Vemuri NV, Karanam LSP, Manchikanti V, Dandamudi S, Puvvada SK, Vemuri VK. Imaging review of cerebrospinal fluid leaks. Indian J Radiol Imaging 2017; 27 (04) 441-446
- 9 Keshri AK, Shah SR, Patadia SD, Sahu RN, Behari S. Transnasal endoscopic repair of pediatric meningoencephalocele. J Pediatr Neurosci 2016; 11 (01) 42-45
- 10 Kosmidou P, Ntarladima V, Katsimantas A, Filippou D, Georgalas C. Endoscopic surgical repair of a giant, postoperative, neglected meningoencephalocele. Cureus 2020; 12 (01) e6739
Address for correspondence
Publication History
Article published online:
08 February 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Xue L, Gehong D, Ying W, Jianhua T, Hong Z, Honggang L. Nasal meningoencephalocele: a retrospective study of clinicopathological features and diagnosis of 16 patients. Ann Diagn Pathol 2020; 49: 151594
- 2 Bagger-Sjöbäck D, Bergstrand G, Edner G, Anggård A. Nasal meningoencephalocele. A clinical problem. Clin Otolaryngol Allied Sci 1983; 8 (05) 329-335
- 3 Mukerji SS, Parmar HA, Gujar S, Passamani P. Intranasal meningoencephalocele presenting as a nasal polyp–a case report. Clin Imaging 2011; 35 (04) 309-311
- 4 Liu S, Tang R, Mao S, Zhang W. Clinical outcomes of coblation-assisted pediatric endoscopic endonasal skull base surgery. Int J Pediatr Otorhinolaryngol 2022; 156: 111089
- 5 Muranjan SN, Singhal DD, Shah SH, Shah AK. Bilateral idiopathic temporal bone meningoencephaloceles - an unusual presentation. J Postgrad Med 2021; 67 (04) 228-231
- 6 Cullu N, Deveer M, Karakas E, Karakas O, Bozkus F, Celik B. Traumatic fronto-ethmoidal encephalocele: a rare case. Eurasian J Med 2015; 47 (01) 69-71
- 7 Geyik M, Erkutlu I, Alptekin M. et al. Anterior skull base defects reconstructed using three-layer method: 78 consecutive cases with long-term follow-up. J Neurol Surg B Skull Base 2016; 77 (06) 499-502
- 8 Vemuri NV, Karanam LSP, Manchikanti V, Dandamudi S, Puvvada SK, Vemuri VK. Imaging review of cerebrospinal fluid leaks. Indian J Radiol Imaging 2017; 27 (04) 441-446
- 9 Keshri AK, Shah SR, Patadia SD, Sahu RN, Behari S. Transnasal endoscopic repair of pediatric meningoencephalocele. J Pediatr Neurosci 2016; 11 (01) 42-45
- 10 Kosmidou P, Ntarladima V, Katsimantas A, Filippou D, Georgalas C. Endoscopic surgical repair of a giant, postoperative, neglected meningoencephalocele. Cureus 2020; 12 (01) e6739