
Subscribe to RSS
DOI: 10.1055/s-0043-1775871
Application of Lasers in Vascular Anomalies

Abstract
Laser technology has significantly improved giving better results, which in turn has led to an increase in the indications for laser therapy. Vascular anomalies comprise vascular tumors and malformations. They are classified according to the type of vessels involved including arteries, capillaries, postcapillary venules, veins, lymphatic vessels, and a combination of two or more of these. Laser needs a chromophore to get absorbed and act. Hemoglobin, both oxy and deoxy, is one of the naturally occurring chromophore that is abundant in vascular lesions. Therefore, in most of the vascular lesions, lasers can bring improvement of a varying degree, while for superficial hemangiomas and port wine stain (PWS) laser treatment is now the standard of care. However, even though there is increase in the use of lasers in clinical practice, many surgeons are still unaware of its versatility and they are unsure about its safety. This article provides a brief overview of laser and intense pulsed light (IPL) technology, and describes the key principles in using these energy sources in vascular malformations. Readers are also familiarized with possible adverse effects and measures to prevent and treat them.
#
Keywords
laser treatment - vascular malformations - vascular anomalies - vascular lasers - hemangiomaIntroduction
The first laser produced was a ruby laser and Theodore H. Maiman demonstrated it in a press conference on July 7, 1960.[1] In 1968, Goldman and Eckhouse reported the first successful clinical treatment of vascular lesions with laser.[2] Vascular malformations (VMs) result from alterations in blood vessels and lymphatic channels and can involve multiple systems and organs.[3] To carry out laser treatment efficiently, basic knowledge of laser physics, laser tissue interaction, and overall understanding of laser systems and intense pulsed light (IPL) sources are required
#
Terminology
-
LASER: Laser is an acronym for “light amplification by stimulated emission of radiation.” Stimulated emission was based on Einstein's quantum theory of radiation.[4] Laser light is monochromatic, coherent, unidirectional, and bright.
-
Intense pulsed light (IPL): Flash lamp usually emits wavelengths in the range from 380 to 1,200 nm and the shorter and longer wavelengths can be eliminated by various cutoff filters (515–755 nm) and water jacket, respectively.
-
Chromophore: Chromophores can be either endogenous or exogenous, meaning they can be either present in the tissues or brought from outside, which absorbs particular wavelengths depending on their absorption coefficient[5] ([Fig. 1]).
-
Selective photothermolysis (SPTL): In 1983, Anderson and Parrish[7] described the theory of SPTL, explaining a method of producing selective and localized tissue damage while sparing the surrounding tissue. This revolutionized laser therapy.
-
Pulse duration: Thermal relaxation time (TRT) depends on the size of the target vessel and selection of pulse duration is mainly guided by the TRT. As large objects take a long time to get heated and to cool down, the larger the vessel, the longer the TRT. More difficulty is encountered while lasing the smaller-diameter vessels. Small vessels need very short pulse width, which makes the epidermis having a TRT of approximately 4 to 10 milliseconds more vulnerable. To overcome this, the short pulse is subdivided into still shorter rations of subpulses that are delivered in rapid succession with a gap of 10 to 40 milliseconds between them. This form of energy delivery is called multiple synchronized pulsing.
-
Multiple Synchronized Sequential Pulsing: Even though the epidermis is a strong competing chromophore, it can be spared as long as the TRT of the target vessels is equal to or longer than that of the epidermis ([Fig. 2]; [Table 1]) Longer TRT means the target takes longer time to cool to 50% of the temperature achieved. Multiple synchronized pulsing usually has two or three subpulses, with periods of delay in between. By the first pulse, both the vessels and epidermis are heated just within the threshold limit of the epidermis; therefore, the epidermis is not damaged. After the first pulse, there is a delay, during which both epidermis and target start cooling; However, as the target cools slowly at the end of the delay, it still retains some heat, while the epidermis gets cooled down completely, aided by the external cooling applied. During the second pulse and the delay thereafter, the same sequence repeats, but now the target gets heated to a higher level as it is starting from an elevated baseline. This pulsing is repeated till such time as the temperature in the target at the end of the last pulse exceeds its threshold limit.[8]


Abbreviations: IPL, intense pulsed light; PDL, pulsed dye laser; PWS, port wine stain.
