

Subscribe to RSS
DOI: 10.1055/s-0041-1741050
Biopsy with Side-Cutting Coaxial Needle—Knowing the “Cutting Length” and “Throw Length”
Authors


Abstract
Image-guided Trucut biopsy is a well-established procedure. The length of the side notch in the stylet is the “cutting length,” which entraps the tissue sample and contributes to the yield. The total distance by which the inner stylet protrudes from the outer cannula with the cutting notch open is the “throw length.” It is inevitably longer than the cutting length does not add to the yield of the sample, but potentially to the complication of the procedure. The authors highlight the importance of knowing this distinction to minimize complications during the procedure.
Introduction
Image-guided percutaneous core needle biopsy is a well-established, minimally invasive method of sampling lesions and is an integral part of interventional radiology practice.[1] [2] Most of the time, it is done with automatic or semiautomatic biopsy devices called “biopsy gun.”[3] A coaxial technique involves the placement of a needle initially to the biopsy site and is wide enough to pass the actual biopsy needle through it for the required number of times.[3] [4] When performed with the correct technique, this procedure is relatively safe with diagnostic accuracy comparable to open surgical biopsy.[4]
As radiologists, it is not only essential to have sound knowledge about the characteristics of the target lesion but also about the biopsy instrument. Familiarity with the needle components helps in selecting the appropriate needle, practicing the correct technique, and planning the best approach for biopsy. This limits the likelihood of a nondiagnostic sample, improves efficiency, and helps avoid inadvertent complications.[4]
In this article, we discuss with illustrations how the needle traverses into the tissue of interest. We also address the potential factors in the outcome of a biopsy procedure with respect to needle penetration.
Points to Keep in Mind before Biopsy
Before attempting a biopsy, the radiologist should be well versed in the anatomical, patient-related, and technical aspects of the biopsy procedure.[4]
-
Anatomical factors: The location, depth from the skin surface, size, vascularity, morphology of the target lesion (site of maximum yield within the lesion), and vital structures in the biopsy path must be assessed based on prior imaging. These are vital to determining the optimal approach and patient position.[3]
-
Patient factors: This includes clinical history, laboratory workup, biopsy contraindications, informed consent, comfortable patient positioning, monitoring vitals, and breathing instructions.[4]
-
Technical factors: The diagnostic accuracy and procedure safety are connected not only to the lesions' features but also to the technical execution of the procedure.[5] Needle choice depends on the characteristics of the lesion (location and size), needle trajectory, amount of tissue required, experience, and operator preference.[3] [6] The measurements of different needle components are important in planning the safe access route, depth of deployment, and sampling technique.
Coaxial Needle System: How It Works?
We describe the working principle of the standard side-cutting coaxial needle with a fully automatic deployment system.
A coaxial needle system derives the name from the two needles, an outer guiding needle and an inner biopsy needle that share the same axis. It is usually obtained as a set. For example, it may be a combination of a 17G outer guiding needle that comes with its own stylet and an 18G biopsy needle. The commonly available lengths are 9 and 15 cm. The outer guiding needle tip is placed in the required region under image (computed tomography [CT] or ultrasonography [USG]) guidance at the edge of the targeted tissue until its tip is within firing distance of the target. Its stylet is removed and an 18G biopsy needle is passed through the guiding cannula. The diameter of the inner biopsy needle is such that it is just possible for it to be passed through the cannula. The biopsy needle tip matches to the tip of the cannula. The needle is attached to a spring-activated biopsy gun, which fires the needle into the targeted lesion. When the gun is fired, the cutting cannula of the biopsy needle rapidly moves over the stylet to cut the tissue and traps it into the notch of the stylet ([Fig. 1]).

During the biopsy shoot, the biopsy needle traverses beyond the tip of the outer coaxial needle along the longitudinal axis into the tissue sample to be obtained. The biopsy needle is removed and; the tissue sample is collected. This may be repeated a couple of times to collect the required amount of material. During USG-guided biopsy, the needle traversing may be seen as real-time guidance, which is not possible during CT-guided biopsy.
The coaxial technique allows the user to obtain multiple samples through a single puncture site while minimizing trauma to surrounding tissues.[7] [8]
Definitions of Biopsy Needle Geometry ([Fig. 2])

