

Subscribe to RSS
DOI: 10.1055/s-0044-1779605
Association of Evening Eating with Sleep Quality and Insomnia among Adults in a Brazilian National Survey
Authors
Fundings This work was supported by Fundação de Amparo à Pesquisa do Estado de Alagoas - FAPEAL (Grant/Award Number: 60030.0000002539/2022). AKPP received a master's scholarship from FAPEAL. MOL received a master's scholarship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - CAPES. MEBN received a scientific initiation scholarship from CNPq.

Abstract
Objective To examine the association of evening eating clock time, its elapsed time to the midpoint of sleep (TEM), consumption of caffeine and sugary foods, and dinner meal size with sleep quality indicators and insomnia.
Methods The present study's participants (n = 2,050; 18–65 y) were part of a population-based research, with virtual data collection. Logistic regression models were fitted to assess differences in the odd ratios (ORs) (95% confidence interval [CI]) of sleep duration < 7 hours, sleep latency > 30 min, poor sleep quality, and insomnia (outcomes) with the evening diet-related variables. Linear regression analyses evaluated differences in sleep duration and latency associated with the same variables. Restricted cubic splines were used to investigate the shape of the association of mealtime and TEM with sleep duration and latency.
Results For each hour delay in evening eating and increase in the duration of TEM, the odds of sleep duration < 7 h [OR(95%CI):1.30(1.20,1.40); OR(95%CI):0.51(0.47,0.56)], sleep latency > 30 [OR(95%CI):1.14(1.07,1.22); 0.88(0.83,0.94)], poor sleep quality [OR(95%CI):1.21(1.13,1.30); 0.80(0.76,0.85)] and insomnia [OR(95%CI):1.12(1.04,1.20); 0.89(0.84,0.95)], respectively, increased and decreased. We found a dose-response association of evening eating (clock time and TEM) with sleep duration. The shortest latency was seen when evening eating was at ∼ 8 PM and ∼ 7 to 8 hours before the midpoint of sleep. Participants who reported dinner as their largest meal and consumed caffeine and/or sugary foods/beverages after 6 PM presented higher odds of sleep duration < 7 hours, poor sleep quality, and insomnia.
Conclusions Our findings indicate that an early-eating schedule has beneficial sleep effects and that it will be necessary to consider evening eating patterns and timing, along with sleep and circadian hygiene, to improve sleep quality and circadian health.
Introduction
Insufficient sleep, poor sleep quality, and insomnia are significant public health problems and common complaints in clinical practice. Approximately 10% of the adult population suffers from an insomnia disorder and another 20% experience occasional insomnia symptoms.[1]
About ⅓ of the general population is affected by insufficient sleep,[2] and in a global quantification of sleep schedules using smartphone data, Brazil appeared as the third country with the shortest sleep duration.[3] Sleep complaints, and symptoms—including nonrestorative sleep, difficulty initiating or maintaining sleep, and daytime sleepiness—are also common in the general population.[2] [4]
Although there are several risk factors and adverse outcomes arising from sleep-related problems, emerging evidence is accumulating to suggest that sleeping and eating habits are closely related, and both serve as important modifiable behaviors that can affect health outcomes.[5] While there is increasing evidence for the influence of sleep on lifestyle and dietary intake,[6] [7] [8] [9] [10] the impact of eating patterns on sleep quality has been less studied.[11]
It has long been widespread that the consumption of stimulant-containing foods and beverages, especially in the evening and close to bedtime, may affect elements of sleep.[12] [13] An example is caffeine, which is an adenosine receptor antagonist, a hormone that regulates sleep-wake cycles, and may attenuate the increase in sleep pressure during wakefulness[14] and lead to delayed sleep initiation and more superficial sleep.[15]
The quality of carbohydrates may also be relevant for sleep: while more fiber intake has been associated with greater deep sleep,[16] a higher sugar intake has been associated with lighter, less restorative sleep with more arousals.[17] [18] [19] [20]
However, other studies do not confirm these associations,[21] and the connection between diet and sleep quality still warrants further investigation.[11]
Furthermore, although for decades, diet composition has been the central focus, more recently, especially with the advancement of research in the field of chrononutrition, temporal eating patterns have received special attention. Evidence suggests that the timing of eating, regardless of its composition, may contribute to circadian system misalignment, directly affecting sleep, as well as weight status and metabolic health.[22] [23] [24] [25] [26] [27]
Some observational studies have shown that eating close to bedtime was associated with impaired sleep quality.[22] [23] [24] On the other hand, a randomized crossover study found that shifting dinner timing from 5 hours before sleep to 1 hour before sleep in healthy volunteers did not result in significant adverse changes in overnight sleep architecture.[24]
It is important to emphasize that one relevant aspect of meal timing studies is to define what a late meal is,[25] and it seems that the clock timing by itself may not be useful to study metabolic alterations related to evening meal timing. It is known that the beginning of the biological night, as assessed by melatonin onset under dim light conditions (Dim Light Melatonin Onset; DLMO), may differ between individuals depending on their circadian timing or chronotype. For example, some subjects with early chronotypes present early melatonin onsets (DLMO around 19:00). Late chronotypes have late melatonin onsets (DLMO around 1:00), while neither type has their melatonin onset around 22:00,[28] with interindividual differences of 6 or more hours in the timing in which the biological night starts in different chronotypes. In this sense, an evening meal at 21:00 may be a late circadian meal for those subjects with melatonin onsets at 19:00, but it may be an early circadian dinner for those whose biological night starts at 1:00. Considering that high endogenous melatonin levels may impair glucose, a late evening meal, determined by clock time, may have different metabolic effects depending on the individual's biological night and/or the concurrence of food intake with high endogenous melatonin levels.[29]
In view of this, McHill et al.[30] studied the association between the timing of food intake and DLMO and demonstrated that eating closer to, or after, DLMO was significantly associated with higher body fat, independent of dietary intake and the level of physical activity. This approach, however, requires repeated blood or saliva collection to evaluate DLMO, and participants need to stay in dim light conditions for many hours, which is not practical for most epidemiological studies.[29]
Considering the aforementioned, Zerón-Rugério et al.[31] proposed the measurement of the elapsed time between dinner and the midpoint of sleep as a practical approach to examining the timing of food intake relative to internal circadian timing. It is important to note that the midpoint of sleep has the highest correlation with DLMO and is also considered to be a marker of the chronotype.[32] Such study found that dining 6 hours before the midpoint of sleep was associated with the lowest values of adiposity.[31] However, to our knowledge, this parameter has not yet been applied in studies with sleep as the outcome.