Source: Adapted from Anderson and Parrish.[9]
Classification of Vascular Anomalies
In 1982, Mulliken and Glowacki[10] proposed a biologic classification system to describe two types of vascular anomalies: hemangiomas and VMs. The most recent classification system adopted by the International Society for the Study of Vascular Anomalies in 2014, and revised in 2018, defines VMs in more detail, proposes more causal genes of vascular anomalies, and includes more complex syndromes with other abnormalities.[11] [12]
#
Role of Lasers in Vascular Lesions
Vascular lesions require proper diagnosis and a clear understanding of their biologic behavior.[13] Cutaneous vascular lesions are one of the most common indications for laser treatment. They are either persistent or growing because of intact vessel wall. Although their chromophore is hemoglobin in its various forms, the ultimate target is the vessel wall. Water content of blood and vessel wall also acts as an additional chromophore. Cure in vascular lesions essentially lies in destroying the vessel wall permanently.[14]
Hemoglobin has an absorption coefficient curve with peaks at 418, 524, 577, and at 1,064 nm ([Fig. 1]). Even though the absorption coefficient is very high, wavelengths at 418 and 524 nm are too short to penetrate to any useful depth in the dermis and their absorption in the competing epidermal melanin is also very high; therefore, these wavelengths cannot be used in vascular lesions. However, the spectrum between 580 and 595 nm is useful clinically.[15] Histologic studies have shown findings that correspond to the clinically obvious purpura seen after treatment with the pulsed dye laser (PDL). There are histologic findings of agglutinated red blood cells, fibrin, and platelet thrombi within the vessels of the papillary and superficial reticular dermis.[9] As would be expected, there is little or no damage to the surrounding tissue.[13] At fourth peak, which is the last peak of absorption coefficient of hemoglobin, the 1,064-nm wavelength, being a longer wavelength, has the advantage of deeper penetration and therefore is the wavelength of choice for deeper vascular lesions like thick or nodular hemangiomas and venous malformations (VMs). Vascular lesions are unique in the sense that their chromophore is moving, albeit slow in many of them, which raises the issue of retention and effective application of heat to the vessel wall. Therefore, only slow-flow lesions can retain the generated heat sufficiently long enough for the vessel wall to get destroyed.
Vascular lesions are dynamic and changes are often visible during and immediately after treatment. During treatment, the desired clinical effects are monitored, and the treatment parameters are adjusted to achieve effective end point. This includes observing for changes in the targeted vessel, such as blanching, graying, and simultaneously observing the integrity and color of the epidermis. Clinically observed factors such as blanching, whitening, purpura, erythema, edema, or severe pain should be closely observed and continuously evaluated to guide optimal and safe treatment.
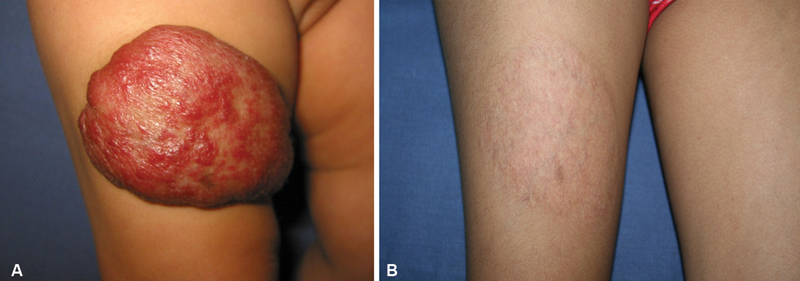
Hemangioma
The only limiting factor in laser treatment of deeper vascular lesions at present is reaching the target and retaining the generated heat. Currently with the wavelength of 1,064 nm, we can reach a maximum of 5 to 6 mm under the skin surface[16] ([Figs. 3] [4] [5] [6]).



#
“Halo” of growth
When laser treatment of congenital or infantile hemangioma is started very early during the neonatal period or during infancy in its proliferative phase, a peculiar phenomenon is observed, which the author has named the “halo of growth.” With initial few laser treatments, the already manifested hemangioma gets cleared, but a ring of capillaries appears around it as this area was destined to be a hemangioma. This happens because laser cannot act unless there is a chromophore. Prior intimation to the parents about the possibility of this occurrence mitigates any misunderstanding ([Fig. 7]).

