

Subscribe to RSS
DOI: 10.1055/s-0043-1776285
Intranasal Glioma with Post-Endoscopic Resection in 1 Year Old Infant: Case Report and Literature Review*
Glioma intranasal com ressecção pós-endoscópica em bebê de 1 ano: Relato de caso e revisão da literaturaAuthors
Funding Nenhum financiamento direcionado foi relatado.


Abstract
Introduction Nasal gliomas - or nasal glial heterotopias - are rare congenital malformations, which correspond to 5% of the congenital nasal masses. It is a mass composed of mature glial tissue that can be located outside, inside or near the nasal region, and may or may not be connected to the brain by a fibrous pedicle. This report addresses a case of nasal glioma that suffered recurrence after endoscopic treatment.
Case Report A 1-year-old boy has, since birth, a mass inside the left nostril, which obstructs and widens the bridge of the nose. Upon physical examination, it is observed that the mass does not increase in size with crying and presents negative transluminescence and Furstenberg test. Upon being biopsied, the lesion reveals malignancy and the presence of inflammatory cells. MRI ruled out communication with intracranial structures. The endoscopic resection of the heterotopia removed a mass of 3,0 × 2,5 × 1,7 cm, whose histological and immunohistochemical analysis revealed glial pattern cell proliferation in the nasal mucosa.
Conclusion Considering that nasal glial heterotopy is frequently present at birth, and that newborns breathe predominantly through this route, early diagnosis of the lesion is of great importance, as it can cause signs and symptoms of respiratory distress. In addition, it is worth noting that the early approach also prevents bone deformities.
Resumo
Introdução Os gliomas nasais – ou heterotopias gliais nasais – são malformações congênitas raras, que correspondem a 5% das massas nasais congênitas. Trata-se de uma massa composta por tecido glial maduro que pode se localizar no exterior, no interior ou nas proximidades da região nasal, podendo ou não estar conectado ao cérebro por um pedículo fibroso. Este relato aborda um caso de glioma nasal que sofreu recidiva após tratamento por via endoscópica.
Relato do caso Um menino de 1 ano de idade apresenta, desde o nascimento, massa no interior da narina esquerda, a qual obstrui e alarga a ponte do nariz. Ao exame físico, observa-se que a massa não aumenta de tamanho com o choro e apresenta transluminescência e teste de Furstenberg negativos. Ao ser biopsiada, a lesão revela malignidade e presença de células inflamatórias. A ressonância magnética descartou comunicação com estruturas intracranianas. A ressecção endoscópica da heterotopia removeu uma massa de 3,0 × 2,5 × 1,7 cm, cujas análise histológica e imuno-histoquímica revelaram proliferação celular de padrão glial em mucosa nasal.
Conclusão Considerando que a heterotopia glial nasal frequentemente se encontra presente ao nascimento, e que os recém-natos respiram predominantemente por essa via, é de grande importância o diagnóstico precoce da lesão, já que ela pode causar sinais e sintomas de desconforto respiratório. Além disso, vale destacar que a abordagem precoce também previne deformidades ósseas.