As seen, the connection of both diet composition and timing with sleep remains a significant controversy and warrants further investigations. Therefore, we conducted the first Brazilian investigation addressing whether evening eating timing (including both clock time and circadian time, measured by the elapsed time between the last evening meal and the midpoint sleep) is associated with sleep quality indicators (duration, latency, and self-perceived sleep quality) and insomnia. Furthermore, we investigated if caffeine and sugary foods consumption (after 18:00) and reporting dinner as the largest meal of the day were associated with sleep variables.
Material and Methods
Study Design and Population
The present study was performed with data from the first and second stages of the SONAR-Brazil Survey, which aims to investigate chronobiological aspects related to sleep, food, and nutrition in Brazilian adults. This is exploratory, population-based research, with data collection exclusively in a virtual environment. The participants were adults, non-pregnant, aged between 18 and 65 years, born and residing in all regions of Brazil (n = 2,140). After excluding participants who declared being shift workers (n = 90), the final sample totalized 2,050 non-pregnant Brazilian adults.
Considering a large population, to estimate population proportions with a confidence level of 95% and a margin error of 5%, we defined, a priori, a minimum sample size of 385 valid questionnaires. However, the sample size remained open, and the efforts were directed to increase participation as much as possible to minimize the error margin. The final sample of 2,050 guarantees proportion estimates with a 95% confidence level and a margin of error lower than 4%. All data collection procedures have been conducted according to the Declaration of Helsinki and approved by the Committee of Research Ethics of Universidade Federal de Alagoas (CAAE: 48689221.3.0000.5013).
Recruitment took place between August 2021 and September 2022, and data were collected using a Google Form (Google LLC., Menlo Park, CA, USA). By clicking on the research link, the volunteer respondents were directed to an informed consent form and, only after indicating their consent to participate in the study, they were directed to the questionnaire, made up of four blocks: characterization, health and lifestyle, sleep characteristics, and eating and sleeping schedules. The generated responses were automatically stored in spreadsheets compatible with Microsoft Office Excel (Microsoft Corp., Redmond, WA, USA) and later exported to the statistical software STATA 13 statistical software (Stata Corp LLC, College Station, TX, USA) for statistical analyses. The link to the online questionnaire was disseminated in several ways: referral of health professionals' reports in newspapers/magazines, advertisements on social media platforms, research institutes, health fairs, events, scientific journals, and electronic pages addressing the research participants, to increase research visibility and, consequently, data collection.
Sleep Traits and Circadian Parameters
In the questionnaire block about eating and sleeping schedules, the participants were informed: ‘In this section, we want to know your routine on weekdays/work-days and weekends/free days’. The following questions were used to measure usual sleep and wake times: ‘Considering your habits during the last month, on a typical weekday [or weekend] 1. What time do you wake up? 2. What time do you sleep?’ Responses were in 30-minute increments.
Sleep duration (in hours) was calculated as the difference between bedtime and wake-up time.[26] [27] We also calculated the midpoint of sleep on weekdays and weekends, defined as the middle time point between bedtime and wake-up timing.[26] [33]
The average weekly sleep duration, wake-up time, bedtime, and the midpoint of sleep were calculated as follows: ([5 × sleep duration/wake-up time/bedtime/midpoint of sleep on weekdays] + [2 × sleep duration/wake-up time/bedtime/midpoint of sleep on weekends])/7.[26] [27]
We adopted the midpoint of sleep on free days corrected for sleep extension on free days (MSFsc) as an indicator of chronotype, which is proposed to clean the chronotype of the confounder sleep debt.[32] For participants whose sleep duration on free days was longer than on workdays, the midpoint was calculated as follows: (bedtime on free days + [sleep duration on free days/2]). For participants whose sleep duration on free days was shorter than on workdays, due to the sleep debt accumulated over the workweek, the corrected midpoint of sleep was applied, and calculated as follows: (bedtime on free days + [weekly average sleep duration/2]). For more details on the methodology see the studies by Roenneberg et al.[32] [33]
Sleep latency was investigated by asking: ‘During the past month, how long (in minutes) has it usually taken you to fall asleep each night?’ and nocturnal awakenings by: 'How many times do you wake up during the night, after sleep onset?'.
Considering the cutoff points established by the American Sleep Foundation for classifying sleep quality indicators, sleep variables were categorized into sleep duration < 7 or ≥ 7 hours/night, sleep latency ≤ 30 or > 30 minute/night, nocturnal awakening ≤ 1 or > 1/night.[4]
Self-perception of sleep quality was investigated based on the question: ‘How do you rate the quality of your sleep?’, with the possible answers: very good, good, poor, and very poor. We considered poor sleep quality for those who answered poor or very poor.
Finally, participants were asked, ‘Do you have a diagnosis of any of the following sleep disorders?’ Possible answers included insomnia.
Evening Eating Clock Time
According to the Chrononutrition Profile Questionnaire,[34] [35] evening eating refers to the clock time of the last eating event, and it was assessed by asking participants: ‘Considering your habits during the last month, on a typical weekday/workday (or weekend/free/day): What time do you usually have your last eating event?’, and responses were in 30-minute increments. The instrument clarified that it included any food and/or drink that contained calories. The weekly average clock time of the last eating event was calculated as follows: ([5 × evening eating timing on weekdays] + ]2 × evening eating timing on weekends])/7.[34] [35]
Participants were also asked: ‘What is your largest meal of the day?’,—which refers to the meal in which participants consume the greatest amount of calories, and possible responses were: Breakfast, lunch, dinner, none, or other.[34] [35] In the analyses, we combined the responses None and Other.
The Elapsed Time between Evening Eating and the Midpoint of Sleep (TEM)
We calculated the elapsed time between the last eating event and the midpoint of sleep (TEM) considering the weekly average value of the midpoint of sleep and evening eating clock time, as follows: ([midpoint of sleep + 24] – last eating event timing). This variable was subsequently dichotomized into less or more than 6 hours.[31]
Evening Dietary Traits
Food consumption was investigated using a food frequency questionnaire comprising 19 food/preparation categories, for which participants selected the frequency of weekly consumption: never, sometimes (1–3 days/week), almost always (4–6 days/week), or always (6–7 days/week). Sequentially, participants reported the daily frequency and times of consumption, with responses in the intervals between 6:01–9:00 AM, 9:01 AM–12:00 PM, 12:01–3:00 PM, 3:01–6:00 PM, 6:01–9:00 PM, 9:01 PM–12:00 AM, after 12:00 AM.