#
Things to Remember
-
“Wait and watch” and “masterly inactivity” policies were advocated for hemangioma when no definitive curative treatment existed.
-
Unpredictability of spontaneous involution of hemangiomas seems to favor earliest intervention with a vascular-specific laser.
#
#
Capillary Malformations
Capillary malformations (CMs) are present at birth and persist throughout life. A port wine stain (PWS) is one of the most common types of CM. Most CMs have a cosmetic problem, but unlike the nevus simplex, a PWS does not fade in the early ages of childhood. On the contrary, during puberty, the skin thickens and gradually becomes raised with multiple nodular fibrovascular lesions due to underlying soft-tissue hypertrophy. Because the dermal thickness increases with age allowing for less optimal targeting of vessels, better response is achieved if the treatment is begun earlier during childhood.[17]
Port Wine Stain or Nevus Flammeus
Flash lamp PDL was the first example of a laser that was specifically constructed to treat PWS.[18] Initially, this laser had a 577-nm wavelength to match the third peak of the absorption curve of hemoglobin and 0.45-millisecond pulse duration, which was less than the TRT of the smaller vessels (postcapillary venules) of PWS[7] ([Table 1]). Later on, it was replaced by yellow light at 585 and finally at 595 nm, having still deeper penetration and giving better results ([Fig. 8]). TRT of the epidermis varies from 3 to 10 milliseconds. Capillaries of PWS are very fine and range from 50 to 100 µm having a TRT of 1 to 5 milliseconds. Unless the pulse is ultrashort, they cannot be heated till destruction. PDL has a 0.45-millisecond pulse width, which is less than the TRT of the smaller vessels of PWS. Additionally, the epidermis is protected with Dynamic Cooling Device (DCD).[19] Although PDL is considered the treatment of choice for most of the PWS, IPL sources with a cutoff filter of 590 nm are also quite effective and are being routinely used for a variety of superficial vascular lesions including PWS.

By extending the principle of SPTL and by making use of multiple synchronized sequential pulsing, the laser surgeon is now able to selectively target a larger or a smaller vessel in the same lesion having the same common chromophore, hemoglobin ([Fig. 9]).

#
#
Venous Malformations
VMs are developmental abnormalities of veins, present at birth and which do not subside on their own like some hemangiomas. They are made up of thin-walled dilated channels of variable size, which show progressive dilatation with age and persist till adulthood ([Fig. 10]). They are more frequent on the head and neck but may occur at any site and may infiltrate any structure of the body including the skin, mucous membrane, bones, joints, and even viscera.[20] For cutaneous and mucosal VMs, a 1,064-nm Nd:YAG (neodymium:yttrium aluminum garnet) laser represents the most effective option as they are thick lesions. Since the absorption coefficient of hemoglobin is low at 1,064 nm, use of high fluence is required. Contact cooling and a large spot size is helpful in reducing scarring ([Figs. 11] and [12]). Their vessels are larger, very thin walled, and contain abundant deoxy hemoglobin; therefore, even though they respond very well to Nd:YAG 1,064-nm laser, a rather low energy has to be delivered to them as at times it can lead to scarring ([Fig. 13]).




#
Arteriovenous Malformations
Arteriovenous malformations (AVMs) form when veins are connected to arteries without an intervening capillary bed and are often mistaken for a hemangioma in children. These are fast-flow VMs, in which the blood flows directly from a high-pressure system to a low-pressure system.[21] The clinical management of pediatric AVMs requires a detailed examination and long-term clinical observation. The most common treatments are surgical interventions and intravascular embolotherapy/sclerotherapy, and a combination of both may sometimes be effective, especially in children.[22] As compared with all other VMs, AVMs, being high-flow lesions, are unable to retain the heat generated by laser. However, if an AVM can be converted into a low-flow lesion by feeder ligation, then it can be treated with 1,064-nm Nd:YAG laser sessions. However, feeder ligation may have to be repeated more than once as new feeders open up subsequently ([Figs. 14] and [15]).


