

Subscribe to RSS
DOI: 10.1055/s-0042-1750395
Atypical Presentation of Marginal Zone Lymphoma as Isolated Diffuse Bone Marrow Involvement: Utility of F-18 FDG PET/CT in Diagnosis and Response Assessment
Authors
Funding None.


Abstract
Non-Hodgkin's lymphoma (NHL) with secondary bone marrow involvement is relatively common. However, isolated involvement of bone marrow in marginal zone type of NHL is atypical and rare. Here, we describe a patient of atypical marginal zone lymphoma with isolated bone marrow involvement who presented with weight loss and bicytopenia, where F-18 FDG PET/CT (fluorine-18-labeled fluorodeoxyglucose positron emission tomography with computed tomography) imaging played a pivotal role in establishing the diagnosis when conventional imaging modalities were unremarkable. The patient was successfully treated with systemic chemotherapy (rituximab, cyclophosphamide, prednisolone) and achieved complete remission, as demonstrated by a follow-up F-18 FDG PET/CT scan.
Keywords
marginal zone lymphoma - F-18 FDG PET/CT - isolated bone marrow involvement - atypical presentation - case reportKey Messages
Isolated bone marrow involvement of indolent lymphomas should also be considered as differential diagnosis, if clinically correlated, when F-18 FDG PET/CT scan shows isolated diffuse bone marrow uptake.
In case of diffuse F-18 FDG uptake in bone marrow, heterogeneity in uptake pattern of F-18 FDG may assist in predicting lymphomatous involvement.
Introduction
Marginal zone lymphoma (MZL) is a low grade, third most common subtype of non-Hodgkin's lymphoma (NHL), and includes three entities: splenic MZL (SMZL), nodal MZL (NMZL), and extra-nodal MZL (EMZL) of mucosa-associated lymphoid tissue (MALT). The MALT type is more frequent among these subtypes. Bone marrow involvement occurs in 90% SMZL, 54% NMZL, and 22% EMZL.[1] However, isolated bone marrow involvement of MZL without lymph nodal and other extra-nodal involvement is very rare. We herein present a case of MZL with isolated bone marrow involvement, where fluorine-18-labeled fluorodeoxyglucose positron emission tomography with computed tomography (F-18 FDG PET/CT) helped in diagnosis when conventional imaging modalities were unremarkable. Such atypical presentation should be recognized for early diagnosis and adequate therapeutic strategies.
Case History
An 85-year-old male patient presented with complaints of weight loss of 7 kgs in 6 months. Routine blood investigations showed bicytopenia: WBC 5.65 K/uL, RBC 3.27 M/uL, platelet 63.0 K/uL, hemoglobin 8.6 g/dL, LDH 155.0 U/L (normal range: 0–248). Rest of the biochemical investigations, ultrasonography abdomen, and CT of thorax and abdomen were unremarkable. Since clinical history and biochemical and radiological tests did not yield any clue on possible underlying pathology, the patient was referred for F-18 FDG PET/CT imaging, to rule out occult malignancy/infection, which showed increased diffuse abnormal F-18 FDG uptake with subtle heterogeneity in the entire visualized skeleton (SUV Max 3.44) with no obvious CT-detected abnormality in the visualized bones ([Figs. 1] [2] [3] [4]).




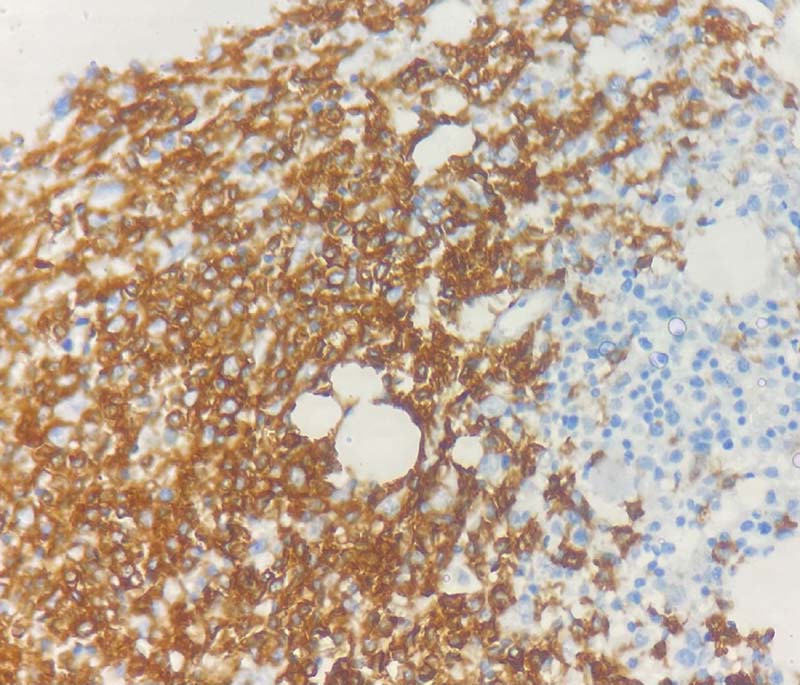
No significant FDG avid lymphadenopathy, splenic involvement, or any other extra-nodal sites of involvement were seen. A possibility of lymphoma with a differential diagnosis of multiple myeloma was entertained. The patient underwent posterior iliac crest bone marrow biopsy ([Figs. 5] [6] [7] [8]), which showed hypercellular marrow with 65% atypical lymphoid cells, predominantly positive for CD20 and negative for CD34, terminal deoxynucleotidyl transferase, and myeloperoxidase with scattered CD3-positive lymphocytes in the background. Flow cytometric immunophenotyping showed a population of CD19-positive B lymphocytes which expressed bright CD20, FMC7, and negative CD23. CD200, CD5, CD10, CD43, CD38, and lambda light chain were negative. Markers for hairy cell leukemia were negative. Chromosome analysis revealed an abnormal male chromosome complement with loss of Y chromosome as the sole anomaly in 60% of cells examined. Based on these results, the patient was diagnosed to have MZL with isolated bone marrow involvement. He was treated with six cycles of rituximab, cyclophosphamide, and prednisolone. Patient's clinical condition improved and he attained good biochemical response. End-of-treatment F-18 FDG PET/CT showed complete metabolic response.