We evaluated the evening diet quality, considering the frequency of food consumption after 6 PM, based on the Food Guide for the Brazilian Population as proposed in a previous study.[26] [27]
Food markers for healthy eating (fresh fruits; vegetables and/or legumes; beans, chickpeas, lentils and/or peas; milk and/or dairy products; eggs; meats; fish) received increasing scores (never = 0; sometimes = 1; almost always = 2; always = 3), while unhealthy eating markers (snacks; chocolate; fried snacks; instant noodles, packaged snacks or crackers; fast food; hamburger and/or sausages; coffee; soda cola-based; sweetened beverages; mate or black tea; guarana powder; alcoholic beverages) received decreasing scores (never = 3; sometimes = 2; almost always = 1; always = 0). From the sum of the scores of each food category, the total score of the Diet Quality Index (DQI) was obtained, which could range from 0 to 57 points, with a higher score suggestive of a higher frequency of consumption of healthier foods and lower frequency of consumption of unhealthy foods. Sequentially, from the available scores, tertiles were created for diet quality classification: 1st tertile – low quality (21–34 points); 2nd tertile – intermediate quality (35–38 points), and 3rd tertile – good quality (39–47 points).
Furthermore, we analyzed evening consumption (after 6 PM) of sugary food/beverages, which includes snacks (sweets, cake, cookies, candy, lollipops), chocolate, and/or sweetened beverages, and caffeine foods/beverages, which included coffee, cola-based soda, mate or black tea, and/or guarana powder. We considered consumers participants who reported consuming at least one of the mentioned food/beverage items sometimes (1–3 days/week), almost always (4–6 days/week), or always (6–7 days/week).
Lifestyle Traits
Physical exercise was measured through the following questions: ‘On which days of the week do you practice physical exercise (moderate-to-vigorous-intensity activity)?’
Screen time per day was evaluated by the questions: ‘In your free time (not counting work/study), how many hours/day do you spend watching TV, on your computer, tablet, or cell phone?’
For anthropometric evaluation, the body mass index (BMI) (weight [Kg]/height(m)2) was calculated, based on self-reported weight and height. The classification of nutritional status was performed based on the cutoff points established by the World Health Organization.[36] [37]
Some other details of the survey questionnaire concerning other covariates including region, education, marital status, and smoking were included in our study.
Statistical Analyses
To assess differences between self-perception of sleep quality (good or poor) and insomnia (yes or no), in their characteristics, evening eating, sleep, and lifestyle traits, the Student t-test (for continuous variables), and the Chi-square test (for categorical variables) were performed.
Logistic regression models were fitted to assess differences in the ORs (95% CI) of short sleep duration (< 7 hours/night), sleep latency > 30 min., poor sleep quality, and insomnia (as outcomes) with the continuous and categorical evening diet-related variables (clock time, TEM, dinner as the largest meal of the day, diet quality, caffeine, and sugary consumption).
Linear regression analyses evaluated differences in sleep duration and sleep latency (as the outcome variable) associated with the same evening diet-related variables. Regression coefficient (β) and 95% CIs were calculated for the unadjusted and adjusted models.
Moreover, restricted cubic splines were also used to study the shape of the association of eating event clock time and its elapsed time from midpoint sleep (TEM) with sleep duration and sleep latency.
All the multiple analyses were adjusted for the potentially confounding variables: age, sex, region, physical exercise frequency, BMI, marital status, and scholarship. A p-value ≤ 0.05 was considered statistically significant.
Results
A total of 2,050 adults (age: 34 years old [range 18–65]; 73% of women) took part in the study ([Table 1]). [Table 1] presents the characteristics of the studied participants, depending on sleep quality (good or poor) and insomnia (yes or no). Among all participants, ∼ 30% reported poor self-perception of sleep quality, and ∼ 26% reported insomnia.
Abbreviations: BMI, body mass index; TEM, time between evening eating and the midpoint of sleep.
Values are shown as means ± SDs or percentages. P-values are derived from the Student t-test (for continuous variables) and from the Chi-square test (for categorical variables).
Significant p-values ≤ 0.05 are shown in bold.
Among participants with poor sleep quality and insomnia, the BMI average and the prevalence of overweight were higher, compared with the group with good sleep quality (50.08% versus 42.13%) and without insomnia (52.73% versus 41.63%) (all p < 0.001) ([Table 1]).
The poor sleep quality group reported the last eating event later and closer to the midpoint of sleep, compared with the good sleep quality group (differences of more than 30 minutes) (p < 0.001). Likewise, participants with insomnia reported the last eating event later (difference of 13 minute) when compared with participants without the disorder, and 31% consumed it less than 6 hours before the MS (versus 24%) (all p < 0.005) ([Table 1]).
Dinner was referred to as the largest meal of the day by more than 11% of the participants, and the percentage was higher among those with poor sleep quality (∼ 14%) and insomnia (∼ 13%), compared, respectively, to those with good sleep quality (∼ 9%) and without the disorder (∼ 10%) (p < 0.05) ([Table 1]).
Furthermore, in both group comparisons, participants with poor sleep quality and those with insomnia more frequently reported evening (after 6 pm) consumption of caffeinated foods/beverages (∼ 49% versus 40%) and sugary food (∼ 54% versus 47%) (all p < 0.05) ([Table 1]).
Regarding sleep traits, the groups with poor sleep quality and insomnia slept later (differences of 32 and 29 minutes, respectively) and, as expected, had shorter sleep duration (differences of 24 and 8 minutes, respectively), higher frequency of nocturnal awakenings, and longer latency duration (All p < 0.05) ([Table 1]).
Regarding lifestyle traits, 67% of the participants practiced physical exercise, with a higher prevalence among those with good sleep quality (70%) and who did not have insomnia (68%) (p < 0.001). Few participants were smokers (6%), but the prevalence was higher among those with insomnia (p = 0.003) ([Table 1]).
The results of the univariate and multiple logistic analyses are shown in [Table 2]. In the adjusted models, each additional hour of the evening eating clock time increased the odds of short sleep duration by 30% (OR: 1.20, 1.40; p < 0.001), of sleep latency > 30 min by 14% (95% CI: 1.06, 1.22; p < 0.001), of poor sleep quality by 21% (95% CI: 1.12, 1.29; p < 0.001), and of insomnia by 11% (95% CI: 1.04,1.20; P: 0.002).
Abbreviations: CI, confidence interval; OR, odds ratio; TEM, time between evening eating and the midpoint of sleep.
Data are presented as OR (95% CI) and the multiple models are adjusted for age, sex, region, physical exercise frequency, BMI, marital status, and scholarship.
Significant p-values ≤ 0.05 are shown in bold.
The elapsed time between last eating event and the midpoint of sleep showed a protective effect on short sleep duration (OR [95% CI]:0.51 [0.47,0.56]; p < 0.001), longer sleep latency (OR [95% CI]: 0.88 [0.83,0.94]; p < 0.001), poor sleep quality (OR [95% CI]: 0.80 [0.75,0.85]; p < 0.001), and insomnia (OR [95% CI]: 0.89 [0.83,0.94]; p < 0.001). In the analysis with the same dichotomized variable, among those who had the last eating event ≤ 6 hours before the midpoint of sleep, the OR of short sleep duration was 6.54 (95% CI: 5.14,8.32; p < 0.001), of sleep latency > 30 min was 1.35 (95% CI: 1.08, 1.69; p = 0.008), of poor sleep quality was 2.08 (95% CI: 1.67, 2.58; p < 0.001), and of insomnia was 1.50 (95% CI: 1.19, 1.88; p < 0.001) ([Table 2]).
