
Subscribe to RSS
DOI: 10.1055/s-0042-1756137
A Three-Dimensional Scale for the Qualitative and Quantitative Assessments of Secondary Alveolar Bone Grafting (SABG) in Unilateral Cleft Lip and Palate Patients Using Cone-Beam Computed Tomography (CBCT)


Abstract
Background The objective of our study was to derive an objective assessment scale for three-dimensional (3D) qualitative and quantitative evaluation of secondary alveolar bone grafting (SABG) using cone-bone computed tomography (CBCT) in patients with unilateral cleft lip and palate (UCLP).
Methods CBCT scans for pre- and 3-month post-SABG were reviewed for bone volume, height, width, and density of the bony bridge formed in the cleft defect in 20 patients with UCLP. Basic descriptive and principal component analysis was used to extract the various sub-components of the scale. Spearman's correlation was used to check the validity of the scale, and intra-class coefficient (ICC) and Cronbach's α were calculated to establish the reliability and retest applicability of the scale.
Results Each CBCT scan was assessed in five areas: cementoenamel junction (CEJ), root apex, root midpoint, 3 and 6 mm below CEJ, and tabulated in percentiles of 20, 25, 40, 50, 60, and 75 for all the parameters (bone volume, density, and width). These scores were validated when correlated to the scale given by Kamperos et al. Cronbach's α for the domains demonstrated acceptable to excellent internal consistency. The ICC showed good test–retest reliability having a range of scores from 0.89 to 0.94.
Conclusion The proposed scale for the 3D assessment of SABG in patients with UCLP provides gradation for the objective assessment of the bony bridge. This gradation enables the qualitative and quantitative assessments of the bony bridge, thus allowing each clinician to judge SABG more conclusively.
#
Introduction
Cleft lip and palate (CLP) is a craniofacial defect arising due to non-fusion of the developmental processes of the face.[1] The sites most affected are the lip, alveolar process, and the palate, with the osseous defect of alveolar process comprising the maximum involvements. Children with this anomaly require multidisciplinary care from birth to adulthood.[2] [3] [4] [5]
Secondary alveolar bone grafting (SABG) has been a standard treatment as a means of repairing the alveolar defect, with the main objective being the formation of bone bridge and making the path for spontaneous tooth eruption through the grafted bone.[6] [7] SABG performed before canine eruption has shown a better dental outcome with fewer adverse effects than that performed post-canine eruption.[8] Furthermore, it is essential to ascertain the status and volume of the bony bridge if the orthodontic movement of the canine into the grafted bone has been planned.[4] [9] Thus, accurate radiological diagnosis and follow-up of SABG is essential.[6] [10]
Cone-bone computed tomography (CBCT) images provide information about volumetric details of the area which is useful in assessing the quantity and quality of the grafted bone, three-dimensional (3D) morphology of the bony architecture formed in the cleft defect, and relationships between the bone bridge and teeth adjacent to the cleft.[11] [12] [13] [14] [15] Orthodontic tooth movement and implant placement can be determined and planned by using the post-SABG CBCT scans. The lower radiation dose to the patients has also been a considerable factor for clinicians preferring CBCT imaging over multi-slice CT.[12] [16] [17] Recent systematic reviews and literature search on 3D radiological evaluation[18] [19] and comparison of 2D and 3D radiological evaluation[11] [20] of SABG in CLP have highlighted the need to develop a cut-off score to decide the amount of bone resorption and serve as a guideline to quantify the outcome of bone graft in a standardized way. Therefore, there is a need to establish a 3D radiographic assessment scale, which provides gradation for the qualitative and quantitative assessments of the bony bridge and resolves the problems of 2D imaging.
The present study was conducted to formulate a 3D radiographic assessment scale using CBCT after SABG in patients with unilateral cleft lip and palate (UCLP), through volumetric, densitometric, and linear assessment at five different root levels on the tooth mesial to the cleft defect.
#
Materials and Methods
The present single-blinded prospective study was approved by the institutional ethical board (I***/I***C/201***1/1*) and was registered in the Clinical Trials Registry (C***/201*/0*/1***2). All the participants were provided with a detailed description of the study, and written informed consent prepared according to the Declaration of Helsinki was obtained prior to their induction in the study. Patients with UCLP between the age group of 7 and 10 years without any history of previous alveolar bone grafting (ABG) were included. Presurgical orthodontics was initiated in patients requiring the expansion of the maxillary arch for the improvement of inter-arch coordination and for the correct estimation of the volume of the cleft defect.[3] [4] All the patients received an autogenous cancellous bone graft from the anterior iliac crest, and the surgical procedure was performed at the hospital by the same surgeon with vast experience of performing SABG.[21] Postoperative instructions for the maintenance and healing of the surgical wound were given in a verbal and written form. Post-SABG CBCT assessment was performed after 3 months to assess the status of the bone graft.[22] Patients with any associated syndromes or with incomplete cleft were excluded from the study.