#
Combined and Complex Combined Vascular Malformations
Due to hyperplasia of the lymphatic network, lymphatic malformations are slow-flow vascular anomalies characterized by dilated lymphatic channels and cysts. Combined malformations such as capillary-venous malformation (CVM), capillary-lymphatic malformation (CLM), lymphaticovenous malformation (LVM), and complex combined malformation. Capillary-lymphaticovenous malformations (CLVMs) have some vascular element that acts as a chromophore in addition to water and absorbs laser. Because these are slow-flow lesions, the generated heat gets time to be conducted to the vessel wall, leading to its destruction ([Fig. 16]).

Role of Endovascular Lasers
The role of endovascular lasers in VMs is limited, wherein laser energy is directly delivered to the vessel wall intraluminally carried through an optical fiber. Diodes 808, 1,470, 1,940, and Nd:YAG 1,320 nm are most suited as they can be carried through the fine optical fiber. Deeply situated, large or extensive malformations, including low-flow venous, lymphaticovenous, and AVMs can be partially controlled with this modality performed under anesthesia under color Doppler guidance. After locating a relatively straight segment of vessel, luminal access is gained with a 10-cm-long 18-gauge spinal needle, and a 600-µm or smaller, 400- or 200-µm, fiber is passed through it and energy is delivered till its closure.
#
#
Adverse Effects and Complications
Excess fluence leads to epidermal erythema, superficial burn, or deep dermal burn with incident scarring depending on the extent of injury. Edema is very common and appears within a few minutes after laser treatment of vascular lesions. Application of ice pack immediately after treatment and continuation till the burning sensation subsides will help reduce it. It resolves within a few hours but one has to refrain from prescribing nonsteroidal anti-inflammatory drugs (NSAIDs) to overcome it as the aseptic inflammation is useful for closing the vessels. A word of caution is in order here while treating vascular lesions in oral cavity and particularly on posterior tongue or cheek, where severe edema can obstruct air passage in post treatment period. One may administer only a few laser pulses during the first session to judge the edema response and during subsequent sessions increase the number of pulses.
In case of lesions like PWS, ecchymosis and purpura followed by dry crusting are unavoidable. Antiseptic creams should be used in the postlaser period. It usually peels off within 4 to 8 days. Moisturizer and sunscreen lotion or gel is to be continued throughout the course of treatment.
In late complications, pigmentary changes either hypo- or, more frequently, hyperpigmentation are due to repeated treatments on the same area and it may be visible after a few sessions. Hyperpigmentation is undesirable as it competes during subsequent treatments. Depigmenting creams and laser can be used to treat it.
In sequelae, scarring due to overtreatment is a hidden risk. In case of VMs, this is attributable to thin-walled larger vessels filled with abundant chromophore, which absorbs a lot of energy. Low fluence and minimum number of shots can mitigate this complication.
#
#
Conclusion
The goal of management and treatment of VMs is to maintain functionality, control associated symptoms, and preserve aesthetic integrity. Laser treatment plays a role in achieving these goals in varying degrees. Complex VMs, although benign, cause deformation, can impair function of vital structures, or even threaten the child's life. Such severe life-threatening functional impairment mandates early intervention with nonlaser modalities. Therefore, to ensure optimal treatment, a multifocal and a multidisciplinary team approach is advocated with the patient's quality of life as the priority.[23] This includes observation, laser or radiofrequency ablation, sclerotherapy, embolotherapy, surgical resection, and medical therapy.
#
#
Conflict of Interest
None declared.
Declaration of Consent
The author has obtained consent of all patients to publish their photographs in this article.