Furthermore, participants who reported dinner as the largest meal of the day presented 51% higher odds of having short sleep duration (95% CI: 1.11, 2.07; P: 0.009), 47% higher odds of having latency > 30 min (95% CI: 1.09, 1.97; p = 0.01), 52% higher odds of perceiving sleep quality as poor (95% CI: 1.13, 2.03; P:0.01), and 34% higher odds of having insomnia (95% CI: 0.99, 1.82; P:0.05) ([Table 2]).
Still, participants who consumed caffeinated food or drinks after 6 PM were 33% (95% CI: 1.07, 1.66; P: 0.009) more likely to have short sleep duration, 33% more likely to report poor sleep quality (95% CI: 1.09, 1.62; P: 0.004), and 35% more likely to have insomnia (95% CI: 1.09, 1.65; P: 0.004). The consumption of sugary foods after 6 PM also increased the odds of latency lasting longer than 30 minutes (OR [95% CI]: 1.26 [1.03; 1.54]; P:0.02), poor sleep quality (OR [95% CI]: 1.24 [1.02; 1.51]; P: 0.02), and insomnia (OR [95% CI]: 1.35 [1.10, 1.66]; P: 0.02) ([Table 2]). All these associations were independent of age, sex, region, physical exercise frequency, BMI, marital status, and scholarship.
The linear regression analysis ([Table 3]) shows, after adjustment for the same confounding variables, that for each additional hour in the clock time of the last eating event, there was an 8 minute decrease in sleep duration [β (95% CI): −0.14 (−0.17, 0.10); p < 0.001] and also a 2.71 minute increase in sleep latency time [95% CI: 1.60, 3.81; p < 0001].
Abbreviations: CI, confidence interval; TEM, time between evening eating and the midpoint of sleep.
Data are presented as β-coefficient (95% CI) and the multiple models are adjusted for age, sex, region, physical exercise frequency, BMI, marital status, and scholarship.
Significant p-values ≤ 0.05 are shown in bold.
Additionally, for each additional hour in the elapsed time between the last eating event and the midpoint of sleep, there was a 21 min increase in sleep duration [β (95% CI): 0.35 (0.33, 0.38); p < 0001] and a 2.66-minute decrease in the duration of sleep latency [β (95% CI): −2.66 (−3.63, −1.69); p < 0.001]. Among those who had the last eating event ≤ 6 hours before the midpoint of sleep, we found a decrease of 1:06 minutes in sleep duration [β (95% CI): −1.08(−1.19, −0.97); p < 0.001] and an increase of 6.78 minutes in sleep latency (95% CI: 3.09, 10.46; p < 0.001) ([Table 3]).
Furthermore, individuals who reported having dinner as the largest meal of the day showed a 12-minute decrease in sleep duration (β [95% CI]: −0.20 [−0.36, −0.04]; P: 0.01), and an increase of 9.29 minutes in sleep latency time (95% CI: 4.27, 14.31; p < 0.001) ([Table 3]).
Among participants who consumed caffeinated food or beverages after 6 PM, a 13-minute decrease in sleep duration was observed (β [95% CI]: −0.22 [−0.32, −0.11]; p < 0.001), and a 3.36-minute increase in latency time (95% CI: 0.09, 6.64; P:0.04). Finally, among those with evening sugary foods consumption, the sleep latency increased by 5.12 minutes (95% CI: 1.91, 8.33, P: 0.002) ([Table 3]).
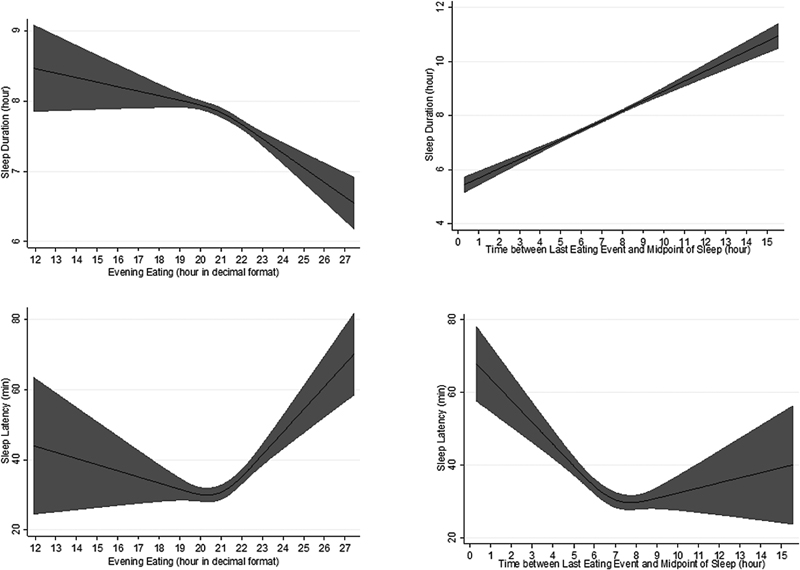
Restricted cubic splines ([Fig. 1]) provide interesting insights. There was a dose-response association between sleep duration and both evening eating time and its elapsed time to the midpoint of sleep. Increasing the interval between the last eating event and the midpoint of sleep, sleep duration increases as well (a). Regarding sleep latency, we found a U-shape association, suggesting that eating too far and too close to sleep increases its duration. Thus, the lowest sleep latency was observed when the last eating event occurred at ∼ 8 PM and ∼ 7 to 8 hours before the midpoint of sleep (b).
Discussion
As far as we are aware, this is the first Brazilian survey on chronobiological aspects related to sleep and eating behaviors, and also the first study to investigate the association of both clock time and circadian timing of evening eating with sleep quality and insomnia among Brazilian adults from the general population.
Our main findings were that both delaying the time of the last eating event, and its consumption closer to the midpoint of sleep were associated with worse sleep parameters. Each additional hour of the last eating event clock time and of the time between the last eating event and the midpoint of sleep, respectively, increased and decreased the odds of short sleep duration (by 30% and 49%), sleep latency > 30 min (by 14% and 12%), poor sleep quality (by 21% and 20%), and insomnia (by 12% and 11%). We found a dose-response association of evening eating (clock time and TEM) with sleep duration, and the shortest sleep latency was seen when the last eating event occurred at ∼ 8 PM and ∼ 7 to 8 hours before the midpoint of sleep.
