
RSS-Feed abonnieren
DOI: 10.1055/s-0043-1764310
Pathological Basis of Imaging in Hepatocellular Carcinoma


- Abstract
- Introduction
- Hepatocarcinogenesis
- Pathogenesis and Pathology of Precursor Nodules
- Iron, Chronic Liver Disease, and HCC
- Fat, Chronic Liver Disease, and HCC
- HCC Appearance and Morphology on Contrast-Enhanced MRI
- HCC Appearance and Morphology on Noncontrast MRI
- Newer Variants of HCC
- Proliferative and Nonproliferative HCC
- Conclusion
- References
Abstract
Hepatocellular carcinoma (HCC) is the most prevalent form of liver cancer with major risk factors being chronic liver disease (CLD) including chronic liver inflammation, steatohepatitis and certain viral infections (Hepatitis B and C). Due to the poor prognosis, early detection is key for effective management. Imaging of HCC has developed over the years with specificity as high as 95%. The Liver Imaging Reporting and Data System (LI-RADS) provides a standardized reporting format that can be followed by radiologists and clinicians alike. This article focuses on the pathological basis of imaging observations described in the LI-RADS lexicon. A clear understanding of the pathological basis of imaging will help the radiologist to be more confident to resolve unequivocal observations apart from achieving a high degree of specificity in the diagnosis of HCC.
#
Keywords
computed tomography - hepatocellular carcinoma - Liver Imaging Reporting and Data System - magnetic resonance imagingIntroduction
Hepatocellular carcinoma (HCC) is the most prevalent form of liver cancer and the fifth most common cancer worldwide. It is a leading cause of cancer mortality with a dismal 5-year survival rate of less than 10%.[1] [2]
To date, hepatitis B and C related chronic liver disease (CLD) remains the major risk factors for the development of HCC. With hepatitis B vaccination and better pharmacologic management of both hepatitis B and C, the incidence of viral infection–related CLD and HCC is likely to fall in the coming years. However, due to their rising incidence, obesity, metabolic syndrome, and nonalcoholic fatty liver disease (NAFLD) are set to become major risk factors for the development of CLD and HCC in the foreseeable future.[3] [4] In the majority of cases (80%), HCC develops in a cirrhotic liver. Chronic liver inflammation due to hepatitis B or C and steatohepatitis are also risk factors for the development of HCC in a morphologically normal liver in a minority of cases.[5] [6]
As discussed, the 5-year survival of HCC is low at approximately 10% with a median survival of 1 year.[2] [5] Due to the poor prognosis, early detection is key for effective management. Curative options for HCC include liver transplant and liver resections, apart from various noninvasive interventions.
Imaging of HCC has developed over the years and can now offer specificity of over 95%.[7] The Liver Imaging Reporting and Data System (LI-RADS) group has created an easily replicable standardized reporting format that can be followed by radiologists and clinicians alike. LI-RADS is now accepted by the American Association for the Study of Liver Diseases (AASLD) as well as the Organ Procurement and Transplantation Network (OPTN) as an optimum and standard reporting system. Patients can undergo medical, nonsurgical therapeutic procedures as well as surgery and transplant based on an LR-5 imaging category without a pathological diagnosis.
With the use of LI-RADS, liver biopsy for HCC can be obviated in the LR-5 category. Other categories may need a biopsy. Biopsy may also be needed in any LI-RADS category for clinical trials, prior to the use of novel immunotherapy and targeted drugs that continue to be developed. Biopsy may also be required to determine grade and molecular characterization of any liver malignancy including HCC.
This article focuses on the pathological basis of imaging observations, which form the basis of the LI-RADS lexicon. A clear understanding of the pathological basis of imaging will help the radiologist to be more confident to resolve unequivocal observations apart from achieving a high degree of specificity in the diagnosis of HCC.
#
Hepatocarcinogenesis
HCC is an epithelial tumor, the cells of which are very similar to a normal hepatocyte. The process of transition of a normal hepatocyte to HCC happens over several complex steps that are influenced by genetic and environmental processes.[5] It is said that “genetics loads the gun and the environment pulls the trigger.” The development of HCC epitomizes this concept.
