
Subscribe to RSS
DOI: 10.1055/s-0040-1716765
Long Term Outcomes of Computer-Navigated Lateral Opening Wedge Distal Femoral Osteotomy for Lateral Compartment Knee Arthrosis[*]
Article in several languages: português | English
- Abstract
- Introduction
- Methods
- Surgical Technique
- Outcome Measures and Statistics
- Results
- Discussion
- Conclusions
- Referências
Abstract
Objective The primary aim of the present study was to evaluate the long-term outcomes including survivorship of computer navigated distal femoral lateral opening wedge osteotomy (DFLOWO). The secondary aim was to identify the potential factors that may influence its survivorship.
Methods A retrospective analysis of prospectively collected data for patients with lateral compartment arthritis who underwent navigated DFLOWO from December 2006 to November 2012 was performed. The International Knee Documentation Committee (IKDC) and Knee Injury and Osteoarthritis Outcome Score (KOOS) scores were analyzed for outcome measures. Conversion to arthroplasty during the follow-up was the end point.
Results A total of 19 DFLOWOs were performed in 17 patients with a mean age of 46.6 ± 6.5 years formed the study cohort. The coronal alignment was corrected from a mean of 7.1° (2–11°) valgus to a mean of 2.1° (0.5°–3°) varus. The IKDC scores improved from mean of 39 preoperatively to 53 at the mean long-term follow-up of 9.1 years. The mean KOOS scores at the long-term follow-up were pain 71, symptoms 56, activities of daily living 82, sports and recreation 59, quality of life 43. Survivorship of the DFLOWO was 78.9% at a follow-up of 9.1 years. Presence of ≥ grade 2 according to the International Cartilage Repair Society (ICRS) cartilage degeneration in the medial compartment of the knee and >7° preoperative valgus deformity were strongly correlated with conversion to total knee arthroplasty (TKA) at the long-term follow-up (r = 0.66).
Conclusions Computer navigated DFLOWO has satisfactory clinical outcomes and 79% survivorship in long-term follow-up. Presence of more than ICRS ≥ grade 2 degenerative changes in the medial compartment of knee with > 7° preoperative valgus deformity negatively affects the survivorship of DFLOWO in the long-term follow-up.
#
Introduction
Osteotomy of the distal femur (DFO) to address symptomatic degeneration in the knee is a well-established procedure[1] with good results reported in the literature.[2] Broadly, the osteotomy is based on either an opening[3] [4] [5] [6] or a closing[7] [8] [9] [10] [11] [12] wedge alignment technique. Several patient-related parameters including age, gender, body mass index (BMI) and surgical factors such as osteotomy site, gap, and fixation technique, amongst others, have been demonstrated to influence the outcome of DFO. Preoperative planning based on imaging is vital to assess the type and extent of deformity correction to be undertaken to achieve optimal alignment.[13] [14] Computer-assisted surgery (CAS) has been extensively used as a dynamic intraoperative alignment aid in knee arthroplasty, providing good outcomes.[15] Several investigators in the current literature have utilized computer navigation in proximal tibial osteotomy and reported improved accuracy in realizing the planned alignment.[16] [17] [18] However, there is paucity of studies reporting the long-term outcomes of distal femur lateral opening-wedge (DFLOWO) using computer navigation. Through our study, we aim to report on the long-term outcomes and survivorship of computer navigated DFLOWO.
#
Methods
Ethics committee approval was obtained for the present study. Due consent was taken for the use of data from all the patients of the present study. A retrospective analysis of prospectively collected data for patients with lateral compartment arthritis who underwent navigated lateral opening wedge distal femoral osteotomy from December 2006 to November 2012 was performed. Consecutive patients of lateral compartment knee arthrosis aged < 55 years old who failed to respond to conservative management were included in the study. Patients who had end stage arthritis with fixed flexion deformity of > 15°, < 90° of knee flexion or who did not consent with the procedure were excluded.