Keywords
nasal glioma - congenital malformations - endoscopic resection - respiratory stress - bone deformitiesPalavras-chave
glioma nasal - malformações congênitas - ressecção endoscópica - estresse respiratório - deformidades ósseasIntroduction
Nasal gliomas are rare congenital malformations, which correspond to 5% of the congenital nasal masses, first described by Reid in 1852 and called “glioma” by Schmidt in 1900. Black and Smith, in 1950, defined nasal glioma as a congenital extracranial mass of mature glial tissue that can be located outside, inside the nasal cavity, in both, or near the root of the nose. The glioma may or may not be connected to the brain by a pedicle of glial tissue, it does not contain a fluid-filled space connecting it to the cerebral ventricles or the subarachnoid space. Thus, these tumors consist of remnants of neuroglial tissue that are among the differential diagnoses of congenital midline nasal masses.[1] [2] [3] [4] [5] [6] [7]
Congenital malformations are often present at birth, even if diagnosed later. Encephalocele is the most frequent midline congenital nasal mass, followed by dermoid cysts, epidermoid cysts, gliomas, teratoma and hemangiomas.[7] [8] The differentiation of glioma in relation to encephalocele is of great importance, since the extracranial management of encephaloceles can increase the risk of meningitis.[6] Nasal gliomas are, therefore, of neurogenic origin and are part of the spectrum of anomalies in the development of the central nervous system, particularly neural crest cells.[1] [9]
The most accepted theory regarding the emergence of nasal glioma is that of herniation of the tissue through the fonticulus frontalis of the foramen cecum displaced by the closure of the anterior neuropore, during the development of the skull base.[10] Some researchers define nasal glioma as an encephalocele that has lost its connection with intracranial contents. Thus, the encephalocele would be a protrusion of the cerebral content connected to the rest of the brain by a pedicle, associated with a bone defect, while the nasal glial heterotopia has no communication with the subarachnoid space or with the central nervous system.[4] [11] [12]
Bearing in mind that the heterotopic tissue represents a histologically normal tissue in an atypical location, many authors argue that the name “glioma” is not appropriate, as it is given to a neoplasm of the same constitution. For this reason, it can also be called nasal glial heterotopy.[13]
Heterotopy has an approximate incidence of one case for every 20.000 to 40.000 live births and is considered benign but can cause deformities due to its slow growth.[3] [7] [9] [11] [14] [15] Some authors report that there is no gender predominance, while others believe that the anomaly is more common in boys (3:2). There is no family predisposition.[3] [10]
On clinical examination, the consistency of the glioma is usually firm and can be seen as a polypoid structure in the nasal cavity. It is a mass with negative transluminescence and that does not increase with compression of the jugular vein - negative Furstenberg sign.[3] [13] As for their location, 60% of the gliomas are extranasal, 20% are intranasal and 10%, mixed. Extranasals are typically lateral to the midline and can result in visual and tear changes on the affected side. There may be hypertelorism. Intranasal gliomas are firm, pale masses that can obstruct and lead to breathing difficulties, deviated septum, epistaxis or nasal congestion. They are most commonly from the lateral nasal wall. The septum and nasal bones are often displaced. Because of the obstruction due to the presence of the mass, there may be symptoms of respiratory stress.[3] [6] [11] Unlike gliomas, encephaloceles are deformable and pulsatile, increase with effort and crying and have a positive Furstenberg signal.[3]
Magnetic resonance imaging (MRI) is considered the exam of choice for the evaluation. The diagnosis can be made in the pre- or post-natal period, with 60% of cases being diagnosed in the neonatal period. Although most commonly found in children, they can also be present in adults. Mass biopsy and aspiration are contraindicated due to the risk of meningitis or loss of functional brain tissue in an encephalocele. Its treatment is complete surgical resection, which can prevent complications such as meningitis, intracranial abscess and facial deformities.[4] [6] [7] [10] [15] Histologically, the tumor is characterized by the presence of nerve fibers intertwined with fibrous and vascular connective tissue. Neurons and astrocytes can be identified in some lesions. The arrangement is usually lobular and cystic structures may be present.[4]
Case Report
A 1-year-old male patient was referred to the service for a cyst in the nasal region. The mother says that the change was already present at birth. The patient was born by cesarean delivery, of a twin pregnancy, with a gestational age of 27 weeks, having remained in the neonatal intensive care unit (ICU) for ∼2 months. His corrected chronological age was 9 months and two days. The mother reports breastfeeding up to five months of age, supplemented with NAN without lactose. She also reports an updated vaccination schedule. Two months before the appointment, he had been admitted for bacterial meningitis. On physical examination, an expansive nasal cavity mass, which was not enlarged with crying or exertion, with negative transluminescence and with a negative Furstenberg test, was noticed. The lesion was benign in appearance, but the possibility of esthesioneuroblastoma was considered.
A computed tomography (CT) scan of the sinus of the face ([Fig. 1]) showed an expansive lesion with a density of soft tissues widening and obliterating the left nasal cavity, measuring 20 mm, of undetermined nature, without associated bone destruction or communication with the central nervous system. An incisional endoscopic biopsy of the lesion was then proposed. The histological study was negative for malignancy and indicated the presence of inflammatory tissue, raising the hypothesis of angiofibroma. The patient presented bronchospasm after extubation, requiring inhalation of adrenaline and dexamethasone.