Evaluation Procedure
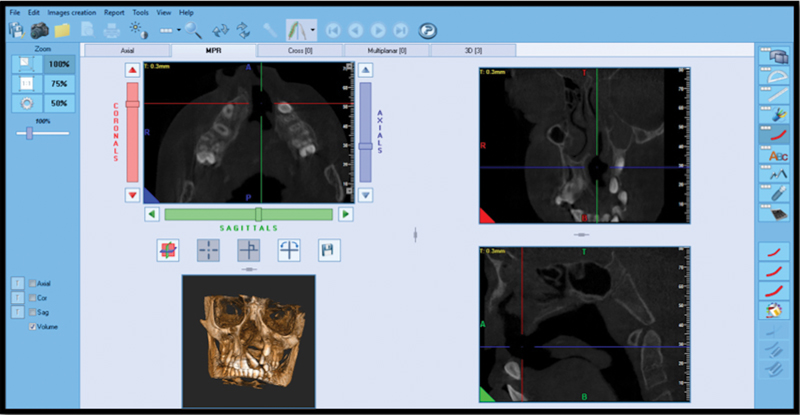
Preoperative and post-SABG high-resolution CBCT scans (NewTom GiANO HR, Italy) with the imaging parameters of 80 kVp, 5 mA, 18 s delivering high-resolution images of 0.3 mm slice thickness with a field of view of 13 × 16 cm were obtained.[23] Patient position was standardized using light markers, with transverse plane parallel to Frankfort horizontal line (mid-sagittal plane and Frankfort plane) of the machine. To protect from scattered radiation, patients were made to wear a thyroid collar and lead apron. The Digital Imaging and Communications in Medicine (DICOM) images of the CBCT scans were evaluated by importing in New Net Technologies software ([Fig. 1]). The scans were coordinated in all three planes along the long axis of the tooth (coronal, sagittal, and axial planes) for the standardization of assessment and to minimize any error. The tooth mesial to the cleft area was identified, and the measurements were taken at the following levels:
-
Cervical slice—cementoenamel junction (CEJ).
-
Intermediate slice—middle point of the root.
-
Apical slice—apex of the root.
-
3 mm below CEJ.
-
6 mm below CEJ.
#
Volumetric Evaluation Procedure[13] [24]
Panoramic reconstruction was done from the CBCT images, and regions of interest were selected. The volume of alveolar cleft defect in each slice was calculated (in cubic millimeter) by multiplying the alveolar cleft defect area by the slice thickness (0.3 mm) and adding the volume of each section to calculate the total volume of the alveolar cleft defect. Volume was calculated at two time intervals: V0—volume of the cleft defect before SABG and V1—volume after 3 months of SABG. Measurements of volume change were measured by taking the difference between alveolar cleft defect volumes at V0 and V1.
#
Density Evaluation Procedure[25] [26]
After volumetric evaluation, 2D densitometric measurements were performed for each axial section. The mean value of density was calculated for all sections and reported in Hounsfield units (HU). The mean value of density was calculated to evaluate the quality of alveolar bone graft in two time intervals: D0—mean value of bone density in the region of cleft defect before SABG and D1—mean value of bone density after 3-month SABG. The conversion ratio for transforming the gray density values of CBCT (voxel values) into HU was conceivable due to this linear correlation. The conversion ratio was approximately 0.7 (0.7 × values of CBCT = values of CT) in the present study.
#
Width Evaluation Procedure[27]
The mean value of width was calculated at all the five levels as defined previously to evaluate the quantity of alveolar bone graft in two time intervals. Mean difference in the width of the alveolar bone was calculated by the difference at the two time interval (W1 − W0) (mean value of the width of the cleft defect region after 3 months of SABG − mean value of the width of the cleft defect region before SABG).
The assessment of SABG was done by assigning a score based on radiographic changes in bone volume, density, and width of cleft defect, from which an index was formulated with their respective grades ([Fig. 2]).

#
Statistical Analysis
The sample size was determined with the help of G*Power software (version 3.1.9.6), the power of the study kept at 95% with a significance level of 5% (a = 0.05) and effect size at 1.51, calculated based upon the mean and standard deviation (SD) of the previous study (860 ± 350 mm3).[28] The required sample size was calculated to be 16 patients and, considering a dropout of 20% in follow-up, the sample size was taken to be 20 patients.
All the parameters of the patients were summarized as mean and SD. The data were collected and tabulated in Microsoft Excel 365 and statistically analyzed using the Statistical Package for Social Sciences software (Version 21.0).