Hepatocarcinogenesis is described here under the following subheadings:
-
Genetic and molecular changes.
-
Cellular changes.
Genetic and Molecular Changes
The changes at the genetic level determine the metabolic pathway alterations that can lead to the development of HCC ([Fig. 1]). Risk factors contribute to the epigenetic mechanisms that are responsible for the formation of a neoplastic cell from a normal hepatocyte. The genetic mutations involved in hepatocarcinogenesis are tabulated in [Table 1].[8] The above genetic mutations alter several metabolic pathways as mentioned in [Table 2].[8]
|
Key genetic mutations in HCC[8] |
|---|
|
TERT |
|
β-catenin |
|
TP-53 |
Abbreviations: TERT, telomerase reverse transcriptase; TP53, tumor protein p53.

Varied permutations and combinations of mutations and signaling pathways lead to the development of different genotypic variants of HCC. The resulting phenotypes exhibit different biologic and clinical behavior that influences prognosis and survival. The genetic and molecular susceptibility is aided by several epigenetic risk factors in hepatocarcinogenesis. Most HCC develop in a cirrhotic liver, which in turn results from hepatitis B and C infection. Many other risk factors are responsible for the development of CLD.[4] [9] [10] [11] Lists of risk factors are enumerated in [Table 3].
#
Cellular Changes
Cellular development of HCC is from two types of cells[2] [12]:
-
Hepatocytes undergo dedifferentiation to form HCC.
-
Intrahepatic stem cells located in the canals of herring can undergo oncogenic stimulation due to chronic liver injury. HCC can develop as a result of oncogenic stimulation. It is of note that intrahepatic cholangiocarcinoma (IHCC) is also a result of such oncogenic stimulation.
Chronic inflammation due to infections (hepatitis B and C) or other insults (heavy alcoholism, etc.) lead to cellular changes of fibrosis and cirrhosis. The chronically inflamed liver develops regenerative and cirrhotic nodules.
With repeated injury, the cirrhotic nodule develops small clones of dysplastic changes within the primary cirrhotic nodule. These subsets of clones progress through early and late dysplastic changes to form early and progressed HCC. The clonal subset replaces the cells of the cirrhotic nodule through progress from benignity to malignancy ([Fig. 2]). Imaging may or may not be reliable in differentiating these precursor stages.

HCC may develop de novo without transitioning through the precursor stages as well.[13] Patients with sustained virologic response after curative medication may develop de novo HCC as well, although they carry a better prognosis and survival.[14]
HCC may be multicentric in the liver with the process of carcinogenesis progressing at different rates in each different site at a given time point.
Although chronic inflammation is a trigger for cirrhosis and the development of HCC, the two processes are mutually exclusive and run in parallel to each other. Since the neoplastic process is much slower than the changes of fibrosis, HCC is nearly always found in cirrhotic livers. Hence, cirrhosis should not be considered a premalignant condition.
#
#
Pathogenesis and Pathology of Precursor Nodules
The spectrum of precursor nodules that precede the development of a full-fledged malignant lesion (HCC) and their pathological characteristics are tabulated in [Table 4]. The precursor nodules give rise to early and progressed HCC. Progressed HCC may occur in a late dysplastic nodule as well. A comparative of the pathological features of early and progressed HCC are enumerated in [Table 5].
Multiple HCC may develop in the liver separated by normal noncancerous liver parenchyma. There are two causes for the same ([Fig. 3]).

-
Development of multiple foci of carcinogenesis. The different foci then show different grades and differentiation.
-
Development of metastatic foci from a primary lesion. The lesions are of the same grade and differentiation.
#
Iron, Chronic Liver Disease, and HCC
Iron has an intriguing relation with CLD and HCC. Whereas iron overload can cause CLD and cirrhosis that can further lead to HCC, neoplastic clones of cells that eventually form HCC are devoid of iron. Again iron overload can cause HCC in a morphologically normal liver.