Two months after the biopsy, the mother reports an increase in the tumor, followed by spontaneous reduction. She reports an episode of epistaxis after surgery. Then, it was proposed to perform an MRI examination of the face, to better assess the presence or absence of mass communication with intracranial content. MRI revealed an expansive heterogeneous solid nodular lesion in the left lateral wall and back of the nose, which protrudes and obliterates the left nasal cavity and measures ∼3,0 × 2,5 × 1,7 cm, with nonspecific characteristics that differed from the hemangioma. The lesion has no intracranial connection. On physical examination, there was an increase in volume in the nasal bridge and obstruction of the left nostril with mass.
Nine months after MRI, microsurgery was performed to resect the nasal cavity / skull base tumor by endoscopy, without complications. The expansive lesion originated in the lateral nasal wall and extended to the floor of the orbit. The histological diagnosis was of cell proliferation of the glial pattern in the nasal mucosa. Immunohistochemistry ([Fig. 2]) demonstrated the positivity of glial fibrillary acid protein (GFAP), S-100 positive protein and Ki-67 positive in 1% of the neoplastic cell nuclei. The pattern of markers corroborated for the diagnosis of glial heterotopia (nasal glioma).

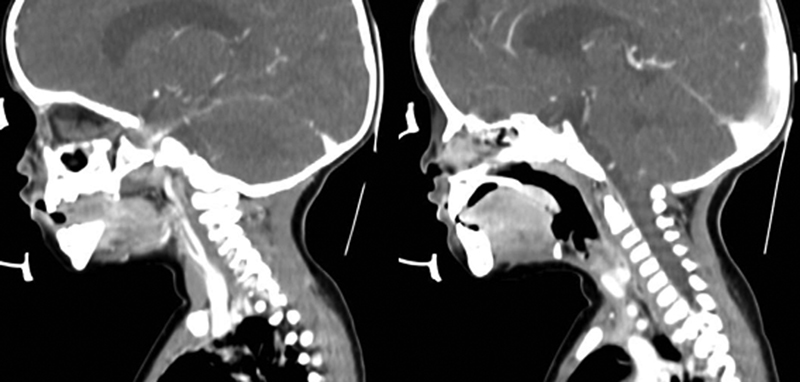
After two years of follow-up of the case, a CT scan of the face ([Fig. 3]) revealed a soft tissue lesion measuring 15 × 16 mm, located in the anterior portion of the left nasal fossa (middle / upper third) with infiltrate and thickening of the septum nasal, determining adjacent bone erosion, in addition to the presence of soft part components in the associated nasal dorsal subcutaneous. The images indicated a recurrence of the lesion, which had been resected by nasal endoscopy about a year ago. Skull CT performed in the same circumstances did not reveal any abnormalities. Another MRI scan ([Fig. 4]) made one year after the last one, during the follow-up, showed persistence of the lesion and led to the indication of a surgical procedure for removal. The removal was successful, and the patient did not experience new relapses since then.


Discussion
Nasal glioma is an anomaly of neurogenic origin with no potential for malignancy with ∼300 cases reported in the literature, corresponding to ∼5% of congenital nasal masses. The lesion consists of normal brain tissue and fibrous bands that can connect to the internal part of the skull in 15 to 20% of cases, which develop with a bone defect at the base of the skull.[1] [2] [3] [6] [8] [10] [16] Their growth rate is usually the same as that of adjacent tissues, but they have the potential to produce bone deformities.[1]
Intranasal gliomas are less frequent and come from the middle turbinate or the lateral nasal wall, which is common to nasal polyps. The latter are the ones with the most intracranial connection, which occurs in 35% of cases.[2] [5] [7] [10] [15] [16] [17]
Also called glial nasal heterotopy, due to the non-neoplastic nature of the lesion, gliomas are not considered hereditary. Some authors believe there is a predilection for the tumor in males, in a ratio of 3:2.[2] [3] [7] [13]
The etiology of nasal gliomas is not well defined. There are four theories that could explain its appearance: sequestration of glial tissue from the olfactory bulb during fusion of the cribiform plaque - which would not explain the emergence of the encephalocele -, ectopic cells of neural tissue, encephaloceles with lost intracranial connection and meningeal continuity and inappropriate closure of the anterior neuropore (the fonticulus frontalis), however, the most accepted theory is that the glioma represents an encephalocele sequestered from intracranial brain content at the beginning of pregnancy.[2] [6] [8] This latter theory is called the pre-nasal space theory, and was first described by Grumwald in 1910.[11]
At the end of the 2nd month of embryogenesis, a small fontanelle - the fonticulus frontalis - appears, located between the nasal and frontal bones. There is also the pre-nasal space, located between the nasal bones and the nasal cartilage capsule, which extends from the base of the skull to the nasal apex. In the same period, a dura mater diverticulum (with or without arachnoid or neural tissue) protrudes anteriorly through the fonticulus frontalis and / or inferiorly through the pre-nasal space. This diverticulum can contact and adhere to the skin. Normally, this diverticulum regresses over time and the bone then closes, creating the nasofrontal suture and foramen cecum (a small channel that passes through the base of the skull before the galli crest). A defect in the regression of this diverticulum can leave ectodermal tissue in this path, preventing complete bone closure at this location, keeping the foramen cecum enlarged and distorting the crista galli. Depending on the patency of this diverticulum and its content, the resulting lesion may be a dermoid cyst, a glioma or an encephalocele, which are the nasal masses with the potential to link with the central nervous system.[1] [5] [7] [8] [9] [14] [15] [17]