To define the success versus failure of SABG, results were tabulated in percentiles of 20, 25, 40, 50, 60, and 75. After measuring all the parameters of cleft defect (e.g., bone volume, density, and width), each patient was assigned their respective score in five areas: CEJ, root apex, root midpoint, 3 mm, and 6 mm below CEJ.
#
Scale Derivation
A sampling adequacy test was performed for all the parameters, and principal component analysis was applied. Principal component analysis is an adaptive data analysis technique where the variants of the technique have been developed that are tailored to various different data types and structures. Thus, principal component analysis for volume, width, and density with and without varimax rotation classified the patterns of alveolar bone distribution in cleft patients and derived the sub-components of the scale.
#
Validation
After measuring all the parameters of cleft defect (like bone volume, density, height, and width), each patient was assigned their respective score, which was corroborated by the scale, as suggested by Kamperos et al.[30] Spearman's correlation was used to calculate the correlation between the two scales and establish the validity of the new scale.
#
Scale Reliability
Using the same scale, the readings were repeated after 2 weeks by the same investigator. Intra-class coefficient (ICC) and Cronbach's α were calculated to establish the reliability and test–retest applicability of the new scale.
#
#
Results
Bone Volume
The mean volume of bone in the area of cleft defect was 41.28 ± 84.46, 31.91 ± 37.77, 18.49 ± 22.88, 43.06 ± 45.39, and 29.28 ± 37.08 mm3 at CEJ, mid-point, apex, below 3 mm CEJ, and below 6 mm CEJ at T0 which subsequently increased to 103.01 ± 49.57, 74.72 ± 55.81, 44.71 ± 33.93, 88.07 ± 70.73, and 82.81 ± 59.15 mm3 at CEJ, mid-point, apex, below 3 mm CEJ and below 6 mm CEJ at T1 time interval, respectively ([Table 1]). The high variability in the bone volume noted in the pretreatment stage of the patients with UCLP indicates the inconsistency with which the cleft defect is clinically present.
Abbreviations: CEJ; cementoenamel junction; HU, Hounsfield units; SABG; secondary alveolar bone grafting.
#
Bone Density
The mean bone density in the unaffected side was 821.66 ± 282.21 HU, and the mean bone density in the cleft area was 581.33 ± 215.51 HU at T0 ([Table 2]). The mean bone density was found to be 600.23 ± 240.13, 541.96 ± 274.37, 573.966 ± 274.95, 580.53 ± 255.26, and 612.10 ± 277.06 HU, at CEJ, mid-point, apex, 3 mm below CEJ, and 6 mm below CEJ, respectively, at T0. The mean bone density was 791.90 ± 170.43, 782.36 ± 221.50, 759.40 ± 274.95, 815.46 ± 184.94, and 766.20 ± 251.63, at CEJ, mid-point, apex, 3 mm below CEJ, and 6 mm below CEJ, respectively, at T1.
Abbreviations: HU, Hounsfield units; SD, standard deviation.
#
Bone Width
The mean value of width was calculated for all sections, and the mean bone width in cleft defect was 3.89 ± 1.11, 3.07 ± 1.16, 4.18 ± 1.90, 4.24 ± 1.97, and 3.23 ± 0.65 mm at CEJ, mid-point, apex, below 3 mm CEJ, and below 6 mm CEJ, respectively, at T0. The mean bone width in the grafted area was 9.21 ± 0.60, 9.05 ± 0.85, 9.65 ± 0.76, 9.54 ± 1.17, and 9.44 ± 0.93 mm at CEJ, mid-point, apex, below 3 mm CEJ and below 6 mm CEJ, respectively, at T1 ([Table 1]).
Furthermore, evaluating the root coverage with the teeth mesial to the cleft defect in the present study, initially, five patients (25%) had more than three-fourth bone bridge at T0, which improved in 13 patients (65%) after SABG (at T1). Similarly, nine patients (45%) had less than half bone bridge or no bone bridge at T0 which improved after SABG with only one patient (5%) presenting with less than half bone bridge ([Table 3]).
|
Scale |
Time interval |
Frequency |
Percent |
|---|---|---|---|
|
Frequency and percentage of height score |
|||
|
No bridge |
T0 |
2 |
10.0 |
|
T1 |
0 |
0.0 |
|
|
Less than one-fourth |
T0 |
1 |
5.0 |
|
T1 |
0 |
0.0 |
|
|
One-fourth to half |
T0 |
6 |
30.0 |
|
T1 |
1 |
5.0 |
|
|
Half to three-fourth |
T0 |
6 |
30.0 |
|
T1 |
6 |
30.0 |
|
|
More than three-fourth |
T0 |
5 |
25.0 |
|
T1 |
13 |
65.0 |
|
|
Frequency and percentage of width score |
|||
|
No bridge |
T0 |
2 |
10.0 |
|
T1 |
0 |
0.0 |
|
|
Less than half |
T0 |
4 |
20.0 |
|
T1 |
2 |
10.0 |
|
|
More than half |
T0 |
14 |
70.0 |
|
T1 |
18 |
90.0 |
|
Scale derivation results showed a value of 0.745 with the Kaiser–Meyer–Olkin measure, indicating that the scale formed in this study was acceptable. Principal component analysis yielded five sub-scales for volume and density: (1) at CEJ, (2) at apex, (3) at mid-point, (4) 3 mm below CEJ, and (5) 6 mm below CEJ; and two sub-scales: (1) coronal half and (2) radicular half for width[29] ([Table 4]).