-
References
- 1 Alster TS. Preface. In: Manual of Cutaneous Laser Techniques. Philadelphia, PA: Lippincott Williams and Wilkins; 2000: 11
- 2 Geronemus RG. Pulsed dye laser treatment of vascular lesions in children. J Dermatol Surg Oncol 1993; 19 (04) 303-310
- 3 Azizkhan RG. Complex vascular anomalies. Pediatr Surg Int 2013; 29 (10) 1023-1038
- 4 Einstein A. Zur Quantentheorie der Strahlung. Physikalische Gesellschaft Zϋrich Miteilungen 1916; 18: 47-62 . Subsequently published in Physikalische Zeitschrift 1917;18:121–128. Reprinted in Kox AJ et al., eds. The collected papers of Albert Einstein: The Berlin Years, Writings, 1914–1917, Princeton: Princeton University Press, 1966:381–397. See also: Einstein A. Uber Einen die Erzeugung und Umwandlung des Lichts Betreffenden Heuristischen Standpunkt. Annalen der Physik 1905;17:132–184
- 5 Dover JS, Arndt KA, Geronemus RG. et al. Illustrated Cutaneous Laser Surgery: A Practitioner's Guide. Norwalk, CT: Appleton & Lange; 1990
- 6 Boulnois JL. Photophysical processes in recent medical laser developments: a review. Med Sci 1986; 1: 47-66
- 7 Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983; 220 (4596) 524-527
- 8 Patil UA, Dhami LD. Overview of lasers. Indian J Plast Surg 2008; 41 (Suppl): S101-S113
- 9 Anderson RR, Parrish JA. Microvasculature can be selectively damaged using dye lasers: a basic theory and experimental evidence in human skin. Lasers Surg Med 1981; 1 (03) 263-276
- 10 Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg 1982; 69 (03) 412-422
- 11 ISSVA. Classification of Vascular Anomalies 2014 International Society for the Study of Vascular Anomalies. Accessed March 20, 2017 at: http://issva.org/classification
- 12 Zhang B, Ma L. Updated classification and therapy of vascular malformations in pediatric patients. Pediatr Investig 2018; 2 (02) 119-123
- 13 Goldberg DJ. Laser treatment of vascular lesions. Clin Plast Surg 2000; 27 (02) 173-180 , ix
- 14 Dhami LD, Patil UA. Lasers and energy devices in plastic surgery. In: Agrawal K, Bhattacharya S. eds. Textbook of Plastic, Reconstructive, and Aesthetic Surgery. Vol. 1. Thieme; 2017: 401-428
- 15 Goldberg DJ. ed. Laser Dermatology. Berlin: Springer-Verlag; 2013
- 16 Scherer K, Waner M. Nd:YAG lasers (1,064 nm) in the treatment of venous malformations of the face and neck: challenges and benefits. Lasers Med Sci 2007; 22 (02) 119-126
- 17 Astner S, Anderson RR. Treating vascular lesions. Dermatol Ther 2005; 18 (03) 267-281
- 18 Goldman MP, Eckhouse S. Photothermal sclerosis of leg veins. ESC Medical Systems, LTD Photoderm VL Cooperative Study Group. Dermatol Surg 1996; 22 (04) 323-330
- 19 DCD: Dynamic Cooling Devices is a trademark of Candela, which sprays the treatment area before each laser pulse with a liquid cryogen coolant. This system provides a cooling protection factor over 50% greater than contact or air cooling and can be adjusted to individual needs to make the procedure as comfortable as possible.