Encephalocele has the same embryological origin as nasal glioma and is an important differential diagnosis between nasal masses.[2] Encephaloceles have an incidence of one in 3.000 live births and are caused by herniation of neural tissue through defects in the skull, which may contain brain tissue and meninges or just meninges. They can communicate with the ventricular system and are always associated with a significant defect at the base of the skull. In 40% of cases, patients have other associated abnormalities. Most encephaloceles are located later, but 15 to 20% are anterior. The clinical characteristics of encephaloceles are of a soft and flexible mass, which increases with effort or crying and with a positive Furstenberg sign, with positive transluminescence. Encephaloceles can develop with CSF rhinorrhea and meningitis. Gliomas are considered encephaloceles that have lost their connection with the meninges of the intracranial space sarcomas.[9] [12] [13] [15] [16] [17] [18]
Dermoid cysts are also a relevant differential diagnosis. They are connected to intracranial content in 26 to 30% of cases, with an incidence of one in 6.000 live births. These are sinus tracts or cavities that have an epithelial lining and a variable number of cutaneous appendages, including hair follicles and glands. Cysts are usually solid and have no pulse. The negative transillumination test can differentiate you from meningocele. It is important to note that ∼4 to 45% of the cysts contain intracranial content.[10]
Capillary hemangiomas, another differential diagnosis to be considered, present themselves as reddish masses with a surface with telangectasis - differentiation must be made through Doppler ultrasonography, since hemangiomas have a higher systolic blood peak than gliomas. Other differential diagnoses include sebaceous cysts, epidermoid cysts, papillomas, inflammatory nasal polyps - extremely rare in children -, carcinomas, lipomas, fibromas, meningiomas, lymphomas and sarcomas.[6] [8] [9] [13] [14] [15] [16] [17] [18]
Gliomas are more commonly identified at birth, but their diagnosis can also be made during a later stage of childhood or even in adulthood.[2] [16] This type of congenital nasal mass is not associated with other anomalies, in most cases, but it can develop with cleft lip and palate, choanal atresia, hydrocephalus, urethral duplication and supernumerary finger.[1] [5] [15] [16]
The form of presentation of the lesion depends on its location. Clinically, the masses are of firm consistency, non-compressible, non-pulsatile, with negative transluminescence and of a gray or purple color. The Furstenberg sign must be negative. The patient with intranasal glioma may present nasal obstruction, epistaxis, cerebrospinal fluid rhinorrhea, nasolacrimal duct obstruction, hypertelorism and bone deformities. When they produce protrusion through the nostril, they can be confused with nasal polyps.[1] [4] [8] [15] [16]
Bearing in mind that newborns are mandatory nasal breathers and that upper airway obstruction at delivery has been described among patients with nasal and nasopharyngeal gliomas, prenatal MRI imaging in the presence of suspicion is paramount for that the appropriate intervention is made at the time of birth.[7] [11]
In cases of extranasal gliomas, the masses appear between the tip of the nose and the eyebrow and there may be bone deformities, hypertelorism, visual or lacrimal changes and the growth of a mass somewhere on the face.[1] [2] [7] [16] In 5% of cases, glioma can occupy other locations, such as scalp, cheek, soft palate, tonsil, medical ear, nasopharynx, oropharynx, submandibular region and orbit.[7] [15]
Surgical resection of the mass is the treatment of choice, since gliomas are not sensitive to radiation therapy. When incomplete, it results in recurrence in ∼4 to 10% of cases, which may justify the use of intraoperative freezing, to define surgical margins. Therefore, in order for the excision to be the best possible, an adequate evaluation is essential to define the site, extent and content of the tumor.[1] [2] [3] [7] [8] [9] [15] [16] [18]