Cutting needles can be of side-cutting or end-cutting types. The side-cutting needle set consists of two parts[9]:
-
Inner stylet: It is fitted with a specimen notch for trapping the target tissue.
-
Cutting cannula: It moves over the sample notch of the stylet, cuts the tissue, and traps it into the notch. Its beveled edge is designed to prevent damage to the tissues surrounding the lesion.
Cutting Length
It is the length of side notch in the stylet, which entraps the tissue sample. The size of the tissue core obtained corresponds to dimensions of the side notch. Length of the side notch varies between devices, 20 mm being the most commonly used.[10]
Dead Space Length or Noncutting Tip
It is the part of the stylet (∼4–5 mm) that projects beyond the specimen notch and outer cannula and forms the tip of the needle. Its purpose is to block the sample in the notch and prevent its dislodgement inside the patient's body. If the target lesion is small in size, it can advance beyond the lesion and injure vital structures around the lesion margin.
Throw Length
It is the total penetration depth of the needle stylet, that is, the total distance by which the inner stylet protrudes from the cannula with the cutting notch open. It decides the guiding cannula's anchoring point so that the cutting length lies within the lesion and a representative sample can be obtained. It is the sum of cutting length and dead space length and measures ∼2.2 to 2.5 cm in standard needles.[11]
Trajectory Path of Needle System
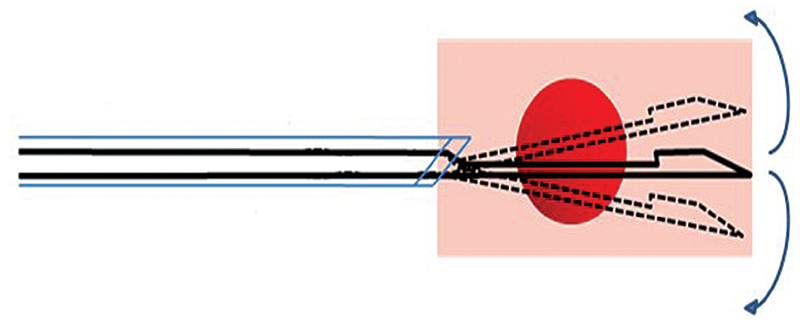
The word “trajectory” is used with respect to “fast-moving objects.” As per definition, it is the path followed by a projectile flying or an object moving under the action of given forces.[12] In the current context, it is the path traversed by the needle after the gun is fired. The trajectory may not strictly align along the expected path of the needle but may deviate if it gets bent/angulated or encounters resistance in its path. The biopsy needle path would be within a small diameter cone-shaped potential zone, from where the tissue sample can be obtained, after the outer guiding cannula of a coaxial system is parked at the lesion edge. It also determines the area vulnerable to injury if the penetration length is overshot ([Figs. 3] and [4]).

Challenges with the Needle Throw Length
The device's throw length and trajectory path cannot be predicted with absolute precision. This is a limitation of a coaxial biopsy needle system.
During the firing of the biopsy gun, the throw length can unexpectedly deflect from its presumed trajectory. This can cause tissue undersampling or damage to delicate structures located in the needle's altered trajectory.[10]
Firing of the gun induces a shock wave that travels both longitudinally and sideways along the needle track. The traumatic nature of the shock wave further adds to damage to normal tissues.[13]
We enlist the following challenges in controlling the needle trajectory:
-
If the lesion is large enough, the needle's throw length may safely lie within the lesion. However, when the lesion is small in size, the dead space length may protrude outside the target to accommodate the specimen notch in the optimal position.[9] This puts deeper structures such as vessels, nerves, interlobar fissures, or lung bullae at risk of injury ([Fig. 5]).[11] For example, if the needle edge hits the pulmonary vessels located deep to the lesion, it can lead to pulmonary hemorrhage and hemoptysis ([Fig. 6]). If the needle tip hits the pleura or fissure along the needle's trajectory, it can lead to pneumothorax, even without the cutting-edge crossing the fissure ([Fig. 7]).
-
While loading the gun, the stylet extends beyond the outer supportive cannula. The sample notch of the stylet is thin and relatively flexible and may bend when encountering dense tissues. This can introduce an unpredictable change in the trajectory path of the needle, changing the original site of sampling or making adjacent tissues vulnerable to damage.
-
Post deployment, the needle tip is manually tilted by small angles to get multiple samples from different areas of the lesion. This creates a larger trajectory path of the needle and exposes a larger volume of tissues to injury.
-
If the length of the selected needle is disproportionately longer than the size/depth of the lesion, the extra undesirable length will lie outside the patient's body and compromise the stability and control over the needle tip. During sampling, this introduces a risk of needle overpenetration. The additional forward trajectory path increases the depth of tissue traumatized by the throw length.
-
After the outer guiding cannula is positioned and stabilized by the fingers, multiple passes of the biopsy needle are made through it. Each time the needle is introduced inside, the cannula can get displaced from its original location and can move to a more superficial/deeper location by at least a few millimeters. This exposes different areas in the linear trajectory path to injury.
-
The needle trajectory may change if it encounters resistance in its path, usually due to inherently dense/fibrous lesions or hard structures in the lesion's vicinity. A common example is when the needle tip hits a bony structure ahead of the lesion, causing backward recoil of the needle. The cutting length can then lie well outside the lesion, leading to collection of nonrepresentative samples ([Fig. 8]).
-
Various movements like patient movement and respiratory motion and complications such as pneumothorax can unknowingly shift the needle from its original location and change the trajectory path, leading to sampling errors ([Fig. 9]).[4]