Discussion
Bone marrow involvement is detected in approximately 5 to 14% of Hodgkin's lymphoma (HL) and 25 to 40% of high-grade NHL. However, isolated bone marrow involvement of indolent NHL is not common. We have described a case of MZL with isolated bone marrow involvement where F-18 FDG PET/CT was fundamental in diagnosing and assessing the treatment response.
Although the role of F-18 FDG PET/CT in staging and response assessment of HL and aggressive NHL is well established, it is of little clinical utility in the evaluation of indolent lymphoma like MZL. Considering the low F-18 FDG avidity of these indolent lymphomas, the Lugano classification has not supported the use of F-18 FDG PET scan for staging of MZL. CT has been considered as the whole-body imaging of choice for staging and response assessment in this indolent lymphoma subtype.[2] However, multiple studies have shown the utility of F-18 FDG PET/CT in MZL with a superior detection rate over conventional imaging.[3] [4] [5] [6] Despite the wide variability of F-18 FDG uptake in MZL, the overall F-18 FDG PET sensitivity was quite high with the pooled estimate value of detection rate being 71% (95% confidence interval: 61–80%), a similar trend to that registered in aggressive NHL.[7] Based on these studies, the classification of MZL under FDG nonavid lymphomas could be now reconsidered. The recent European Society for Medical Oncology guidelines have even proposed to consider F-18 FDG PET scanning in MALT lymphomas when localized treatment is planned, as well as in the case of suspicious transformation to high-grade histology to target lymph node for biopsy.[8]
Our case of atypical MZL with isolated diffuse bone marrow involvement showed fair F-18 FDG uptake, concurring with the above-mentioned data. The disease involvement in our case was not detected by the current recommended imaging modality of choice for MZL, i.e., CT thorax and abdomen. Thus, this case shows the utility of F-18 FDG PET/CT in MZL and its superiority over the morphological imaging in atypical presentation.
F-18 FDG PET/CT is being frequently used in detecting the lymphomatous bone marrow involvement. Focal F-18 FDG uptake in HL and aggressive NHL is sensitive for bone marrow involvement and may even obviate the need for biopsy.[9] However, diffuse F-18 FDG uptake is the controversial area where multiple studies have shown positive and negative bone marrow biopsy results.[10] Heterogeneity in F-18 FDG uptake pattern in these scenarios may assist in predicting the bone marrow involvement, like in our case, which also shows the role of F-18 FDG PET/CT in assessing response to therapy in atypical MZL.
In conclusion, we report a unique case of atypical MZL with isolated bone marrow involvement, successfully treated with systemic chemotherapy, in which F-18 FDG PET/CT played a pivotal role in diagnosis as well as response assessment. In cases with isolated diffuse F-18 FDG bone marrow uptake with heterogeneity, MZL may be included in one of the differential diagnoses, and it is important to establish the diagnosis quickly and initiate systemic chemotherapy.
Conflict of Interest
None declared.