- 20 McRae MY, Adams S, Pereira J, Parsi K, Wargon O. Venous malformations: Clinical course and management of vascular birthmark clinic cases. Australas J Dermatol 2013; 54 (01) 22-30
- 21 Galich SP, Dabizha AIu, Gindich OA. et al. Combined treatment of arteriovenous malformations of the head and neck. Angiol Sosud Khir 2015; 21 (01) 170-177
- 22 Johnson CM, Navarro OM. Clinical and sonographic features of pediatric soft-tissue vascular anomalies part 2: vascular malformations. Pediatr Radiol 2017; 47 (09) 1196-1208
- 23 Balakrishnan K, Edwards TC, Perkins JA. Functional and symptom impacts of pediatric head and neck lymphatic malformations: developing a patient-derived instrument. Otolaryngol Head Neck Surg 2012; 147 (05) 925-931
Address for correspondence
Publication History
Article published online:
03 November 2023
© 2023. Association of Plastic Surgeons of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Alster TS. Preface. In: Manual of Cutaneous Laser Techniques. Philadelphia, PA: Lippincott Williams and Wilkins; 2000: 11
- 2 Geronemus RG. Pulsed dye laser treatment of vascular lesions in children. J Dermatol Surg Oncol 1993; 19 (04) 303-310
- 3 Azizkhan RG. Complex vascular anomalies. Pediatr Surg Int 2013; 29 (10) 1023-1038
- 4 Einstein A. Zur Quantentheorie der Strahlung. Physikalische Gesellschaft Zϋrich Miteilungen 1916; 18: 47-62 . Subsequently published in Physikalische Zeitschrift 1917;18:121–128. Reprinted in Kox AJ et al., eds. The collected papers of Albert Einstein: The Berlin Years, Writings, 1914–1917, Princeton: Princeton University Press, 1966:381–397. See also: Einstein A. Uber Einen die Erzeugung und Umwandlung des Lichts Betreffenden Heuristischen Standpunkt. Annalen der Physik 1905;17:132–184
- 5 Dover JS, Arndt KA, Geronemus RG. et al. Illustrated Cutaneous Laser Surgery: A Practitioner's Guide. Norwalk, CT: Appleton & Lange; 1990
- 6 Boulnois JL. Photophysical processes in recent medical laser developments: a review. Med Sci 1986; 1: 47-66
- 7 Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983; 220 (4596) 524-527
- 8 Patil UA, Dhami LD. Overview of lasers. Indian J Plast Surg 2008; 41 (Suppl): S101-S113
- 9 Anderson RR, Parrish JA. Microvasculature can be selectively damaged using dye lasers: a basic theory and experimental evidence in human skin. Lasers Surg Med 1981; 1 (03) 263-276
- 10 Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg 1982; 69 (03) 412-422
- 11 ISSVA. Classification of Vascular Anomalies 2014 International Society for the Study of Vascular Anomalies. Accessed March 20, 2017 at: http://issva.org/classification
- 12 Zhang B, Ma L. Updated classification and therapy of vascular malformations in pediatric patients. Pediatr Investig 2018; 2 (02) 119-123
- 13 Goldberg DJ. Laser treatment of vascular lesions. Clin Plast Surg 2000; 27 (02) 173-180 , ix
- 14 Dhami LD, Patil UA. Lasers and energy devices in plastic surgery. In: Agrawal K, Bhattacharya S. eds. Textbook of Plastic, Reconstructive, and Aesthetic Surgery. Vol. 1. Thieme; 2017: 401-428
- 15 Goldberg DJ. ed. Laser Dermatology. Berlin: Springer-Verlag; 2013
- 16 Scherer K, Waner M. Nd:YAG lasers (1,064 nm) in the treatment of venous malformations of the face and neck: challenges and benefits. Lasers Med Sci 2007; 22 (02) 119-126
- 17 Astner S, Anderson RR. Treating vascular lesions. Dermatol Ther 2005; 18 (03) 267-281
- 18 Goldman MP, Eckhouse S. Photothermal sclerosis of leg veins. ESC Medical Systems, LTD Photoderm VL Cooperative Study Group. Dermatol Surg 1996; 22 (04) 323-330
- 19 DCD: Dynamic Cooling Devices is a trademark of Candela, which sprays the treatment area before each laser pulse with a liquid cryogen coolant. This system provides a cooling protection factor over 50% greater than contact or air cooling and can be adjusted to individual needs to make the procedure as comfortable as possible.
- 20 McRae MY, Adams S, Pereira J, Parsi K, Wargon O. Venous malformations: Clinical course and management of vascular birthmark clinic cases. Australas J Dermatol 2013; 54 (01) 22-30
- 21 Galich SP, Dabizha AIu, Gindich OA. et al. Combined treatment of arteriovenous malformations of the head and neck. Angiol Sosud Khir 2015; 21 (01) 170-177
- 22 Johnson CM, Navarro OM. Clinical and sonographic features of pediatric soft-tissue vascular anomalies part 2: vascular malformations. Pediatr Radiol 2017; 47 (09) 1196-1208
- 23 Balakrishnan K, Edwards TC, Perkins JA. Functional and symptom impacts of pediatric head and neck lymphatic malformations: developing a patient-derived instrument. Otolaryngol Head Neck Surg 2012; 147 (05) 925-931