Abbreviation: CEJ; cementoenamel junction.
Based upon the present study, a new scale ([Table 5]) is proposed for the 3D radiographic assessment of SABG, preferred in patients of 7 to 10 years with the CBCT scan after 3 months.
Abbreviation: HU, Hounsfield units.
#
Scale Validation[30]
The Spearman coefficient ranged from 0.58 for the width component to 0.72 for the height component. The respective correlations were statistically significant (p < 0.05), indicating good criterion validity and discriminant validity.
#
Scale Reliability
The range for Cronbach's α[31] for the domains was from 0.84 for density to 0.89 for width measurements, thereby demonstrating acceptable to excellent internal consistency. The ICC showed good test–retest reliability having a range of scores from 0.89 to 0.94.
#
#
Discussion
SABG has been the mainstay surgical treatment modality for the treatment of the alveolar defect in patients with CLP. Semb[32] advocated that the optimal time for alveolar cleft grafting is between the ages of 9 and 11 years (before the eruption of the canine when the root is half to two-third formed). Furthermore, 95% of the anteroposterior and transverse growth is completed by the age of 8 years. In the present study, SABG was performed on 20 patients between the ages of 7 and 10 years (mean age 8.1 ± 1.4 years). However, it is pertinent to note that the correct age of the SABG is dependent upon the radiographic evaluation of the lateral incisor and canine associated with the cleft defect, rather than the chronological age of the patient. Additionally, amidst no definitive conclusion of early (5–7 years) or late (8–12 years) SABG providing better treatment outcome, a mixed age group of patients from 7 to 10 years were taken depending upon the status of the erupting canine.[8] [33] [34]
The radiographic CBCT assessment measured the volume, density, and width of the bony bridge in the region of the cleft defect at five different root levels of the tooth mesial to the cleft defect as suggested by Garcia et al[33] and Gomes et al.[35]
CBCT is more precise, reliable, and reproducible as compared with 2D radiographs and, therefore, could be used for volumetric and densitometric evaluation for the success of SABG.[18] [23] [24] [36] Furthermore, volumetric assessment using CBCT with a slice thickness of 0.3 mm is found to be more accurate as compared with conventional CT which tends to overestimate the bony defect with increased radiation exposure.[13] [15] [26]
The postoperative assessment of the grafted bone was done 3 months (T1) after performing SABG. The assessment of the bone graft should preferably be performed at this stage, as the grafted bone transforms into the normal trabecular bone by 3 months, and results indicate that the alveolar bone density remains stable between 3 and 6 months.[22] [32] Furthermore, it has been suggested that subsequent orthodontic or prosthetic implants should be placed at this stage as bone height level starts to decline after 3 months of ABG.[22]
Bone density has been classically described in the gray values (GV) obtained from classic CT examination and quantified in HU.[16] Development in CBCT imaging, as well as the use of advanced GV correction techniques, have increased the potential of applying CBCT-derived GVs, such as CT-derived HU.[37] The mean bone density in the unaffected side was measured to be 821.66 ± 282.21 HU, whereas the mean bone density in the grafted area was 581.33 ± 215.51 HU at T1. The minimum density in the unaffected side was 203 HU, and in the grafted area was 135 HU, while the maximum density in the unaffected side was 1,171 HU and in the grafted area was 875 HU. The present findings correlate with the studies of Zhang et al,[22] who evaluated radiographic bone density where bone density D3 350 to 850 HU is more common in maxilla. The mean density of grafted bone at T1 was 581.33 ± 251.51 HU.
In evaluating the bone width in the cleft defect among the 20 patients, 14 patients (70%) had more than half bone width at T0, which later improved in 18 patients (90%) after SABG at T1. Six patients had less than half bone width at T0 which later improved after SABG for four patients (20%) at T1, where there was more than half of the bone width present.
Based upon the percentile distribution of the pre- and post-SABG values of each respective domain, a new gradation-based scale is formulated for a 3D radiographic assessment scale of SABG, preferred in patients of 7 to 10 years with the CBCT scan after 3 months ([Table 5]). Few studies have attempted to set thresholds for characterizing a good postsurgical outcome; however, these studies do not provide a single success scale that considers both qualitative and quantitative aspects of the bony bridge. The respective gradations would allow for objective-based assessments of each individual parameter.