Modification of the Biopsy Technique: Adjustment for Needle Throw Length
We describe the following methods of avoiding or overcoming the above-mentioned shortcomings of unpredictability in needle trajectory:
-
While planning the biopsy, we must ensure that the sensitive structures, such as large vessels, are not in the device's potential deployment path or in the danger space ahead of the lesion. This can be partly achieved by selecting an appropriate patient position or entry route for the biopsy.
-
In situations of small lesion size or unfavorable anatomy, the guiding cannula should be withdrawn and parked proximal to the lesion, so that the cutting length of the stylet can course through the lesion ([Figs. 10] and [11]). This safe distance is calculated between the cannula's anticipated tip and the distal edge of the lesion and corresponds to the “throw length” of the needle. Maintaining a safe firing distance minimizes damage to structures located close to the deep aspect of the lesion, without sacrificing the diagnostic yield.[11]
-
If the size of the lesion is smaller than the size of the cutting length, the biopsy needle tip can be kept slightly within the outer guiding coaxial needle while firing.
-
Even when the guiding cannula is parked at a favorable location, during the sampling process, the stylet and its cutting notch should be angulated and directed away from the vital structures. However, tilting the needle by larger degrees is also unfavorable.
-
The safe distance should be calculated before the start of the procedure so that the appropriate needle length can be selected. The length should be slightly longer than the depth of the lesion from the skin surface. This will give better control over the needle and prevent its overpenetration.
-
Extreme care should be taken not to inadvertently advance or withdraw the guiding cannula, especially during multiple insertions of the biopsy gun through it. The use of a needle guard provides better control of needle progression and enables graded insertion without needle displacement.
-
The needle should be advanced in a stepwise manner from the skin to the lesion and the latest acquired scan should be monitored. Corrective manipulation should be done if there is a change in the trajectory of the needle.[4] The cutting notch should be documented to be within the lesion before firing the gun, increasing the confidence of getting a positive sample yield.[10]
-
One should be aware of large pulsating structures like cardiac chambers and aorta while placing needles into an area close to these, especially under CT guidance.
-
A check CT can be performed if the tip was in the correct position, but there is no yield. This can check the inadvertent movement of the tip of the outer needle or a complication like pneumothorax or local hemorrhage.