Cirrhotic nodules may store iron and are then called siderotic nodules, which pathologically are early dysplastic nodules.[15] [16] Once these nodules undergo neoplastic change through early and progressed HCC, the neoplastic clone becomes devoid of iron. This is because the neoplastic cells use up iron, making them appear iron free on imaging. The neoplastic cells may also appear iron free due to rapid turnover of cells and apparent lack of available iron for accumulation within the cells.[17] On imaging, a siderotic nodule in a cirrhotic liver is likely to be a dysplastic nodule. Development of an iron-free nodule within this siderotic nodule signals the development of a neoplastic clone. Iron overload can cause chronic hepatocyte injury leading to CLD and cirrhosis. This condition of the liver can cause HCC in a mechanism as described earlier.[18]
HCC can also arise de novo in iron overload conditions such as hereditary hemochromatosis and chronic blood transfusion. The de novo development of HCC in an apparently normal liver can be attributed to free radical–induced oxidative stress injury followed by direct DNA damage as well as suppression of tumor suppressor genes and P53 gene[18] ([Table 6]).
#
Fat, Chronic Liver Disease, and HCC
Fat may be detected in HCC on pathology and imaging. There are different causes for the development of fat in HCC. Steatotic livers can develop HCC. In such cases, fat is found in the HCC nodules, both early and progressed as well as dysplastic nodules.[5] [19] [20]
Inflammation-induced metaplastic processes (which include steatohepatitis) can cause the development of fat within HCC. This inflammatory response may be due to an ischemic change during transition of arterial supply to HCC (early through progressed) from the paired to the unpaired artery. In such cases, fat is present in late dysplastic nodules and early HCC. As the unpaired arterial supply to the HCC resolves the ischemic change, fat within the HCC disappears.[21] [22]
On imaging as we progress from early dysplastic nodules, through late dysplasia and early HCC, the fat content increases either diffusely or within a subnodule. With increasing size and grade, the fat content of the nodule decreases.[5]
The third cause of fat in HCC is its development from an intermediate fat-containing lesion, for example, steatohepatitic adenoma, inflammatory hepatocellular adenoma, and sonic hedgehog hepatocellular adenoma.[21] Unlike the above condition, both early and progressed HCC developing from intermediate fat-containing lesions retain fat throughout grades and size ([Table 7]).
#
HCC Appearance and Morphology on Contrast-Enhanced MRI
Arterial Phase
The arterial phase referred to on imaging of a cirrhotic liver is a late arterial phase where the acquisition is at approximately 25 to 30 seconds after injection of the contrast medium.
Generally, only about 20% of the blood flow to the liver is contributed by the hepatic artery. Hence, in the arterial phase, due to low contribution from the hepatic artery, the liver appears hypointense/hypodense.
HCC typically shows a heterogeneous and mosaic pattern of enhancement on the arterial phase in contrast to the hypodensity/hypointensity of the background liver ([Figs. 4] and [5]). This type of enhancement is called arterial phase hyperenhancement (APHE) and should be differentiated from peripheral rimlike arterial hyperenhancement, which is named rimlike APHE. Differentials can be based on different types of arterial phase enhancement as enumerated in [Table 8] ([Figs. 6],[7],[8],[9]).






|
Mosaic APHE ([Fig. 6]) |
Hepatocellular carcinoma (HCC), fibrolamellar HCC, conglomerated metastasis |
|---|---|
|
Rimlike APHE (targetoid enhancement; [Fig. 7] ) |
Intrahepatic cholangiocarcinoma (IHCC)/metastasis, atypical HCC |
|
Diffuse enhancement ([Fig. 8]) |
Flash filling hemangioma, focal nodular hyperplasia (FNH), hepatic adenoma, small metastasis |
|
Ring enhancement ([Fig. 9]) |
Metastasis, HCC (atypical), IHCC, postinfection/inflammation, ablation |
Abbreviations: APHE, arterial phase hyperenhancement.
Over its development, a cirrhotic nodule grows into a low-grade dysplastic nodule, high-grade dysplastic nodule, early HCC, and progressed HCC. In the course of this spectrum, the portal venous contribution to the nodule withers away and unpaired arterial supply takes precedence. In fact, the portal triads reduce in number as the lesion progresses from a benign nodule to a malignant one and the contribution from the paired arteries also diminishes.