In describing the success versus failure, there was a reasonably good agreement present between the new CBCT scale and the scale given by Kamperos et al.[30] In the present study, 90% of patients were defined as successful after the SABG.
The present study sets a success scale for the outcome evaluation of SABG on an objective gradation-based assessment in all the respective domains (bone volume, bone density, and bone width). The new scale also provides accurate, qualitative, and quantitative assessments on the 3D morphology of the repaired alveolar process (bone volume, bone density, bone height, and bone width).
Limitations and Future Scope
The use of the present scale on a larger treatment group would provide validation on the scale; furthermore, the correlation of the gradation post-SABG with the long-term stability of teeth and clinical success of treatment would provide the scale a prognostic component as well.
#
#
Conclusion
The present scale provides gradation-based qualitative (bone density) and quantitative (bone volume and width) assessments of the bony bridge formed after SABG for the better understanding of both orthodontists and surgeons, thus allowing to judge the prognosis of each SABG case more conclusively.
#
#
Conflict of Interest
None declared.
-
References
- 1 Dixon MJ, Marazita ML, Beaty TH, Murray JC. Cleft lip and palate: understanding genetic and environmental influences. Nat Rev Genet 2011; 12 (03) 167-178
- 2 Mossey PA, Little J, Munger RG, Dixon MJ, Shaw WC. Cleft lip and palate. Lancet 2009; 374 (9703): 1773-1785
- 3 Ma L, Hou Y, Liu G, Zhang T. Effectiveness of presurgical orthodontics in cleft lip and palate patients with alveolar bone grafting: a systematic review. J Stomatol Oral Maxillofac Surg 2021; 122 (01) 13-17
- 4 Chang C-S, Wallace CG, Hsiao Y-C. et al. Difference in the surgical outcome of unilateral cleft lip and palate patients with and without pre-alveolar bone graft orthodontic treatment. Sci Rep 2016; 6: 23597
- 5 Freitas JA, Garib DG, Oliveira M. et al. Rehabilitative treatment of cleft lip and palate: experience of the hospital for rehabilitation of craniofacial anomalies-USP (HRAC-USP)—part 2: pediatric dentistry and orthodontics. J Appl Oral Sci 2012; 20 (02) 268-281
- 6 Boyne PJ, Sands NR. Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg 1972; 30 (02) 87-92
- 7 Abyholm FE, Bergland O, Semb G. Secondary bone grafting of alveolar clefts. A surgical/orthodontic treatment enabling a non-prosthodontic rehabilitation in cleft lip and palate patients. Scand J Plast Reconstr Surg 1981; 15 (02) 127-140
- 8 Vandersluis YR, Fisher DM, Stevens K, Tompson BD, Lou W, Suri S. Comparison of dental outcomes in patients with nonsyndromic complete unilateral cleft lip and palate who receive secondary alveolar bone grafting before or after emergence of the permanent maxillary canine. Am J Orthod Dentofacial Orthop 2020; 157 (05) 668-679
- 9 Wirthlin JO. The orthodontist's role in the management of patients with cleft lip and palate undergoing alveolar bone grafting. Semin Orthod 2017; 23 (03) 268-278
- 10 Hynes PJ, Earley MJ. Assessment of secondary alveolar bone grafting using a modification of the Bergland grading system. Br J Plast Surg 2003; 56 (07) 630-636
- 11 Feichtinger M, Zemann W, Mossböck R, Kärcher H. Three-dimensional evaluation of secondary alveolar bone grafting using a 3D-navigation system based on computed tomography: a two-year follow-up. Br J Oral Maxillofac Surg 2008; 46 (04) 278-282
- 12 Hamada Y, Kondoh T, Noguchi K. et al. Application of limited cone beam computed tomography to clinical assessment of alveolar bone grafting: a preliminary report. Cleft Palate Craniofac J 2005; 42 (02) 128-137
- 13 Oberoi S, Chigurupati R, Gill P, Hoffman WY, Vargervik K. Volumetric assessment of secondary alveolar bone grafting using cone beam computed tomography. Cleft Palate Craniofac J 2009; 46 (05) 503-511
- 14 Dissaux C, Bodin F, Grollemund B. et al. Evaluation of success of alveolar cleft bone graft performed at 5 years versus 10 years of age. J Craniomaxillofac Surg 2016; 44 (01) 21-26