Also, participants who reported dinner as the largest meal of the day and those who consumed caffeine and/or sugary foods/beverages after 6 PM presented higher odds of having sleep duration < 7 hours (respectively 51%, 34%, 94%), perceiving sleep quality as poor (respectively 52%, 33%, 25%) and having insomnia (all 35%). The odds for latency > 30 min were also 47% higher when dinner was the largest meal and 24% higher among those reporting evening consumption of sugary foods/beverages. These associations were independent of age, sex, region, physical exercise frequency, BMI, marital status, and scholarship.
Although there are no previous studies that have used TEM to analyze the effects of circadian eating timing on sleep, the study that first proposed it[31] was justified by the consequences of evening eating on circadian misalignment, previously highlighted by numerous experimental and observational studies.[25] [26] [34] [35] [36] [37] [38] [39]
Both evening eating and evening latency, defined as the duration of time between the last eating event and sleep onset, are part of chrononutritional behaviors that can misalign the phase of an individual's circadian rhythm and negatively influence health.[34] [35] Findings suggested that eating late and close to bedtime may contribute to poor sleep and misalignment of the melatonin phase,[22] [23] besides affecting weight, weight-related health outcomes such as insulin resistance, metabolic disease, and inflammation.[31] [35] [36] [37] [38] [39]
In a cross-sectional examination of the young Japanese population under free-living conditions, shortened time from dinner to bedtime was associated with prolonged sleep latency.[22] In a Brazilian study, healthy participants completed a 3-day food diary and underwent polysomnography, and findings showed that food intake within 30 to 60 minutes of bedtime was associated with delayed sleep onset and decreased sleep efficiency.[23]
Such studies, by emphasizing that eating high-calorie meals at the end of the day can contribute to poor sleep quality, may also justify the relationship we found between reporting dinner as the largest meal of the day and worse sleep parameters.
It is worth mentioning that the self-reported largest meal may have questionable accuracy, as demonstrated in previous studies, [34] [35] attributed to individuals' challenges in accurately estimating their caloric intake and their tendency to confuse the perception of plate size with the actual calories consumed. Nevertheless, overeating and consuming a substantial amount of food, regardless of its energy density, close to bedtime, can negatively impact sleep quality.[22] [23]
Regarding the association found between evening consumption of caffeinated food/beverages, similar results have been reported in the literature.[15] [40] In a review, Clark et al.[15] pointed out that caffeine consumed during the day can significantly reduce the total amount of sleep and lead to a decrease in sleep efficiency. Interestingly, one of the studies in this review[40] demonstrated that caffeine consumption in the morning can negatively impact nighttime sleep. A higher dose in the early morning (200 mg at 7:10) caused a significant reduction in sleep efficiency and total sleep duration when compared with placebo, although caffeine saliva concentrations approached zero when measured shortly before sleep.
Although caffeine provides immediate energy after consumption, some longer-lasting effects consequences alter sleep patterns for many hours after intake, including prolonged sleep latency, reduced total sleep time, sleep inefficiency, worsened perceived sleep quality, and rapid eye movement (REM) sleep behavior disorder.[15] [41] [42]
The linkage between sleep characteristics and evening sugar intake has not been largely studied, but findings from the existing literature indicate that consuming lower-quality carbohydrates negatively impacts sleep quality. Higher intakes of dietary added sugars, starch, and nonwhole/refined grains were each associated with higher odds of incident insomnia among postmenopausal women from the Women's Health Initiative Observational Study.[43] In the study by St-Onge et al.,[44] which assessed the impact of self-determined dietary intakes on sleep, nocturnal arousals were higher in participants consuming more sugar and more non-sugary/non-fiber carbohydrates (e.g., starches).
An investigation on middle-aged Japanese women found that a high intake of confectioneries and noodles (i.e., high glycemic index and simple carbohydrates) was associated with poor sleep quality.[20] Afaghi et al.[45] reported that the consumption of a high glycemic index evening meal was associated with a shorter sleep onset latency.
In a recent summary of extant research among adults, the odds of drinking soda in those with short sleep duration was 1.2 times higher than in those with sufficient sleep (OR: 1.20; 95% CI: 1.12, 1.28).[18] As mentioned before, insufficient sleep and circadian misalignment are important metabolic stressors, which can alter the levels of appetite hormones and promote unhealthier food choices, such as higher sugar intake, skipping breakfast, and delaying mealtimes.[46]
Although further research should be performed to clarify the causality and underlying mechanisms to explain the relationship between carbohydrate consumption and sleep, the most commonly proposed mechanisms refer to changes in the levels of brain tryptophan, serotonin, or melatonin.[47]
The influence of meal composition, both in terms of macro and micronutrients, meal size, and meal timing, must be explored in future studies to improve our understanding of the relationship between diet and sleep.
Strengths and Weaknesses
Our study has a few limitations, starting with the use of self-reported questionnaires, which are prone to underreporting or misreporting. Also, precise questions were used to investigate sleep domains; the questionnaire specified that responses should be based on recent behaviors (last month) and, to guarantee data as close as possible to the real usual behavior, the questionnaire differentiated weekdays (work/study days) and weekends (free days).[48]
Furthermore, although the survey questionnaire clarified that insomnia should have been diagnosed by a professional, we recognize as a limitation the use of self-reported insomnia. However, it is important to consider that even subjective perceptions of sleep disorders can capture nuances in symptoms and indicate the presence of sleep problems that might be affecting one's quality of life.
In addition, despite our covariate adjustment for sociodemographic, diet-related, and lifestyle traits, we recognize that a general weakness of cross-sectional studies is that the direction of the relationship, and possible pathways of causation, can only be hypothesized. Also, we recognize as a limitation the absence of energy and nutrient consumption data to assess differences in daily/evening intake between groups.
Conclusions
In conclusion, our results suggest that the timing of evening eating (both clock time and the midpoint of sleep-related time), the evening consumption of caffeine and sugary foods and having dinner as the largest meal of the day are associated with worse sleep parameters.
These findings tend to support evidence indicating that an early-eating schedule has beneficial sleep effects and that it will be necessary to consider components of chrononutrition, such as evening eating patterns, distribution, and timing, along with the existing sleep hygiene and circadian hygiene recommendations, to improve sleep quality and circadian health and to prevent and treat sleep disorders.
Finally, due to the novelty of our study, it is important to mention that the TEM parameter seems to be a good measure for studies on evening eating timing. Since it measures the elapsed time between the last eating event and the midpoint of sleep, which is considered a chronotype marker, it might also represent a proxy of circadian time.
Conflict of Interests
The authors have no conflict of interests to declare.
Author Contributions
Maria Eduarda Bezerra Nunes: Conceptualization; data curation; formal analysis; investigation; methodology; supervision; validation; roles/writing - original draft; writing - review & editing.
Caio Henrique Barros dos Santos: Conceptualization; data curation; formal analysis; investigation; methodology; supervision; validation; roles/writing - original draft; writing - review & editing.