The unpaired arterial contribution to the nodule across its journey from a cirrhotic nodule to a progressed HCC is akin to neovascularization. An important feature of the neo-vessels is the lack of order and pattern. They are also unpaired, meaning they are not accompanied by bile ducts or portal veins as is the norm. The neo-vessels grow in a bizarre fashion and once they are perfused by the hepatic artery in the late arterial phase, the pattern is as bizarre—mosaiclike and heterogeneous. There is no fixed pattern of vessels and hence there is no fixed pattern of enhancement. This hallmark imaging feature defines APHE.
The enhancement of the HCC is more in comparison to the background liver, which is being fed by the regular hepatic artery contributing only 20%. Hence, APHE is more correctly referred to as a phenomenon, in contrast to the background liver parenchymal attenuation/intensity.
The APHE is not only because of unpaired hepatic arterial contribution. Sinusoidal capillarization also contributes to APHE. Sinusoids appear like systemic arteries due to basement membrane formation and loss of fenestration of the endothelium.[23]
The key differential for an arterial phase enhancing nodule in a cirrhotic liver is an IHCC. The usual enhancement pattern in IHCC is a rimlike APHE. The typical enhancement pattern is, as the name suggests, in a rimlike peripheral pattern encompassing a poorly enhancing core. The rim that enhances is densely cellular and is the reason for enhancement. The rim shows restriction on diffusion weighted imaging, confirming its cellularity.
#
Portal Venous Phase
The portal venous phase is typically acquired between 70 and 90 seconds after injection of contrast. The liver is perfused mainly by the portal vein that contributes 80% of the entire flow to the liver. The rest of the blood flow to the liver is by the hepatic artery. In the portal venous phase, the liver appears hyperintense/hyperdense due to high portal venous flow.
An early or progressed HCC will appear hypointense/hypodense in comparison to the background liver, where the portal venous contribution is 80%. This is called the washout phenomenon ([Fig. 10]).

The washout phenomenon is a result of drainage of blood from the nodule by the portal vein. The early and progressed HCC are drained by the portal vein. In the progressed HCC, the hepatic veins also help drain blood from the nodule. The resultant effect of portal vein feeding the background liver rendering it hyperintense/hyperdense and on the contrary draining blood away from the HCC results in the washout phenomenon.
As a result of drainage of blood from the nodule by the portal vein and to a lesser extent the hepatic vein, tumor thrombi are also prone to traverse into the portal and hepatic veins from the respective nodules, resulting in what is known as “tumor in vein” (TIV) in the LI-RADS lexicon.
#
Hepatic Venous Phase
A hepatic venous phase may not be routinely acquired on imaging for HCC. This phase is acquired approximately 120 minutes after injection of the contrast medium.
In the hepatic venous phase, the HCC nodule appears hypointense to the background liver parenchyma. In this phase, the liver is still being perfused by portal venous blood. Since the HCC is being drained by the portal and hepatic veins, it stands out as a hypodense/hypointense nodule in the hepatic venous phase. As mentioned earlier, hepatic venous drainage of blood from HCC facilitates tumor thrombus within the hepatic vein as well.
Capsule is a feature of progressed HCC that is best observed on the venous phase. The capsule does not contain hepatocytes or malignant cells, but consists of a fibrous and a vascular layer. On contrast administration, the vascular layer enhances first. There is delayed enhancement of the fibrous layer and, hence, on the delayed scans after administration of contrast, the capsule is better appreciated ([Figs. 11] and [12]).


The corona phenomena are a feature of progressed HCC. Small portal venules carry blood away from the tumor through the capsule into the adjoining sinusoids, best seen on the delayed arterial phase of the portal venous phase ([Figs. 13] and [14]).


In the portal venous phase, tumors that have infiltrated the venules show enhancement. This leads to an appearance of nodules adjoining the main nodule, also called satellite nodule ([Fig. 15]). Satellite nodules are in actuality intrahepatic metastasis and a feature of progressed HCC.