- 15 Parveen S, Husain A, Mascarenhas R, Reddy SG. Clinical utility of cone-beam computed tomography in patients with cleft lip palate: current perspectives and guidelines. J Cleft Lip Palate Craniofacial Anomalies 2018; 5 (02) 74-87
- 16 Spin-Neto R, Gotfredsen E, Wenzel A. Impact of voxel size variation on CBCT-based diagnostic outcome in dentistry: a systematic review. J Digit Imaging 2013; 26 (04) 813-820
- 17 Kamburoğlu K, Murat S, Kolsuz E, Kurt H, Yüksel S, Paksoy C. Comparative assessment of subjective image quality of cross-sectional cone-beam computed tomography scans. J Oral Sci 2011; 53 (04) 501-508
- 18 De Mulder D, Cadenas de Llano-Pérula M, Jacobs R, Verdonck A, Willems G. Three-dimensional radiological evaluation of secondary alveolar bone grafting in cleft lip and palate patients: a systematic review. Dentomaxillofac Radiol 2018; 48 (01) 20180047
- 19 Stasiak M, Wojtaszek-Słomińska A, Racka-Pilszak B. Current methods for secondary alveolar bone grafting assessment in cleft lip and palate patients—a systematic review. J Craniomaxillofac Surg 2019; 47 (04) 578-585
- 20 Yu X, Guo R, Li W. Comparison of 2- and 3-dimensional radiologic evaluation of secondary alveolar bone grafting of clefts: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol 2020; 130 (04) 455-463
- 21 Semb G, Brattström V, Mølsted K. et al. The Eurocleft study: intercenter study of treatment outcome in patients with complete cleft lip and palate. Part 4: relationship among treatment outcome, patient/parent satisfaction, and the burden of care. Cleft Palate Craniofac J 2005; 42 (01) 83-92
- 22 Zhang DZ, Xiao WL, Zhou R, Xue LF, Ma L. Evaluation of bone height and bone mineral density using cone beam computed tomography after secondary bone graft in alveolar cleft. J Craniofac Surg 2015; 26 (05) 1463-1466
- 23 Koç A, Kaya S. Is it possible to estimate volume of bone defects formed on dry sheep mandibles more practically by secondarily reconstructing section thickness of cone beam computed tomography images?. Dentomaxillofac Radiol 2021; 50 (03) 20200400
- 24 Barbosa GLR, Wood JS, Pimenta LA, de Almeida SM, Tyndall DA. Comparison of different methods to assess alveolar cleft defects in cone beam CT images. Dentomaxillofac Radiol 2016; 45 (02) 20150332
- 25 Pauwels R, Jacobs R, Singer SR, Mupparapu M. CBCT-based bone quality assessment: are Hounsfield units applicable?. Dentomaxillofac Radiol 2015; 44 (01) 20140238
- 26 Cassetta M, Stefanelli LV, Pacifici A, Pacifici L, Barbato E. How accurate is CBCT in measuring bone density? A comparative CBCT-CT in vitro study. Clin Implant Dent Relat Res 2014; 16 (04) 471-478
- 27 Witherow H, Cox S, Jones E, Carr R, Waterhouse N. A new scale to assess radiographic success of secondary alveolar bone grafts. Cleft Palate Craniofac J 2002; 39 (03) 255-260
- 28 Barbosa GLR, Emodi O, Pretti H. et al. GAND classification and volumetric assessment of unilateral cleft lip and palate malformations using cone beam computed tomography. Int J Oral Maxillofac Surg 2016; 45 (11) 1333-1340
- 29 Lever J, Krzywinski M, Altman N. Principal component analysis. Nat Methods 2017; 14 (07) 641-642
- 30 Kamperos G, Theologie-Lygidakis N, Tsiklakis K, Iatrou I. A novel success scale for evaluating alveolar cleft repair using cone-beam computed tomography. J Craniomaxillofac Surg 2020; 48 (04) 391-398
- 31 Tavakol M, Dennick R. Making sense of Cronbach's alpha. Int J Med Educ 2011; 2: 53-55
- 32 Semb G. Effect of alveolar bone grafting on maxillary growth in unilateral cleft lip and palate patients. Cleft Palate J 1988; 25 (03) 288-295
- 33 Garcia MA, Yatabe M, Fuzer TU, Calvo AM, Trindade-Suedam IK. Ideal versus late secondary alveolar bone graft surgery: a bone-thickness cone-beam computed tomographic assessment. Cleft Palate Craniofac J 2018; 55 (03) 369-374
- 34 Fahradyan A, Tsuha M, Wolfswinkel EM, Mitchell KS, Hammoudeh JA, Magee III W. Optimal timing of secondary alveolar bone grafting: a literature review. J Oral Maxillofac Surg 2019; 77 (04) 843-849
- 35 Gomes OS, Carvalho RM, Faco R. et al. Influence of bone-anchored maxillary protraction on secondary alveolar bone graft status in unilateral complete cleft lip and palate. Am J Orthod Dentofacial Orthop 2020; 158 (05) 731-737