The included patients were operated by one of the three senior surgeons attached to our research institute. The included patients were followed-up with clinical and radiological evaluation at regular intervals (6 weeks / 6 months / 1 year / 5 years). The final follow-up for the included patients was done using an email questionnaire of the patient-reported outcomes measures. Conversion to either unicompartmental knee arthroplasty (UKA) or total knee arthroplasty (TKA) during the follow-up was the end point. Additionally, this information was verified from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) database.[19]
#
Surgical Technique
The surgery was performed in the supine position.The preparation was made, as well as free sterile draping of the lower limb. Femoral and tibial trackers were inserted to register the landmarks for measuring the limb alignment using navigation. The three surgeons used two different navigation systems, including ORTHOSoft (Zimmer, Warsaw, IN, USA) and OrthoMap Precision Knee Navigation (Stryker, Kalamazoo, MI, USA). First, the center of the femoral head was registered. Subsequently, diagnostic arthroscopy was performed, and any arthroscopically treatable intra-articular causes of knee pain were addressed. The International Cartilage Repair Society (ICRS) grade of the knee articular cartilage was documented for the medial compartment, the lateral compartment, the patella and the trochlea. Registration of remaining landmarks was then completed including the center of the distal femur and the proximal tibia as well as the femoral condyle and tibial plateau and the malleoli.
A lateral skin incision of between 12 and 15 cm was made from the level of the lateral knee joint line proximally. The fascia lata was incised immediately posterior to the iliotibial band and the vastus lateralis was exposed and elevated anteriorly off the lateral intermuscular septum. Subperiosteal posterior femoral soft tissue dissection was performed to separate the posterior neurovascular structures from the posterior femoral surface. Protective soft tissue retractors were used to protect the neurovascular structures and the anterior extensor mechanism. Utilizing fluoroscopic guidance, a guidewire was passed from the middle of the lateral femoral surface just proximal to the superior pole of the patella and slightly oblique to the axial plane, aiming slightly distally toward the adductor tubercle. Utilizing fluoroscopy and a sagittal saw, the osteotomy was commenced through the metaphyseal bone from lateral to medial immediately proximal to the guidewire. While the saw was utilized for osteotomy of the lateral and anterior femur, a sharp osteotome was used to perform osteotomy of the posterior cortex. The medial hinge of the intact bone was preserved by carefully advancing the saw and the osteotome up to but not beyond the line corresponding to the lateral face of the medial femoral condyle. After osteotomy, the alignment was corrected to a neutral mechanical axis under the guidance of navigation, using a laminar spreader to create a controlled gap at the osteotomy site with care to not alter the femur in the sagittal plane. Once adequate correction was achieved, the wedge-shaped bone void was filled with allograft and the osteotomy was stabilized with a plate fixation.
Postoperatively, the limb was held in full extension in a limited range of motion brace, which was opened to allow a range of 0 to 30° on the first postoperative day. Part weight bearing mobilization was allowed with support – initially one quarter of the body weight as tolerated by the patient and increasing by one quarter of the body weight every 2 weeks. At 2 weeks, the brace was opened to allow a range of 0 to 90° and gradual flexion was allowed with supervision by a physiotherapist until the 6-week mark, when the brace was discontinued. Use of crutches is continued as needed and after 6 weeks physiotherapy regime was upgraded from range of motion to strengthening exercise program. this was continued till the patient was able to full weight bear and walk with support.
#
Outcome Measures and Statistics
International Knee Documentation Committee (IKDC)[20] and Knee Injury and Osteoarthritis Outcome Score (KOOS)[21] were prospectively collected. The IKDC score was obtained preoperatively and at 1 year and then at the long-term follow-up (> 6 years), and the KOOS scores were recorded at the long-term follow-up (> 6 years). The collected data was recorded on a Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) spreadsheet and analyzed using IBM SPSS Statistics for Windows Version 24 (IBM Corp., Armonk, NY, USA). Descriptive statistics including mean, standard deviation (SD) and range were quantified for all recorded data. The Student t-test and analysis of variance (ANOVA) were used to compare the means of 2 or > 2 independent groups, respectively. Linear and multiple regression analyses were used to identify the factors correlating with conversion to TKA.