#
Delayed Hepatobiliary Phase on MRI
The delayed hepatobiliary phase is obtained after 1 to 3 hours in case gadobenate dimeglumine (Gd-BOPTA) is administered, since only 5% of this contrast media shows biliary excretion. Gadoxetate disodium has 50% biliary excretion and hence if this is the contrast administered, the hepatobiliary phase is obtained at 15 to 30 minutes after administration.
The appearance of any lesion on the hepatobiliary phase depends on the expression of the organic anionic transporting peptide (OATP) receptor on the lesion. As a nodule progresses from an early dysplastic nodule to a progressed HCC, the OATP expression falls. Hence, the progressed HCC appears as a hypointense nodule (lack of OATP receptor expression) on the background of a liver that is hyperintense (due to normal expression of OATP receptors of normal hepatocytes; [Fig. 16]).
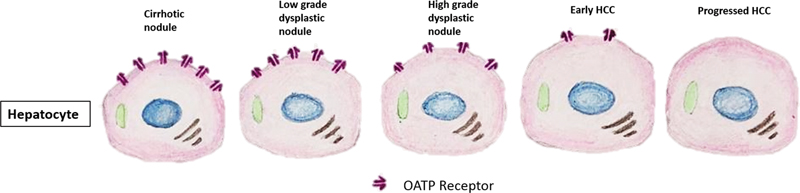
OATP receptor expression is inversely related to the grade of HCC. Hence, low expression of OATP resulting in a hypointense HCC nodule in the hepatobiliary phase indicates poor prognosis[24] [25] ([Fig. 17]).

The above-mentioned hepatocyte-specific contrast agents cannot produce a good hepatobiliary phase imaging in case of jaundice, where bilirubin is above 2 mg/dL. This is because the intracellular uptake of contrast by the diseased hepatocytes is suboptimal and as a result excretion into biliary channels is inadequate.
Gadoxetate disodium is not available in India. Since this contrast has a 50% excretion through the biliary system and the hepatobiliary phase is obtained between 15 and 30 minutes after injection of contrast, an overlap with the portal and hepatic venous phase is evident, also called the transitional phase.
A comparative table of the appearance of the precursor nodules and early and progressed HCC on different phases of contrast study is as tabulated in [Table 9].
Abbreviations: APHE, arterial phase hyperenhancement.
#
#
HCC Appearance and Morphology on Noncontrast MRI
Diffusion Weighted Images
Cellularity is the basis of diffusion restriction for any neoplastic lesion including HCC. HCC is a slow-growing tumor with low cellularity. Moreover, the background cirrhotic liver has a higher diffusion restriction due to fibrosis and as a result the diffusion signal of HCC does not stand out in the background of cirrhosis. Diffusion restriction is thus not a consistent imaging feature for HCC. Diffusion weighted imaging (DWI) is placed as an ancillary feature in the LI-RADS lexicon ([Figs. 18] and [19]).


#
T2 Signal
HCC appears to be an intermediate signal on T2. The lesions are more cellular than the background liver and, along with cellular edema, show an intermediate signal on T2-weighted imaging (T2WI).
A nodule-in-nodule appearance is found in HCC in contrast imaging as well as T1 and T2 sequences. They may also be appreciated on DWI. Pathologically, the larger nodule is a cirrhotic nodule within which there is clonal proliferation of a dysplastic nodule or an early/progressed HCC ([Fig. 19]).
#
In- and Opposed-Phase Images
Fat-containing HCC does occur especially in the background of a fatty liver. NAFLD is the most common risk factor for HCC in the western world. CLD as a result of NAFLD may show HCC with fat contents. This fat may appear as a signal drop in the opposed-phase images ([Fig. 20]). Fat in HCC may also be a result of inflammation-induced metaplastic phenomenon, where fat is produced within the tumor. Intermediate lesions like fat-containing adenomas may convert to HCC and show fatty contents. The fat (macro- and microscopic) signals on MRI and CT are tabulated in [Table 10].

A comparative table of the signals of the precursor nodules and early and progressed HCC is presented in [Table 11].