Márcia de Oliveira Lima: Conceptualization; data curation; formal analysis; investigation; methodology; supervision; validation; roles/writing - original draft; writing - review & editing.
Anny Kariny Pereira Pedrosa: Methodology; roles/writing - original draft; writing - review & editing.
Risia Cristina Egito de Menezes: Methodology; roles/writing - original draft; writing - review & editing.
Giovana Longo-Silva: Conceptualization; data curation; formal analysis; investigation; methodology; project administration; supervision; validation; visualization; roles/writing - original draft; writing - review & editing.
-
References
- 1 Morin CM, Jarrin DC. Epidemiology of Insomnia: Prevalence, Course, Risk Factors, and Public Health Burden. Sleep Med Clin 2022; 17 (02) 173-191
- 2 Grandner MA. Epidemiology of insufficient sleep and poor sleep quality. Sleep Health 2019; 1 (02) 11-20
- 3 Walch OJ, Cochran A, Forger DB. A global quantification of “normal” sleep schedules using smartphone data. Sci Adv 2016; 2 (05) e1501705
- 4 Ohayon M, Wickwire EM, Hirshkowitz M. et al. National Sleep Foundation's sleep quality recommendations: first report. Sleep Health 2017; 3 (01) 6-19
- 5 Andreeva VA, Perez-Jimenez J, St-Onge MP. A Systematic Review of the Bidirectional Association Between Consumption of Ultra-processed Food and Sleep Parameters Among Adults. Curr Obes Rep 2023
- 6 van Egmond LT, Meth EMS, Engström J. et al. Effects of acute sleep loss on leptin, ghrelin, and adiponectin in adults with healthy weight and obesity: A laboratory study. Obesity (Silver Spring) 2023; 31 (03) 635-641
- 7 Tobaldini E, Fiorelli EM, Solbiati M, Costantino G, Nobili L, Montano N. Short sleep duration and cardiometabolic risk: from pathophysiology to clinical evidence. Nat Rev Cardiol 2019; 16 (04) 213-224
- 8 Nedeltcheva AV, Kilkus JM, Imperial J, Kasza K, Schoeller DA, Penev PD. Sleep curtailment is accompanied by increased intake of calories from snacks. Am J Clin Nutr 2009; 89 (01) 126-133
- 9 Taheri S, Lin L, Austin D, Young T, Mignot E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med 2004; 1 (03) e62
- 10 Imaki M, Hatanaka Y, Ogawa Y, Yoshida Y, Tanada S. An epidemiological study on relationship between the hours of sleep and life style factors in Japanese factory workers. J Physiol Anthropol Appl Human Sci 2002; 21 (02) 115-120
- 11 Wilson K, St-Onge MP, Tasali E. Diet Composition and Objectively Assessed Sleep Quality: A Narrative Review. J Acad Nutr Diet 2022; 122 (06) 1182-1195
- 12 Weibel J, Lin YS, Landolt HP. et al. The impact of daily caffeine intake on nighttime sleep in young adult men. Sci Rep 2021; 11 (01) 4668
- 13 Fredholm BB, Bättig K, Holmén J, Nehlig A, Zvartau EE. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev 1999; 51 (01) 83-133
- 14 Landolt HP. Sleep homeostasis: a role for adenosine in humans?. Biochem Pharmacol 2008; 75 (11) 2070-2079
- 15 Clark I, Landolt HP. Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep Med Rev 2017; 31: 70-78
- 16 St-Onge MP, Roberts A, Shechter A, Choudhury AR. Fiber and saturated fat are associated with sleep arousals and slow wave sleep. J Clin Sleep Med 2016; 12 (01) 19-24
- 17 Boozari B, Saneei P, Safavi SM. Association between sleep duration and sleep quality with sugar and sugar-sweetened beverages intake among university students. Sleep Breath 2021; 25 (02) 649-656
- 18 Shahdadian F, Boozari B, Saneei P. Association between short sleep duration and intake of sugar and sugar-sweetened beverages: A systematic review and meta-analysis of observational studies. Sleep Health 2023; 9 (02) 159-176
- 19 Spaeth AM, Dinges DF, Goel N. Objective measurements of energy balance are associated with sleep architecture in healthy adults. Sleep 2017; 40 (01) zsw018
- 20 Katagiri R, Asakura K, Kobayashi S, Suga H, Sasaki S. Low intake of vegetables, high intake of confectionary, and unhealthy eating habits are associated with poor sleep quality among middle-aged female Japanese workers. J Occup Health 2014; 56 (05) 359-368
- 21 Chaudhary NS, Grandner MA, Jackson NJ, Chakravorty S. Caffeine consumption, insomnia, and sleep duration: Results from a nationally representative sample. Nutrition 2016; 32 (11-12): 1193-1199
- 22 Yasuda J, Kishi N, Fujita S. Association between Time from Dinner to Bedtime and Sleep Quality Indices in the Young Japanese Population: A Cross-Sectional Study. Dietetics. 2023; 2: 140-149
- 23 Crispim CA, Zimberg IZ, dos Reis BG, Diniz RM, Tufik S, de Mello MT. Relationship between food intake and sleep pattern in healthy individuals. J Clin Sleep Med 2011; 7 (06) 659-664
- 24 Duan D, Gu C, Polotsky VY, Jun JC, Pham LV. Effects of Dinner Timing on Sleep Stage Distribution and EEG Power Spectrum in Healthy Volunteers. Nat Sci Sleep 2021; 13: 601-612
- 25 Lopez-Minguez J, Gómez-Abellán P, Garaulet M. Timing of Breakfast, Lunch, and Dinner. Effects on Obesity and Metabolic Risk. Nutrients 2019; 11 (11) 2624
- 26 Longo-Silva G, Pedrosa AKP, de Oliveira PMB. et al. Beyond sleep duration: Sleep timing is associated with BMI among Brazilian adults. Sleep Med X 2023; 6 (15) 100082
- 27 Longo-Silva G, Bezerra de Oliveira PM, Pedrosa AKP. et al. Breakfast skipping and timing of lunch and dinner: Relationship with BMI and obesity. Obes Res Clin Pract 2022; 16 (06) 507-513
- 28 Keijzer H, Smits MG, Duffy JF, Curfs LM. Why the dim light melatonin onset (DLMO) should be measured before treatment of patients with circadian rhythm sleep disorders. Sleep Med Rev 2014; 18 (04) 333-339
- 29 Lopez-Minguez J, Saxena R, Bandín C, Scheer FA, Garaulet M. Late dinner impairs glucose tolerance in MTNR1B risk allele carriers: A randomized, cross-over study. Clin Nutr 2018; 37 (04) 1133-1140