#
Results
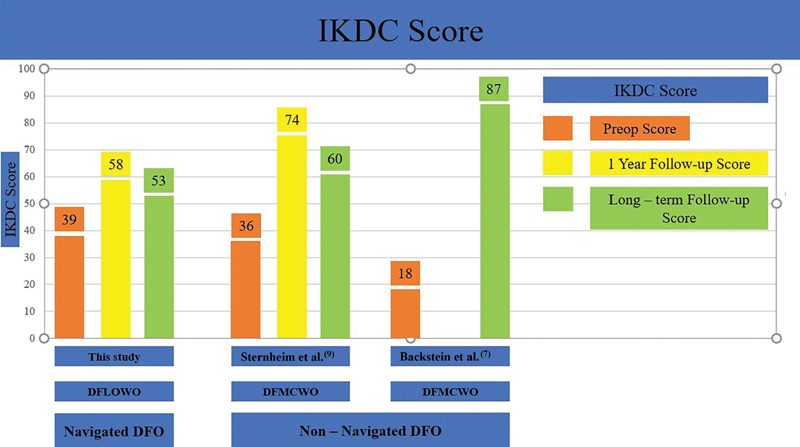
A total of 19 DFLOWOs were performed in 17 patients including 11 males and 6 females. The mean age was 46.6 ± 6.5 (33–53) years. A total of 15 of the 19 DFLOWOs (78.9%) had a previous history of partial lateral meniscectomy. The coronal alignment was corrected from a mean of 7.1° (2–11°) valgus to a mean 2.1° (0.5° - 3°) varus. The sagittal alignment was corrected from a mean of 7.5° (0–11°) of flexion contracture to a mean of 1° (0–3°) of flexion contracture. A total of 4 out of 19 DFLOWOs were converted to TKA. Thus, the survivorship of navigated DFLOWO in our study cohort was 78.9% at a mean follow-up of 9.1 years ([Fig. 1]). The IKDC scores improved from a mean of 39 in the preoperative period to 58 at the 1-year follow-up and deteriorated to 53 at the mean long-term follow-up of 9.1 years ([Fig. 2]). The KOOS scores at the long-term follow-up were: pain 71, symptoms 56, activities of daily living 82, sports and recreation 59, quality of life 43 ([Fig. 3]). The knee range of motion for the cohort ranged from a mean of 3° of flexion contracture to 124° of maximum flexion. The degree of preoperative valgus deformity negatively correlated with survivorship (Pearson’s correlation coefficient [PCC]: - 0.49; p = 0.03). Also, presence of ≥ grade 2 ICRS cartilage damage in the medial compartment of the knee with higher preoperative valgus deformity (> 7°) was strongly correlated with conversion to TKA at the long-term follow-up [r = 0.66; p = 0.002] ([Table 1]).


|
Factors |
PCC |
p-value |
|---|---|---|
|
Gender |
−0.13 |
0.61 |
|
Age |
0.28 |
0.25 |
|
Preoperative valgus |
−0.49 |
0.03* |
|
Degree of correction |
−0.33 |
0.17 |
|
ICRS Grade cartilage damage |
||
|
• Medial compartment of knee |
−0.28 |
0.25 |
|
• Lateral compartment of knee |
0.05 |
0.84 |
|
• Patellofemoral compartment of knee |
−0.12 |
0.62 |
|
Previous lateral meniscectomy |
−0.18 |
0.47 |
|
>7° preoperative valgus and ≥ grade 2 ICRS in Medical compartment of knee |
−0.66 |
0.002* |
Apart from conversion to TKA, 12 additional surgical interventions were performed in the study cohort during the follow-up period. These included: i) hardware removal (9), ii) bone graft and stabilization (2) for nonunion and iii) revision fixation (1) for peri-implant fracture secondary to a fall at 6 months after the primary surgery, which progressed to satisfactory union following intervention. One patient suffered from deep venous thrombosis after the procedure and was adequately treated without any long-term consequences.