- 36 Rosenstein SW, Long Jr RE, Dado DV, Vinson B, Alder ME. Comparison of 2-D calculations from periapical and occlusal radiographs versus 3-D calculations from CAT scans in determining bone support for cleft-adjacent teeth following early alveolar bone grafts. Cleft Palate Craniofac J 1997; 34 (03) 199-205
- 37 Razi T, Niknami M, Ghazani FA. Relationship between Hounsfield unit in CT scan and gray scale in CBCT. J Dent Res Dent Clin Dent Prospect 2014; 8 (02) 107-110
Address for correspondence
Publication History
Article published online:
26 October 2022
© 2022. Association of Plastic Surgeons of India. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Dixon MJ, Marazita ML, Beaty TH, Murray JC. Cleft lip and palate: understanding genetic and environmental influences. Nat Rev Genet 2011; 12 (03) 167-178
- 2 Mossey PA, Little J, Munger RG, Dixon MJ, Shaw WC. Cleft lip and palate. Lancet 2009; 374 (9703): 1773-1785
- 3 Ma L, Hou Y, Liu G, Zhang T. Effectiveness of presurgical orthodontics in cleft lip and palate patients with alveolar bone grafting: a systematic review. J Stomatol Oral Maxillofac Surg 2021; 122 (01) 13-17
- 4 Chang C-S, Wallace CG, Hsiao Y-C. et al. Difference in the surgical outcome of unilateral cleft lip and palate patients with and without pre-alveolar bone graft orthodontic treatment. Sci Rep 2016; 6: 23597
- 5 Freitas JA, Garib DG, Oliveira M. et al. Rehabilitative treatment of cleft lip and palate: experience of the hospital for rehabilitation of craniofacial anomalies-USP (HRAC-USP)—part 2: pediatric dentistry and orthodontics. J Appl Oral Sci 2012; 20 (02) 268-281
- 6 Boyne PJ, Sands NR. Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg 1972; 30 (02) 87-92
- 7 Abyholm FE, Bergland O, Semb G. Secondary bone grafting of alveolar clefts. A surgical/orthodontic treatment enabling a non-prosthodontic rehabilitation in cleft lip and palate patients. Scand J Plast Reconstr Surg 1981; 15 (02) 127-140
- 8 Vandersluis YR, Fisher DM, Stevens K, Tompson BD, Lou W, Suri S. Comparison of dental outcomes in patients with nonsyndromic complete unilateral cleft lip and palate who receive secondary alveolar bone grafting before or after emergence of the permanent maxillary canine. Am J Orthod Dentofacial Orthop 2020; 157 (05) 668-679
- 9 Wirthlin JO. The orthodontist's role in the management of patients with cleft lip and palate undergoing alveolar bone grafting. Semin Orthod 2017; 23 (03) 268-278
- 10 Hynes PJ, Earley MJ. Assessment of secondary alveolar bone grafting using a modification of the Bergland grading system. Br J Plast Surg 2003; 56 (07) 630-636
- 11 Feichtinger M, Zemann W, Mossböck R, Kärcher H. Three-dimensional evaluation of secondary alveolar bone grafting using a 3D-navigation system based on computed tomography: a two-year follow-up. Br J Oral Maxillofac Surg 2008; 46 (04) 278-282
- 12 Hamada Y, Kondoh T, Noguchi K. et al. Application of limited cone beam computed tomography to clinical assessment of alveolar bone grafting: a preliminary report. Cleft Palate Craniofac J 2005; 42 (02) 128-137
- 13 Oberoi S, Chigurupati R, Gill P, Hoffman WY, Vargervik K. Volumetric assessment of secondary alveolar bone grafting using cone beam computed tomography. Cleft Palate Craniofac J 2009; 46 (05) 503-511
- 14 Dissaux C, Bodin F, Grollemund B. et al. Evaluation of success of alveolar cleft bone graft performed at 5 years versus 10 years of age. J Craniomaxillofac Surg 2016; 44 (01) 21-26
- 15 Parveen S, Husain A, Mascarenhas R, Reddy SG. Clinical utility of cone-beam computed tomography in patients with cleft lip palate: current perspectives and guidelines. J Cleft Lip Palate Craniofacial Anomalies 2018; 5 (02) 74-87
- 16 Spin-Neto R, Gotfredsen E, Wenzel A. Impact of voxel size variation on CBCT-based diagnostic outcome in dentistry: a systematic review. J Digit Imaging 2013; 26 (04) 813-820
- 17 Kamburoğlu K, Murat S, Kolsuz E, Kurt H, Yüksel S, Paksoy C. Comparative assessment of subjective image quality of cross-sectional cone-beam computed tomography scans. J Oral Sci 2011; 53 (04) 501-508