#
T1 Signal
The T1 signal in HCC can be usually isointense or marginally hyperintense. Since the HCC cell is phenotypically similar to a normal hepatocyte, the HCC cell and the background liver appear similar in T1 signal. This is contrary to a hepatic metastasis that appears markedly hypointense to the background liver, since the metastatic cells are not of liver origin. The marginal hyperintensity of HCC may be attributed to mineral or fatty contents. Hemorrhage is not uncommon in HCC and can also contribute to T1 hyperintensity ([Fig. 21]).

#
#
Newer Variants of HCC
Several new variants of HCC have been described in the World Health Organization Classification System revised in 2019,[26] of which the steatotic variant has already been described earlier. Nearly a third of all HCC can be classified under these new variants and there are prognostic implications[26] [27] and imaging differences as well ([Table 12]).
Abbreviations: AFP, alpha fetoprotein; APHE, arterial phase hyperenhancement.
#
Proliferative and Nonproliferative HCC
Genetic and molecular analyses classify HCC into a proliferative variety with poor prognosis and a nonproliferative variety with good prognosis. Both genetic/molecular and imaging biomarkers can aid in this classification process and are enumerated in [Table 13].
Abbreviations: APHE, arterial phase hyperenhancement; ADC, apparent diffusion coefficient; CTNNB1, catenin beta 1; JAK/STAT, Janus kinase / signal transducers and activators of transcription; TP53, tumor protein 53; VEGF, vascular endothelial growth factor
#
Conclusion
Diagnosis of HCC has achieved significant specificity after incorporation of the LI-RADS system of standardized reporting. Understanding the pathological basis of the observation of LI-RADS is important for the radiologist to communicate effectively with pathologists and clinical colleagues for better diagnosis and management of HCC.
#
#
Conflict of Interest
None declared.
-
References
- 1 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68 (06) 394-424
- 2 Trevisani F, Cantarini MC, Wands JR, Bernardi M. Recent advances in the natural history of hepatocellular carcinoma. Carcinogenesis 2008; 29 (07) 1299-1305
- 3 Sagnelli E, Macera M, Russo A, Coppola N, Sagnelli C. Epidemiological and etiological variations in hepatocellular carcinoma. Infection 2020; 48 (01) 7-17
- 4 McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology 2021; 73 (Suppl (Suppl. 01) 4-13
- 5 Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part I. Development, growth, and spread: key pathologic and imaging aspects. Radiology 2014; 272 (03) 635-654
- 6 Tarao K, Nozaki A, Ikeda T. et al. Real impact of liver cirrhosis on the development of hepatocellular carcinoma in various liver diseases-meta-analytic assessment. Cancer Med 2019; 8 (03) 1054-1065
- 7 Chernyak V, Fowler KJ, Kamaya A. et al. Liver Imaging Reporting and Data System (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology 2018; 289 (03) 816-830
- 8 Katabathina VS, Khanna L, Surabhi VR. et al. Morphomolecular classification update on hepatocellular adenoma, hepatocellular carcinoma, and intrahepatic cholangiocarcinoma. Radiographics 2022; 42 (05) 1338-1357
- 9 El-Serag HB. Hepatocellular carcinoma. N Engl J Med 2011; 365 (12) 1118-1127
- 10 Baffy G, Brunt EM, Caldwell SH. Hepatocellular carcinoma in non-alcoholic fatty liver disease: an emerging menace. J Hepatol 2012; 56 (06) 1384-1391
- 11 McGlynn KA, London WT. The global epidemiology of hepatocellular carcinoma: present and future. Clin Liver Dis 2011; 15 (02) 223-243, vii–x .