Prenatal ultrasound can raise the diagnostic suspicion by revealing a solid frontonasal mass, with a final diastolic characteristic of low arterial flow velocity on Doppler.[3] [6] [10] [14] MRI is considered the best exam for the analysis of nasal glioma, as it shows in detail the soft tissues and the possibility of intracranial connection, in addition to not using radiation. Sometimes, herniation of meninges alone (meningocele) or brain and meninges (encephalocele) is evident. Contrast images should be obtained to assist in the differential diagnosis of solid masses or when infection is suspected. Computed tomography (CT) is useful in checking bone defects and in assessing the nasal roof.[1] [2] [3] [5] [6] [7] [8] [9] [11] [15] [16] [18] When viewed through CT, the tumor mass is the same density as brain tissue. Through MRI, the lesion is isointense to hypointense in relation to the gray matter in T1-weighted images and hyperintense and heterogeneous in T2-weighted images and proton density sequence.[7] [10] [16] Some imaging findings that should be investigated among patients with a midline nasal mass are: enlargement of the nasal bones, enlargement of the nasal septum, nasal septum, bifid perpendicular plaque, galli bifida crest, interorbital enlargement, cribiform lamina defects and extension of the mass intracranially.[15] Since ∼10 to 20% of nasal gliomas connect to intracranial structures through a fibrous band, it is unlikely that the size of the foramen cecum is likely to be useful to differentiate nasal gliomas from dermoid and encephalocele cysts.[1] [4]
In view of the possibility of mass communication with brain tissue, any preoperative biopsy should be avoided, as it may cause spillage of cerebrospinal fluid, formation of fistula and meningitis. If there is no evidence of an intracranial glioma, a conservative extracranial approach should be performed early - preferably in the first year of life, due to the risk of developing bone deformities or secondary infection. In general, the surgical approach should be based on the location and size of the mass, bone or associated cartilage deformity and, most importantly, the surgeon's experience. Transnasal endoscopic resection is widely used for this purpose, since it allows precise excision with minimal trauma to adjacent tissues. The endoscopic examination can also be easily used for follow-up. In the presence of intracranial extension, frontal craniotomy is indicated, in addition to the multidisciplinary approach, involving otolaryngology, neurosurgery and neuroradiology.[1] [2] [3] [7] [8] [9] [14] [15] [16] [17] Macroscopically, differentiating the glioma from brain tissue is difficult in the presence of a mass filament. In these cases, broad resection and repair of the bone defect with dural graft, bone wax or methacrylate are considered1. For extranasal gliomas, an external incision must be performed (lateral rhinotomy, open rhinoplasty, midline incision or bicoronal incision). A conservative and aesthetic incision is recommended, since the glioma is benign and recurrence is rare.[7] [8]
The largest series of cases of nasal glioma ever reported was published by Rahbar et al, who described 9 cases in infants during 32 years of study. Five patients underwent intra or transnasal excision. Among the four patients with extranasal gliomas, two external rhinoplasties, a lateral rhinotomy and a median rhinotomy were performed.[17]
The diagnosis is confirmed by histological evaluation, through which a mass without capsule is identified, with mature astrocytic cells of eosinophilic cytoplasm with varying proportion of fibrous and vascular connective tissue, which can be covered by skin or nasal respiratory mucosa. Mitoses are often absent. There may be malignant histological features similar to those of astrocytoma, but there is no potential for malignancy. The presence of leptomeninges, ependyma and choroid plexus are compatible with the diagnosis of encephalocele. In 40% of cases, some degree of inflammation and calcifications and ependymal cystic degeneration can also be seen occasionally. Immunohistochemistry has an important role in the analysis of tumors. The glial and neuronal nature of cells is demonstrated by the presence of the S100 protein, GFAP, NSE (neuron specific enolase) and vimetida.[3] [4] [5] [6] [7] [10] [15] [16] [17] Neuronal cells, when present, are sparse and not prominent. The Ki67 and p53 markers are negative among gliomas.[15]
Conclusion
Nasal gliomas are rare congenital anomalies that must be considered among the differential diagnoses of nasal masses in newborns, as well as dermoid cysts and encephaloceles. Diagnostic suspicion can be made in the prenatal period, first through Doppler ultrasonography and, later, by MRI. Imaging exams are mandatory to exclude the intracranial extension of the mass. In the case of intranasal glioma, the treatment of choice is endoscopic resection. The approach to extranasal gliomas may vary according to their location. In the presence of intracranial communication, craniotomy is indicated. Early intervention favors the prevention of facial deformities and secondary infections. Diagnostic difficulty can be found in children older than 1 year, in view of the atypical presentation of the condition.