Conclusion
The diagnostic accuracy and procedure safety depend upon the lesion's characteristics and the technical execution of the procedure. Knowledge of the structures in the vicinity of the lesion and components of the core-biopsy needle such as the “throw length” helps predict the trajectory path, needle anchoring position, and safe firing distance. These modifications to the biopsy approach, based on needle specifications, help in improvising the yield and minimizing the complications.
Conflicts of Interest
There are no conflicts of interest.
Financial Support and Sponsorship
Nil.
-
References
- 1 Hatfield MK, Beres RA, Sane SS, Zaleski GX. Percutaneous imaging-guided solid organ core needle biopsy: coaxial versus noncoaxial method. AJR Am J Roentgenol 2008; 190 (02) 413-417
- 2 Geraghty PR, Kee ST, McFarlane G, Razavi MK, Sze DY, Dake MD. CT-guided transthoracic needle aspiration biopsy of pulmonary nodules: needle size and pneumothorax rate. Radiology 2003; 229 (02) 475-481
- 3 Gupta S, Madoff DC. Image-guided percutaneous needle biopsy in cancer diagnosis and staging. Tech Vasc Interv Radiol 2007; 10 (02) 88-101
- 4 Lal H, Neyaz Z, Nath A, Borah S. CT-guided percutaneous biopsy of intrathoracic lesions. Korean J Radiol 2012; 13 (02) 210-226
- 5 Wu CC, Maher MM, Shepard J-AO. CT-guided percutaneous needle biopsy of the chest: preprocedural evaluation and technique. AJR Am J Roentgenol 2011; 196 (05) W511-4
- 6 Winokur RS, Pua BB, Sullivan BW, Madoff DC. Percutaneous lung biopsy: technique, efficacy, and complications. Semin Intervent Radiol 2013; 30 (02) 121-127
- 7 Hopper KD, Abendroth CS, TenHave TR, Hartzel J, Savage CA. Multiple fine-needle biopsies using a coaxial technique: efficacy and a comparison of three methods. Cardiovasc Intervent Radiol 1995; 18 (05) 307-311
- 8 Schässburger K-U, Paepke S, Saracco A, Azavedo E, Ekström C, Wiksell H. High velocity pulse biopsy device enables controllable and precise needle insertion and high yield tissue acquisition. Phys Med 2018; 46: 25-31
- 9 Yuen HY, Lee Y, Bhatia K, Wong KT, Ahuja AT. Use of end-cutting needles in ultrasound-guided biopsy of neck lesions. Eur Radiol 2012; 22 (04) 832-836
- 10 Birchard KR. Transthoracic needle biopsy. Semin Intervent Radiol 2011; 28 (01) 87-97
- 11 Coucher JR, Connor P. Percutaneous coaxial needle biopsy using the spacer technique: a novel and easy modification to increase procedure safety. Clin Radiol 2005; 60 (08) 926-929
- 12 Projectile motion - Wikipedia [Internet]. Accessed November 20, 2021 from: https://en.wikipedia.org/wiki/Projectile_motion
- 13 Tsai I-C, Tsai W-L, Chen M-C. et al. CT-guided core biopsy of lung lesions: a primer. AJR Am J Roentgenol 2009; 193 (05) 1228-1235
Address for correspondence
Publication History
Article published online:
10 January 2022
© 2022. Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Hatfield MK, Beres RA, Sane SS, Zaleski GX. Percutaneous imaging-guided solid organ core needle biopsy: coaxial versus noncoaxial method. AJR Am J Roentgenol 2008; 190 (02) 413-417
- 2 Geraghty PR, Kee ST, McFarlane G, Razavi MK, Sze DY, Dake MD. CT-guided transthoracic needle aspiration biopsy of pulmonary nodules: needle size and pneumothorax rate. Radiology 2003; 229 (02) 475-481
- 3 Gupta S, Madoff DC. Image-guided percutaneous needle biopsy in cancer diagnosis and staging. Tech Vasc Interv Radiol 2007; 10 (02) 88-101
- 4 Lal H, Neyaz Z, Nath A, Borah S. CT-guided percutaneous biopsy of intrathoracic lesions. Korean J Radiol 2012; 13 (02) 210-226
- 5 Wu CC, Maher MM, Shepard J-AO. CT-guided percutaneous needle biopsy of the chest: preprocedural evaluation and technique. AJR Am J Roentgenol 2011; 196 (05) W511-4
- 6 Winokur RS, Pua BB, Sullivan BW, Madoff DC. Percutaneous lung biopsy: technique, efficacy, and complications. Semin Intervent Radiol 2013; 30 (02) 121-127
- 7 Hopper KD, Abendroth CS, TenHave TR, Hartzel J, Savage CA. Multiple fine-needle biopsies using a coaxial technique: efficacy and a comparison of three methods. Cardiovasc Intervent Radiol 1995; 18 (05) 307-311
- 8 Schässburger K-U, Paepke S, Saracco A, Azavedo E, Ekström C, Wiksell H. High velocity pulse biopsy device enables controllable and precise needle insertion and high yield tissue acquisition. Phys Med 2018; 46: 25-31
- 9 Yuen HY, Lee Y, Bhatia K, Wong KT, Ahuja AT. Use of end-cutting needles in ultrasound-guided biopsy of neck lesions. Eur Radiol 2012; 22 (04) 832-836
- 10 Birchard KR. Transthoracic needle biopsy. Semin Intervent Radiol 2011; 28 (01) 87-97
- 11 Coucher JR, Connor P. Percutaneous coaxial needle biopsy using the spacer technique: a novel and easy modification to increase procedure safety. Clin Radiol 2005; 60 (08) 926-929
- 12 Projectile motion - Wikipedia [Internet]. Accessed November 20, 2021 from: https://en.wikipedia.org/wiki/Projectile_motion
- 13 Tsai I-C, Tsai W-L, Chen M-C. et al. CT-guided core biopsy of lung lesions: a primer. AJR Am J Roentgenol 2009; 193 (05) 1228-1235