- 18 De Mulder D, Cadenas de Llano-Pérula M, Jacobs R, Verdonck A, Willems G. Three-dimensional radiological evaluation of secondary alveolar bone grafting in cleft lip and palate patients: a systematic review. Dentomaxillofac Radiol 2018; 48 (01) 20180047
- 19 Stasiak M, Wojtaszek-Słomińska A, Racka-Pilszak B. Current methods for secondary alveolar bone grafting assessment in cleft lip and palate patients—a systematic review. J Craniomaxillofac Surg 2019; 47 (04) 578-585
- 20 Yu X, Guo R, Li W. Comparison of 2- and 3-dimensional radiologic evaluation of secondary alveolar bone grafting of clefts: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol 2020; 130 (04) 455-463
- 21 Semb G, Brattström V, Mølsted K. et al. The Eurocleft study: intercenter study of treatment outcome in patients with complete cleft lip and palate. Part 4: relationship among treatment outcome, patient/parent satisfaction, and the burden of care. Cleft Palate Craniofac J 2005; 42 (01) 83-92
- 22 Zhang DZ, Xiao WL, Zhou R, Xue LF, Ma L. Evaluation of bone height and bone mineral density using cone beam computed tomography after secondary bone graft in alveolar cleft. J Craniofac Surg 2015; 26 (05) 1463-1466
- 23 Koç A, Kaya S. Is it possible to estimate volume of bone defects formed on dry sheep mandibles more practically by secondarily reconstructing section thickness of cone beam computed tomography images?. Dentomaxillofac Radiol 2021; 50 (03) 20200400
- 24 Barbosa GLR, Wood JS, Pimenta LA, de Almeida SM, Tyndall DA. Comparison of different methods to assess alveolar cleft defects in cone beam CT images. Dentomaxillofac Radiol 2016; 45 (02) 20150332
- 25 Pauwels R, Jacobs R, Singer SR, Mupparapu M. CBCT-based bone quality assessment: are Hounsfield units applicable?. Dentomaxillofac Radiol 2015; 44 (01) 20140238
- 26 Cassetta M, Stefanelli LV, Pacifici A, Pacifici L, Barbato E. How accurate is CBCT in measuring bone density? A comparative CBCT-CT in vitro study. Clin Implant Dent Relat Res 2014; 16 (04) 471-478
- 27 Witherow H, Cox S, Jones E, Carr R, Waterhouse N. A new scale to assess radiographic success of secondary alveolar bone grafts. Cleft Palate Craniofac J 2002; 39 (03) 255-260
- 28 Barbosa GLR, Emodi O, Pretti H. et al. GAND classification and volumetric assessment of unilateral cleft lip and palate malformations using cone beam computed tomography. Int J Oral Maxillofac Surg 2016; 45 (11) 1333-1340
- 29 Lever J, Krzywinski M, Altman N. Principal component analysis. Nat Methods 2017; 14 (07) 641-642
- 30 Kamperos G, Theologie-Lygidakis N, Tsiklakis K, Iatrou I. A novel success scale for evaluating alveolar cleft repair using cone-beam computed tomography. J Craniomaxillofac Surg 2020; 48 (04) 391-398
- 31 Tavakol M, Dennick R. Making sense of Cronbach's alpha. Int J Med Educ 2011; 2: 53-55
- 32 Semb G. Effect of alveolar bone grafting on maxillary growth in unilateral cleft lip and palate patients. Cleft Palate J 1988; 25 (03) 288-295
- 33 Garcia MA, Yatabe M, Fuzer TU, Calvo AM, Trindade-Suedam IK. Ideal versus late secondary alveolar bone graft surgery: a bone-thickness cone-beam computed tomographic assessment. Cleft Palate Craniofac J 2018; 55 (03) 369-374
- 34 Fahradyan A, Tsuha M, Wolfswinkel EM, Mitchell KS, Hammoudeh JA, Magee III W. Optimal timing of secondary alveolar bone grafting: a literature review. J Oral Maxillofac Surg 2019; 77 (04) 843-849
- 35 Gomes OS, Carvalho RM, Faco R. et al. Influence of bone-anchored maxillary protraction on secondary alveolar bone graft status in unilateral complete cleft lip and palate. Am J Orthod Dentofacial Orthop 2020; 158 (05) 731-737
- 36 Rosenstein SW, Long Jr RE, Dado DV, Vinson B, Alder ME. Comparison of 2-D calculations from periapical and occlusal radiographs versus 3-D calculations from CAT scans in determining bone support for cleft-adjacent teeth following early alveolar bone grafts. Cleft Palate Craniofac J 1997; 34 (03) 199-205
- 37 Razi T, Niknami M, Ghazani FA. Relationship between Hounsfield unit in CT scan and gray scale in CBCT. J Dent Res Dent Clin Dent Prospect 2014; 8 (02) 107-110