No conflict of interest has been declared by the author(s).
Ethics statement
Este estudo está em conformidade com todas as diretrizes institucionais relativas a seres humanos. O consentimento informado foi obtido do responsável pelo paciente.
Disclosure statement
Os autores declaram não haver conflitos de interesse.
* Institution in which the study was carried out: Erasto Gaertner Hospital, Curitiba, PR, Brazil.
-
References
- 1 Verney Y, Zanolla G, Teixeira R, Oliveira LC. Midline nasal mass in infancy: a nasal glioma case report. Eur J Pediatr Surg 2001; 11 (05) 324-327
- 2 Rouev P, Dimov P, Shomov G. A case of nasal glioma in a new-born infant. Int J Pediatr Otorhinolaryngol 2001; 58 (01) 91-94
- 3 Dasgupta NR, Bentz ML. Nasal gliomas: identification and differentiation from hemangiomas. J Craniofac Surg 2003; 14 (05) 736-738
- 4 Penner CR, Thompson L. Nasal glial heterotopia: a clinicopathologic and immunophenotypic analysis of 10 cases with a review of the literature. Ann Diagn Pathol 2003; 7 (06) 354-359
- 5 Sharma JK, Pippal SK, Sethi Y, Arora S, Raghuwanshi SK. Nasal glioma : A case report. Indian J Otolaryngol Head Neck Surg 2006; 58 (04) 413-415
- 6 Irkoren S, Selman Ozkan H, Karaca H. Nasal glioma presenting with strabismus. Ophthal Plast Reconstr Surg 2015; 31 (03) e57-e59
- 7 Medel BS, Fernández AF, Sáez EE, Bachelet RC. Glioma nasal gigante: reporte de un caso. Rev Otorrinolaringol Cir Cabeza Cuello 2015; 75 (03) 257-260
- 8 Rahbar R, Resto VA, Robson CD. et al. Nasal glioma and encephalocele: diagnosis and management. Laryngoscope 2003; 113 (12) 2069-2077
- 9 Petersson RS, Carlson ML, Wetjen NM, Orvidas LJ, Thompson DM. Nasal dermoid cyst and nasal glioma with intracranial extension. Laryngoscope 2010; 120 (Suppl. 04) S225-S225
- 10 Jiang L, Lai Y. Nasal Glioma: A Case Report and Review of Literature. J Case Rep Clin Med. 2017; 1 (01) 112
- 11 Tonni G, Lituania M, Bonasoni MP, De Felice C. Prenatal ultrasound and histological diagnosis of fetal nasal glioma (heterotopic central nervous system tissue): report of a new case and review of the literature. Arch Gynecol Obstet 2011; 283 (Suppl. 01) 55-59
- 12 Charles NC, Lisman RD, Patel P, Callahan AB. Nasal Glioma: A Rare Cause of Congenital Inner Canthal Swelling. Ophthal Plast Reconstr Surg 2018; 34 (03) e93-e95
- 13 Jartti PH, Jartti AE, Karttunen AI, Pääkkö EL, Herva RL, Pirilä TO. MR of a nasal glioma in a young infant. Acta Radiol 2002; 43 (02) 141-143
- 14 Oddone M, Granata C, Dalmonte P, Biscaldi E, Rossi U, Toma P. Nasal glioma in an infant. Pediatr Radiol 2002; 32 (02) 104-105
- 15 Frizzarini R, Lessa M, Goto E, Voegels R, Sennes L, Butugan O. Glioma nasal: relato de três casos e revisão de literatura. Rev Bras Otorrinolaringol 2003; 69 (04) 561-564
- 16 Salati SA, Rather AA. Congenital intranasal glioma. Case Rep Surg 2011; 2011: 175209
- 17 Horn D, Klein N, McSoley T. External rhinoplasty excision of a nasal tip glioma in a 6-month-old infant: Case report and review of the literature. Int J Pediatr Otorhinolaryngol Extra 2010; 5 (02) 79-84