-
References
- 1 Boveri E, Arcaini L, Merli M. et al. Bone marrow histology in marginal zone B-cell lymphomas: correlation with clinical parameters and flow cytometry in 120 patients. Ann Oncol 2009; 20 (01) 129-136
- 2 Cheson BD, Fisher RI, Barrington SF. et al; Alliance, Australasian Leukaemia and Lymphoma Group,, Eastern Cooperative Oncology Group,, European Mantle Cell Lymphoma Consortium,, Italian Lymphoma Foundation,, European Organisation for Research, Treatment of Cancer/Dutch Hemato-Oncology Group,, Grupo Español de Médula Ósea,, German High-Grade Lymphoma Study Group,, German Hodgkin's Study Group,, Japanese Lymphorra Study Group,, Lymphoma Study Association, NCIC Clinical Trials Group,, Nordic Lymphoma Study Group,, Southwest Oncology Group,, United Kingdom National Cancer Research Institute. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol 2014; 32 (27) 3059-3068
- 3 Albano D, Bertoli M, Ferro P. et al. 18F-FDG PET/CT in gastric MALT lymphoma: a bicentric experience. Eur J Nucl Med Mol Imaging 2017; 44 (04) 589-597
- 4 Albano D, Giubbini R, Bertagna F. 18F-FDG PET/CT in splenic marginal zone lymphoma. Abdom Radiol (NY) 2018; 43 (10) 2721-2727
- 5 Vaxman I, Bernstine H, Kleinstern G. et al. FDG PET/CT as a diagnostic and prognostic tool for the evaluation of marginal zone lymphoma. Hematol Oncol 2019; 37 (02) 168-175
- 6 Carrillo-Cruz E, Marín-Oyaga VA, de la Cruz Vicente F. et al. Role of 18F-FDG-PET/CT in the management of marginal zone B cell lymphoma. Hematol Oncol 2015; 33 (04) 151-158 Erratum in: Hematol Oncol. 2016;34(2):117
- 7 Treglia G, Zucca E, Sadeghi R, Cavalli F, Giovanella L, Ceriani L. Detection rate of fluorine-18-fluorodeoxyglucose positron emission tomography in patients with marginal zone lymphoma of MALT type: a meta-analysis. Hematol Oncol 2015; 33 (03) 113-124
- 8 Zucca E, Arcaini L, Buske C. et al; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Marginal zone lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2020; 31 (01) 17-29
- 9 Barrington SF, Mikhaeel NG, Kostakoglu L. et al. Role of imaging in the staging and response assessment of lymphoma: consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J Clin Oncol 2014; 32 (27) 3048-3058 Erratum in: J Clin Oncol. 2016;34(21):2562
- 10 Elamir Y, Elazab M, Owis A, Elsayad HF. PET/CT and bone marrow biopsy (BMB) in evaluating bone marrow in lymphoma. Egypt J Radiol Nucl Med 2020; 51: 201
Address for correspondence
Publication History
Article published online:
05 September 2022
© 2022. World Association of Radiopharmaceutical and Molecular Therapy (WARMTH). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Boveri E, Arcaini L, Merli M. et al. Bone marrow histology in marginal zone B-cell lymphomas: correlation with clinical parameters and flow cytometry in 120 patients. Ann Oncol 2009; 20 (01) 129-136
- 2 Cheson BD, Fisher RI, Barrington SF. et al; Alliance, Australasian Leukaemia and Lymphoma Group,, Eastern Cooperative Oncology Group,, European Mantle Cell Lymphoma Consortium,, Italian Lymphoma Foundation,, European Organisation for Research, Treatment of Cancer/Dutch Hemato-Oncology Group,, Grupo Español de Médula Ósea,, German High-Grade Lymphoma Study Group,, German Hodgkin's Study Group,, Japanese Lymphorra Study Group,, Lymphoma Study Association, NCIC Clinical Trials Group,, Nordic Lymphoma Study Group,, Southwest Oncology Group,, United Kingdom National Cancer Research Institute. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol 2014; 32 (27) 3059-3068
- 3 Albano D, Bertoli M, Ferro P. et al. 18F-FDG PET/CT in gastric MALT lymphoma: a bicentric experience. Eur J Nucl Med Mol Imaging 2017; 44 (04) 589-597
- 4 Albano D, Giubbini R, Bertagna F. 18F-FDG PET/CT in splenic marginal zone lymphoma. Abdom Radiol (NY) 2018; 43 (10) 2721-2727
- 5 Vaxman I, Bernstine H, Kleinstern G. et al. FDG PET/CT as a diagnostic and prognostic tool for the evaluation of marginal zone lymphoma. Hematol Oncol 2019; 37 (02) 168-175
- 6 Carrillo-Cruz E, Marín-Oyaga VA, de la Cruz Vicente F. et al. Role of 18F-FDG-PET/CT in the management of marginal zone B cell lymphoma. Hematol Oncol 2015; 33 (04) 151-158 Erratum in: Hematol Oncol. 2016;34(2):117
- 7 Treglia G, Zucca E, Sadeghi R, Cavalli F, Giovanella L, Ceriani L. Detection rate of fluorine-18-fluorodeoxyglucose positron emission tomography in patients with marginal zone lymphoma of MALT type: a meta-analysis. Hematol Oncol 2015; 33 (03) 113-124
- 8 Zucca E, Arcaini L, Buske C. et al; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Marginal zone lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2020; 31 (01) 17-29
- 9 Barrington SF, Mikhaeel NG, Kostakoglu L. et al. Role of imaging in the staging and response assessment of lymphoma: consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J Clin Oncol 2014; 32 (27) 3048-3058 Erratum in: J Clin Oncol. 2016;34(21):2562
- 10 Elamir Y, Elazab M, Owis A, Elsayad HF. PET/CT and bone marrow biopsy (BMB) in evaluating bone marrow in lymphoma. Egypt J Radiol Nucl Med 2020; 51: 201