- 12 van Malenstein H, van Pelt J, Verslype C. Molecular classification of hepatocellular carcinoma anno 2011. Eur J Cancer 2011; 47 (12) 1789-1797
- 13 Taguchi K, Asayama Y, Aishima S. et al. Morphologic approach to hepatocellular carcinoma development in man: de novo or the so-called “dysplastic nodule-carcinoma” sequence?. Oncol Rep 2002; 9 (04) 737-743
- 14 Toyoda H, Hiraoka A, Uojima H. et al. Characteristics and prognosis of de novo hepatocellular carcinoma after sustained virologic response. Hepatol Commun 2021; 5 (07) 1290-1299
- 15 International Consensus Group for Hepatocellular NeoplasiaThe International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology 2009; 49 (02) 658-664
- 16 Terada T, Kadoya M, Nakanuma Y, Matsui O. Iron-accumulating adenomatous hyperplastic nodule with malignant foci in the cirrhotic liver. Histopathologic, quantitative iron, and magnetic resonance imaging in vitro studies. Cancer 1990; 65 (09) 1994-2000
- 17 Gurusamy K. Trace element concentration in primary liver cancers: a systematic review. Biol Trace Elem Res 2007; 118 (03) 191-206
- 18 Fargion S, Valenti L, Fracanzani AL. Role of iron in hepatocellular carcinoma. Clin Liver Dis (Hoboken) 2014; 3 (05) 108-110
- 19 Inui S, Kondo H, Tanahashi Y. et al. Steatohepatitic hepatocellular carcinoma: imaging findings with clinicopathological correlation. Clin Radiol 2021; 76 (02) 160.e15-160.e25
- 20 Salomao M, Remotti H, Vaughan R, Siegel AB, Lefkowitch JH, Moreira RK. The steatohepatitic variant of hepatocellular carcinoma and its association with underlying steatohepatitis. Hum Pathol 2012; 43 (05) 737-746
- 21 Olofson AM, Gonzalo DH, Chang M, Liu X. Steatohepatitic variant of hepatocellular carcinoma: a focused review. Gastroenterol Res 2018; 11 (06) 391-396
- 22 Kutami R, Nakashima Y, Nakashima O, Shiota K, Kojiro M. Pathomorphologic study on the mechanism of fatty change in small hepatocellular carcinoma of humans. J Hepatol 2000; 33 (02) 282-289
- 23 Park YN, Yang CP, Fernandez GJ, Cubukcu O, Thung SN, Theise ND. Neoangiogenesis and sinusoidal “capillarization” in dysplastic nodules of the liver. Am J Surg Pathol 1998; 22 (06) 656-662
- 24 Kitao A, Matsui O, Yoneda N. et al. The uptake transporter OATP8 expression decreases during multistep hepatocarcinogenesis: correlation with gadoxetic acid enhanced MR imaging. Eur Radiol 2011; 21 (10) 2056-2066
- 25 Kogita S, Imai Y, Okada M. et al. Gd-EOB-DTPA-enhanced magnetic resonance images of hepatocellular carcinoma: correlation with histological grading and portal blood flow. Eur Radiol 2010; 20 (10) 2405-2413
- 26 Vij M, Calderaro J. Pathologic and molecular features of hepatocellular carcinoma: an update. World J Hepatol 2021; 13 (04) 393-410
- 27 Torbenson MS. Hepatocellular carcinoma: making sense of morphological heterogeneity, growth patterns, and subtypes. Hum Pathol 2021; 112: 86-101
Address for correspondence
Publikationsverlauf
Artikel online veröffentlicht:
17. April 2023
© 2023. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68 (06) 394-424
- 2 Trevisani F, Cantarini MC, Wands JR, Bernardi M. Recent advances in the natural history of hepatocellular carcinoma. Carcinogenesis 2008; 29 (07) 1299-1305
- 3 Sagnelli E, Macera M, Russo A, Coppola N, Sagnelli C. Epidemiological and etiological variations in hepatocellular carcinoma. Infection 2020; 48 (01) 7-17
- 4 McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology 2021; 73 (Suppl (Suppl. 01) 4-13
- 5 Choi JY, Lee JM, Sirlin CB. CT and MR imaging diagnosis and staging of hepatocellular carcinoma: part I. Development, growth, and spread: key pathologic and imaging aspects. Radiology 2014; 272 (03) 635-654
- 6 Tarao K, Nozaki A, Ikeda T. et al. Real impact of liver cirrhosis on the development of hepatocellular carcinoma in various liver diseases-meta-analytic assessment. Cancer Med 2019; 8 (03) 1054-1065
- 7 Chernyak V, Fowler KJ, Kamaya A. et al. Liver Imaging Reporting and Data System (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology 2018; 289 (03) 816-830
- 8 Katabathina VS, Khanna L, Surabhi VR. et al. Morphomolecular classification update on hepatocellular adenoma, hepatocellular carcinoma, and intrahepatic cholangiocarcinoma. Radiographics 2022; 42 (05) 1338-1357
- 9 El-Serag HB. Hepatocellular carcinoma. N Engl J Med 2011; 365 (12) 1118-1127
- 10 Baffy G, Brunt EM, Caldwell SH. Hepatocellular carcinoma in non-alcoholic fatty liver disease: an emerging menace. J Hepatol 2012; 56 (06) 1384-1391
- 11 McGlynn KA, London WT. The global epidemiology of hepatocellular carcinoma: present and future. Clin Liver Dis 2011; 15 (02) 223-243, vii–x .