#
Discussion
There has been a resurgence of interest in DFO to manage lateral compartment knee arthritis especially in the young and active population group. This interest has stemmed from the improvisation in surgical techniques and the availability of better fixation implants. A major technical advancement has been the use of computer navigation to achieve accurate correction. Although DFLOWO has recently gained popularity over the conventional distal femoral medial closing wedge osteotomy (DFMCWO),[1] [2] there is paucity of studies in the current literature reporting the long-term outcomes and survivorship following DFLOWO.[2]
Our study is the first to report the long-term survivorship of 78.9% at 9.1 years of follow-up for computer-navigated DFLOWO. The only other study which reports on the clinical outcomes of computer navigated DFO is by Saragaglia et al.[22] It included patients who have undergone either a DFLOWO or DFMCWO and reported the clinical outcomes at a mean medium-term follow-up of 50.9 months. At the last follow-up, none of the included patients were converted to TKA. A recently published study by Shivji et al.[23] described the clinical outcomes of large cohort patients from a single center who underwent either DFMCWO or DFLOWO. The patients included in their cohort underwent DFO after modern digital planning with use of precise surgical instruments to achieve accurate correction and stabilization with precontoured locking plate fixation. They reported an overall survival of 89% at 10 years. The long-term survival of osteotomy in our study is inferior to the one described by Shivji et al.[23] Including patients of only DFLOWO and not a mixed cohort of DFLOWO and DLMCWO could explain this difference. Also, when we compare the published survival rates of DFOs with this study, it is evident that the long-term survival of computer-navigated DFLOWO is better than the survival of non-navigated DFLOWO, but inferior to survivorship of non-navigated DFMCWO ([Fig. 1]).
Use of knee arthroscopy at the time of performing navigated DFO facilitated knowledge of accurate status of articular cartilage damage. Patients who had ≥ grade 2 ICRS cartilage damage in the medial compartment of the knee and had > 7° of preoperative valgus were more likely to be converted to TKA (r = 0.66). This important information can aid in preoperative decision-making and postoperative patient counselling. Assessment of articular cartilage status based on radiographs can underestimate the cartilage damage. Thus, efforts should be made to gain information about the status of the knee cartilage from old patient records, if patients had undergone previous knee arthroscopy. Young patients with lateral compartment knee arthrosis with ≥ grade 2 ICRS cartilage damage in the medial compartment of knee and > 7° of valgus limb alignment should be duly informed about the high chances of DFLOWO failing and of the need of a second surgery for conversion to TKA in the long-term follow-up.
The long-term KOOS scores of patients who underwent DFLOWO in our study were similar to those reported by Ekeland et al.[1] in their series of patients who underwent non-navigated DFLOWO ([Fig. 3]). When compared with the published long-term IKDC scores of patients who underwent non-navigated DFMCWO, the results were mixed ([Fig. 2]). Long-term IKDC scores of navigated DFLOWO patients in our series were either similar or marginally inferior to those of non-navigated DFMCWO; but no direct comparison and conclusions could be drawn as these studies were heterogeneous.
Our study had certain limitations. Although our study was done using the data of patients belonging to one institute, the included patients belonged to three different surgeons who made use of two different navigation systems. Although all the surgeons were fellowship trained knee surgeons and made use of similar surgical techniques, there were differences in the type of fixation and bone graft used. Also, the total number of DFLOWOs included in the study was small when compared with some other published series.
#
Conclusions
Computer-navigated DFLOWO has satisfactory clinical outcomes and 79% survivorship in long-term follow-up. Presence of ICRS ≥ grade 2 degenerative changes in the medial compartment of the knee with > 7° preoperative valgus deformity negatively affects the survivorship of DFLOWO in the long-term follow-up.
#
#
Authors' contributions
All the authors contributed to the formulation of the idea and study protocol, data collection, statistical analyses, analyses of the results and writing of the manuscript.
Abbreviations
Osteotomy of distal femur (DFO), distal femur lateral opening-wedge osteotomy (DFLOWO), distal femur medial closing wedge osteotomy (DFMCWO), body mass index (BMI), International Knee Documentation Committee (IKDC), Knee Injury and Osteoarthritis Outcome Score (KOOS), Total knee arthroplasty (TKA), Uni-compartmental knee arthroplasty (UKA), International Cartilage Repair Society (ICRS), Computer assisted surgery (CAS).