- 18 Pereyra-Rodríguez JJ, Bernabeu-Wittel J, Fajardo M, Torre C, Sánchez-Gallego F. Nasal glial heterotopia (nasal glioma). J Pediatr 2010; 156 (04) 688-688.e1
Address for correspondence
Publication History
Received: 25 January 2021
Accepted: 16 June 2021
Article published online:
26 April 2024
© 2024. Sociedade Brasileira de Neurocirurgia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
References
- 1 Verney Y, Zanolla G, Teixeira R, Oliveira LC. Midline nasal mass in infancy: a nasal glioma case report. Eur J Pediatr Surg 2001; 11 (05) 324-327
- 2 Rouev P, Dimov P, Shomov G. A case of nasal glioma in a new-born infant. Int J Pediatr Otorhinolaryngol 2001; 58 (01) 91-94
- 3 Dasgupta NR, Bentz ML. Nasal gliomas: identification and differentiation from hemangiomas. J Craniofac Surg 2003; 14 (05) 736-738
- 4 Penner CR, Thompson L. Nasal glial heterotopia: a clinicopathologic and immunophenotypic analysis of 10 cases with a review of the literature. Ann Diagn Pathol 2003; 7 (06) 354-359
- 5 Sharma JK, Pippal SK, Sethi Y, Arora S, Raghuwanshi SK. Nasal glioma : A case report. Indian J Otolaryngol Head Neck Surg 2006; 58 (04) 413-415
- 6 Irkoren S, Selman Ozkan H, Karaca H. Nasal glioma presenting with strabismus. Ophthal Plast Reconstr Surg 2015; 31 (03) e57-e59
- 7 Medel BS, Fernández AF, Sáez EE, Bachelet RC. Glioma nasal gigante: reporte de un caso. Rev Otorrinolaringol Cir Cabeza Cuello 2015; 75 (03) 257-260
- 8 Rahbar R, Resto VA, Robson CD. et al. Nasal glioma and encephalocele: diagnosis and management. Laryngoscope 2003; 113 (12) 2069-2077
- 9 Petersson RS, Carlson ML, Wetjen NM, Orvidas LJ, Thompson DM. Nasal dermoid cyst and nasal glioma with intracranial extension. Laryngoscope 2010; 120 (Suppl. 04) S225-S225
- 10 Jiang L, Lai Y. Nasal Glioma: A Case Report and Review of Literature. J Case Rep Clin Med. 2017; 1 (01) 112
- 11 Tonni G, Lituania M, Bonasoni MP, De Felice C. Prenatal ultrasound and histological diagnosis of fetal nasal glioma (heterotopic central nervous system tissue): report of a new case and review of the literature. Arch Gynecol Obstet 2011; 283 (Suppl. 01) 55-59
- 12 Charles NC, Lisman RD, Patel P, Callahan AB. Nasal Glioma: A Rare Cause of Congenital Inner Canthal Swelling. Ophthal Plast Reconstr Surg 2018; 34 (03) e93-e95
- 13 Jartti PH, Jartti AE, Karttunen AI, Pääkkö EL, Herva RL, Pirilä TO. MR of a nasal glioma in a young infant. Acta Radiol 2002; 43 (02) 141-143
- 14 Oddone M, Granata C, Dalmonte P, Biscaldi E, Rossi U, Toma P. Nasal glioma in an infant. Pediatr Radiol 2002; 32 (02) 104-105
- 15 Frizzarini R, Lessa M, Goto E, Voegels R, Sennes L, Butugan O. Glioma nasal: relato de três casos e revisão de literatura. Rev Bras Otorrinolaringol 2003; 69 (04) 561-564
- 16 Salati SA, Rather AA. Congenital intranasal glioma. Case Rep Surg 2011; 2011: 175209
- 17 Horn D, Klein N, McSoley T. External rhinoplasty excision of a nasal tip glioma in a 6-month-old infant: Case report and review of the literature. Int J Pediatr Otorhinolaryngol Extra 2010; 5 (02) 79-84
- 18 Pereyra-Rodríguez JJ, Bernabeu-Wittel J, Fajardo M, Torre C, Sánchez-Gallego F. Nasal glial heterotopia (nasal glioma). J Pediatr 2010; 156 (04) 688-688.e1