- 30 McHill AW, Phillips AJK, Czeisler CA. et al. Later circadian timing of food intake is associated with increased body fat. Am J Clin Nutr 2017; 106 (05) 1213-1219
- 31 Zerón-Rugerio MF, Longo-Silva G, Hernáez Á, Ortega-Regules AE, Cambras T, Izquierdo-Pulido M. The Elapsed Time between Dinner and the Midpoint of Sleep is Associated with Adiposity in Young Women. Nutrients 2020; 12 (02) 410
- 32 Roenneberg T, Pilz LK, Zerbini G, Winnebeck EC. Chronotype and Social Jetlag: A (Self-) Critical Review. Biology (Basel) 2019; 8 (03) 54
- 33 Roenneberg T, Wirz-Justice A, Merrow M. Life between clocks: daily temporal patterns of human chronotypes. J Biol Rhythms 2003; 18 (01) 80-90
- 34 Lira NCC, de Araújo SM, de Medeiros ACQ, de Souza JC. Translation, adaptation and validation of the Chrononutrition Profile - Questionnaire (CP-Q) in Brazilian Portuguese. Chronobiol Int 2023; 40 (04) 473-482
- 35 Veronda AC, Allison KC, Crosby RD, Irish LA. Development, validation and reliability of the Chrononutrition Profile - Questionnaire. Chronobiol Int 2020; 37 (03) 375-394
- 36 WHO. Obesity and Overweight. Geneva, Switzerland: World Health Organization; 2017
- 37 Xiao Q, Garaulet M, Scheer FAJL. Meal timing and obesity: interactions with macronutrient intake and chronotype. Int J Obes 2019; 43 (09) 1701-1711
- 38 Piesman M, Hwang I, Maydonovitch C, Wong RK. Nocturnal reflux episodes following the administration of a standardized meal. Does timing matter?. Am J Gastroenterol 2007; 102 (10) 2128-2134
- 39 Yoshitake R, Park I, Ogata H, Omi N. Meal Timing and Sleeping Energy Metabolism. Nutrients 2023; 15 (03) 763
- 40 Landolt HP, Werth E, Borbély AA, Dijk DJ. Caffeine intake (200 mg) in the morning affects human sleep and EEG power spectra at night. Brain Res 1995; 675 (1-2): 67-74
- 41 McLellan TM, Caldwell JA, Lieberman HR. A review of caffeine's effects on cognitive, physical and occupational performance. Neurosci Biobehav Rev 2016; 71: 294-312
- 42 Roehrs T, Roth T. Caffeine: sleep and daytime sleepiness. Sleep Med Rev 2008; 12 (02) 153-162
- 43 Gangwisch JE, Hale L, St-Onge MP. et al. High glycemic index and glycemic load diets as risk factors for insomnia: analyses from the Women's Health Initiative. Am J Clin Nutr 2020; 111 (02) 429-439
- 44 St-Onge MP, Mikic A, Pietrolungo CE. Effects of Diet on Sleep Quality. Adv Nutr 2016; 7 (05) 938-949
- 45 Afaghi A, O'Connor H, Chow CM. High-glycemic-index carbohydrate meals shorten sleep onset. Am J Clin Nutr 2007; 85 (02) 426-430
- 46 Chaput JP, McHill AW, Cox RC. et al. The role of insufficient sleep and circadian misalignment in obesity. Nat Rev Endocrinol 2023; 19 (02) 82-97
- 47 Benton D, Bloxham A, Gaylor C, Brennan A, Young HA. Carbohydrate and sleep: An evaluation of putative mechanisms. Front Nutr 2022; 9: 933898
- 48 Robbins R, Quan SF, Barger LK. et al. Self-reported sleep duration and timing: A methodological review of event definitions, context, and timeframe of related questions. Sleep Epidemiol 2021; 1: 100016
Address for correspondence
Publication History
Received: 14 August 2023
Accepted: 13 December 2023
Article published online:
23 February 2024
© 2024. Brazilian Sleep Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Morin CM, Jarrin DC. Epidemiology of Insomnia: Prevalence, Course, Risk Factors, and Public Health Burden. Sleep Med Clin 2022; 17 (02) 173-191
- 2 Grandner MA. Epidemiology of insufficient sleep and poor sleep quality. Sleep Health 2019; 1 (02) 11-20
- 3 Walch OJ, Cochran A, Forger DB. A global quantification of “normal” sleep schedules using smartphone data. Sci Adv 2016; 2 (05) e1501705
- 4 Ohayon M, Wickwire EM, Hirshkowitz M. et al. National Sleep Foundation's sleep quality recommendations: first report. Sleep Health 2017; 3 (01) 6-19
- 5 Andreeva VA, Perez-Jimenez J, St-Onge MP. A Systematic Review of the Bidirectional Association Between Consumption of Ultra-processed Food and Sleep Parameters Among Adults. Curr Obes Rep 2023
- 6 van Egmond LT, Meth EMS, Engström J. et al. Effects of acute sleep loss on leptin, ghrelin, and adiponectin in adults with healthy weight and obesity: A laboratory study. Obesity (Silver Spring) 2023; 31 (03) 635-641
- 7 Tobaldini E, Fiorelli EM, Solbiati M, Costantino G, Nobili L, Montano N. Short sleep duration and cardiometabolic risk: from pathophysiology to clinical evidence. Nat Rev Cardiol 2019; 16 (04) 213-224
- 8 Nedeltcheva AV, Kilkus JM, Imperial J, Kasza K, Schoeller DA, Penev PD. Sleep curtailment is accompanied by increased intake of calories from snacks. Am J Clin Nutr 2009; 89 (01) 126-133
- 9 Taheri S, Lin L, Austin D, Young T, Mignot E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med 2004; 1 (03) e62
- 10 Imaki M, Hatanaka Y, Ogawa Y, Yoshida Y, Tanada S. An epidemiological study on relationship between the hours of sleep and life style factors in Japanese factory workers. J Physiol Anthropol Appl Human Sci 2002; 21 (02) 115-120
- 11 Wilson K, St-Onge MP, Tasali E. Diet Composition and Objectively Assessed Sleep Quality: A Narrative Review. J Acad Nutr Diet 2022; 122 (06) 1182-1195
- 12 Weibel J, Lin YS, Landolt HP. et al. The impact of daily caffeine intake on nighttime sleep in young adult men. Sci Rep 2021; 11 (01) 4668
- 13 Fredholm BB, Bättig K, Holmén J, Nehlig A, Zvartau EE. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol Rev 1999; 51 (01) 83-133
- 14 Landolt HP. Sleep homeostasis: a role for adenosine in humans?. Biochem Pharmacol 2008; 75 (11) 2070-2079
- 15 Clark I, Landolt HP. Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep Med Rev 2017; 31: 70-78