- 12 van Malenstein H, van Pelt J, Verslype C. Molecular classification of hepatocellular carcinoma anno 2011. Eur J Cancer 2011; 47 (12) 1789-1797
- 13 Taguchi K, Asayama Y, Aishima S. et al. Morphologic approach to hepatocellular carcinoma development in man: de novo or the so-called “dysplastic nodule-carcinoma” sequence?. Oncol Rep 2002; 9 (04) 737-743
- 14 Toyoda H, Hiraoka A, Uojima H. et al. Characteristics and prognosis of de novo hepatocellular carcinoma after sustained virologic response. Hepatol Commun 2021; 5 (07) 1290-1299
- 15 International Consensus Group for Hepatocellular NeoplasiaThe International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatology 2009; 49 (02) 658-664
- 16 Terada T, Kadoya M, Nakanuma Y, Matsui O. Iron-accumulating adenomatous hyperplastic nodule with malignant foci in the cirrhotic liver. Histopathologic, quantitative iron, and magnetic resonance imaging in vitro studies. Cancer 1990; 65 (09) 1994-2000
- 17 Gurusamy K. Trace element concentration in primary liver cancers: a systematic review. Biol Trace Elem Res 2007; 118 (03) 191-206
- 18 Fargion S, Valenti L, Fracanzani AL. Role of iron in hepatocellular carcinoma. Clin Liver Dis (Hoboken) 2014; 3 (05) 108-110
- 19 Inui S, Kondo H, Tanahashi Y. et al. Steatohepatitic hepatocellular carcinoma: imaging findings with clinicopathological correlation. Clin Radiol 2021; 76 (02) 160.e15-160.e25
- 20 Salomao M, Remotti H, Vaughan R, Siegel AB, Lefkowitch JH, Moreira RK. The steatohepatitic variant of hepatocellular carcinoma and its association with underlying steatohepatitis. Hum Pathol 2012; 43 (05) 737-746
- 21 Olofson AM, Gonzalo DH, Chang M, Liu X. Steatohepatitic variant of hepatocellular carcinoma: a focused review. Gastroenterol Res 2018; 11 (06) 391-396
- 22 Kutami R, Nakashima Y, Nakashima O, Shiota K, Kojiro M. Pathomorphologic study on the mechanism of fatty change in small hepatocellular carcinoma of humans. J Hepatol 2000; 33 (02) 282-289
- 23 Park YN, Yang CP, Fernandez GJ, Cubukcu O, Thung SN, Theise ND. Neoangiogenesis and sinusoidal “capillarization” in dysplastic nodules of the liver. Am J Surg Pathol 1998; 22 (06) 656-662
- 24 Kitao A, Matsui O, Yoneda N. et al. The uptake transporter OATP8 expression decreases during multistep hepatocarcinogenesis: correlation with gadoxetic acid enhanced MR imaging. Eur Radiol 2011; 21 (10) 2056-2066
- 25 Kogita S, Imai Y, Okada M. et al. Gd-EOB-DTPA-enhanced magnetic resonance images of hepatocellular carcinoma: correlation with histological grading and portal blood flow. Eur Radiol 2010; 20 (10) 2405-2413
- 26 Vij M, Calderaro J. Pathologic and molecular features of hepatocellular carcinoma: an update. World J Hepatol 2021; 13 (04) 393-410
- 27 Torbenson MS. Hepatocellular carcinoma: making sense of morphological heterogeneity, growth patterns, and subtypes. Hum Pathol 2021; 112: 86-101