- 16 St-Onge MP, Roberts A, Shechter A, Choudhury AR. Fiber and saturated fat are associated with sleep arousals and slow wave sleep. J Clin Sleep Med 2016; 12 (01) 19-24
- 17 Boozari B, Saneei P, Safavi SM. Association between sleep duration and sleep quality with sugar and sugar-sweetened beverages intake among university students. Sleep Breath 2021; 25 (02) 649-656
- 18 Shahdadian F, Boozari B, Saneei P. Association between short sleep duration and intake of sugar and sugar-sweetened beverages: A systematic review and meta-analysis of observational studies. Sleep Health 2023; 9 (02) 159-176
- 19 Spaeth AM, Dinges DF, Goel N. Objective measurements of energy balance are associated with sleep architecture in healthy adults. Sleep 2017; 40 (01) zsw018
- 20 Katagiri R, Asakura K, Kobayashi S, Suga H, Sasaki S. Low intake of vegetables, high intake of confectionary, and unhealthy eating habits are associated with poor sleep quality among middle-aged female Japanese workers. J Occup Health 2014; 56 (05) 359-368
- 21 Chaudhary NS, Grandner MA, Jackson NJ, Chakravorty S. Caffeine consumption, insomnia, and sleep duration: Results from a nationally representative sample. Nutrition 2016; 32 (11-12): 1193-1199
- 22 Yasuda J, Kishi N, Fujita S. Association between Time from Dinner to Bedtime and Sleep Quality Indices in the Young Japanese Population: A Cross-Sectional Study. Dietetics. 2023; 2: 140-149
- 23 Crispim CA, Zimberg IZ, dos Reis BG, Diniz RM, Tufik S, de Mello MT. Relationship between food intake and sleep pattern in healthy individuals. J Clin Sleep Med 2011; 7 (06) 659-664
- 24 Duan D, Gu C, Polotsky VY, Jun JC, Pham LV. Effects of Dinner Timing on Sleep Stage Distribution and EEG Power Spectrum in Healthy Volunteers. Nat Sci Sleep 2021; 13: 601-612
- 25 Lopez-Minguez J, Gómez-Abellán P, Garaulet M. Timing of Breakfast, Lunch, and Dinner. Effects on Obesity and Metabolic Risk. Nutrients 2019; 11 (11) 2624
- 26 Longo-Silva G, Pedrosa AKP, de Oliveira PMB. et al. Beyond sleep duration: Sleep timing is associated with BMI among Brazilian adults. Sleep Med X 2023; 6 (15) 100082
- 27 Longo-Silva G, Bezerra de Oliveira PM, Pedrosa AKP. et al. Breakfast skipping and timing of lunch and dinner: Relationship with BMI and obesity. Obes Res Clin Pract 2022; 16 (06) 507-513
- 28 Keijzer H, Smits MG, Duffy JF, Curfs LM. Why the dim light melatonin onset (DLMO) should be measured before treatment of patients with circadian rhythm sleep disorders. Sleep Med Rev 2014; 18 (04) 333-339
- 29 Lopez-Minguez J, Saxena R, Bandín C, Scheer FA, Garaulet M. Late dinner impairs glucose tolerance in MTNR1B risk allele carriers: A randomized, cross-over study. Clin Nutr 2018; 37 (04) 1133-1140
- 30 McHill AW, Phillips AJK, Czeisler CA. et al. Later circadian timing of food intake is associated with increased body fat. Am J Clin Nutr 2017; 106 (05) 1213-1219
- 31 Zerón-Rugerio MF, Longo-Silva G, Hernáez Á, Ortega-Regules AE, Cambras T, Izquierdo-Pulido M. The Elapsed Time between Dinner and the Midpoint of Sleep is Associated with Adiposity in Young Women. Nutrients 2020; 12 (02) 410
- 32 Roenneberg T, Pilz LK, Zerbini G, Winnebeck EC. Chronotype and Social Jetlag: A (Self-) Critical Review. Biology (Basel) 2019; 8 (03) 54
- 33 Roenneberg T, Wirz-Justice A, Merrow M. Life between clocks: daily temporal patterns of human chronotypes. J Biol Rhythms 2003; 18 (01) 80-90
- 34 Lira NCC, de Araújo SM, de Medeiros ACQ, de Souza JC. Translation, adaptation and validation of the Chrononutrition Profile - Questionnaire (CP-Q) in Brazilian Portuguese. Chronobiol Int 2023; 40 (04) 473-482
- 35 Veronda AC, Allison KC, Crosby RD, Irish LA. Development, validation and reliability of the Chrononutrition Profile - Questionnaire. Chronobiol Int 2020; 37 (03) 375-394
- 36 WHO. Obesity and Overweight. Geneva, Switzerland: World Health Organization; 2017
- 37 Xiao Q, Garaulet M, Scheer FAJL. Meal timing and obesity: interactions with macronutrient intake and chronotype. Int J Obes 2019; 43 (09) 1701-1711
- 38 Piesman M, Hwang I, Maydonovitch C, Wong RK. Nocturnal reflux episodes following the administration of a standardized meal. Does timing matter?. Am J Gastroenterol 2007; 102 (10) 2128-2134
- 39 Yoshitake R, Park I, Ogata H, Omi N. Meal Timing and Sleeping Energy Metabolism. Nutrients 2023; 15 (03) 763
- 40 Landolt HP, Werth E, Borbély AA, Dijk DJ. Caffeine intake (200 mg) in the morning affects human sleep and EEG power spectra at night. Brain Res 1995; 675 (1-2): 67-74
- 41 McLellan TM, Caldwell JA, Lieberman HR. A review of caffeine's effects on cognitive, physical and occupational performance. Neurosci Biobehav Rev 2016; 71: 294-312
- 42 Roehrs T, Roth T. Caffeine: sleep and daytime sleepiness. Sleep Med Rev 2008; 12 (02) 153-162
- 43 Gangwisch JE, Hale L, St-Onge MP. et al. High glycemic index and glycemic load diets as risk factors for insomnia: analyses from the Women's Health Initiative. Am J Clin Nutr 2020; 111 (02) 429-439
- 44 St-Onge MP, Mikic A, Pietrolungo CE. Effects of Diet on Sleep Quality. Adv Nutr 2016; 7 (05) 938-949
- 45 Afaghi A, O'Connor H, Chow CM. High-glycemic-index carbohydrate meals shorten sleep onset. Am J Clin Nutr 2007; 85 (02) 426-430
- 46 Chaput JP, McHill AW, Cox RC. et al. The role of insufficient sleep and circadian misalignment in obesity. Nat Rev Endocrinol 2023; 19 (02) 82-97
- 47 Benton D, Bloxham A, Gaylor C, Brennan A, Young HA. Carbohydrate and sleep: An evaluation of putative mechanisms. Front Nutr 2022; 9: 933898
- 48 Robbins R, Quan SF, Barger LK. et al. Self-reported sleep duration and timing: A methodological review of event definitions, context, and timeframe of related questions. Sleep Epidemiol 2021; 1: 100016