* Work developed at Orthopaedic Knee surgery, Sydney Orthopaedic Research Institute, Chatswood, Sydney, NSW, Australia.
-
Referências
- 1 Ekeland A, Nerhus TK, Dimmen S, Heir S. Good functional results of distal femoral opening-wedge osteotomy of knees with lateral osteoarthritis. Knee Surg Sports Traumatol Arthrosc 2016; 24 (05) 1702-1709
- 2 Chahla J, Mitchell JJ, Liechti DJ. et al. Opening-and closing-wedge distal femoral osteotomy: a systematic review of outcomes for isolated lateral compartment osteoarthritis. Orthop J Sports Med 2016; 4 (06) 2325967116649901
- 3 Dewilde TR, Dauw J, Vandenneucker H, Bellemans J. Opening wedge distal femoral varus osteotomy using the Puddu plate and calcium phosphate bone cement. Knee Surg Sports Traumatol Arthrosc 2013; 21 (01) 249-254
- 4 Jacobi M, Wahl P, Bouaicha S, Jakob RP, Gautier E. Distal femoral varus osteotomy: problems associated with the lateral open-wedge technique. Arch Orthop Trauma Surg 2011; 131 (06) 725-728
- 5 Thein R, Bronak S, Thein R, Haviv B. Distal femoral osteotomy for valgus arthritic knees. J Orthop Sci 2012; 17 (06) 745-749
- 6 Zarrouk A, Bouzidi R, Karray B, Kammoun S, Mourali S, Kooli M. Distal femoral varus osteotomy outcome: Is associated femoropatellar osteoarthritis consequential?. Orthop Traumatol Surg Res 2010; 96 (06) 632-636
- 7 Backstein D, Morag G, Hanna S, Safir O, Gross A. Long-term follow-up of distal femoral varus osteotomy of the knee. J Arthroplasty 2007; 22 (04, Suppl 1): 2-6
- 8 Finkelstein JA, Gross AE, Davis A. Varus osteotomy of the distal part of the femur. A survivorship analysis. J Bone Joint Surg Am 1996; 78 (09) 1348-1352
- 9 Sternheim A, Garbedian S, Backstein D. Distal femoral varus osteotomy: unloading the lateral compartment: long-term follow-up of 45 medial closing wedge osteotomies. Orthopedics 2011; 34 (09) e488-e490
- 10 Kosashvili Y, Safir O, Gross A, Morag G, Lakstein D, Backstein D. Distal femoral varus osteotomy for lateral osteoarthritis of the knee: a minimum ten-year follow-up. Int Orthop 2010; 34 (02) 249-254
- 11 Forkel P, Achtnich A, Metzlaff S, Zantop T, Petersen W. Midterm results following medial closed wedge distal femoral osteotomy stabilized with a locking internal fixation device. Knee Surg Sports Traumatol Arthrosc 2015; 23 (07) 2061-2067
- 12 Wang JW, Hsu CC. Distal femoral varus osteotomy for osteoarthritis of the knee. J Bone Joint Surg Am 2005; 87 (01) 127-133
- 13 Paccola CAJ. Pre-operative planning and surgical technique of the open wedge supracondylar osteotomy for correction of valgus knee and fixation with a fixed-angle implant. Rev Bras Ortop 2015; 45 (06) 627-635
- 14 Elattar O, Swarup I, Lam A, Nguyen J, Fragomen A, Rozbruch SR. Open wedge distal femoral osteotomy: accuracy of correction and patient outcomes. HSS J 2017; 13 (02) 128-135
- 15 Lee SH, Song EK, Seon JK. Navigation system provides better functional outcomes of total knee arthroplasty. Form J Musculoskel Dis 2016; 7 (01) 8-16
- 16 Reising K, Strohm PC, Hauschild O. et al. Computer-assisted navigation for the intraoperative assessment of lower limb alignment in high tibial osteotomy can avoid outliers compared with the conventional technique. Knee Surg Sports Traumatol Arthrosc 2013; 21 (01) 181-188
- 17 Akamatsu Y, Mitsugi N, Mochida Y. et al. Navigated opening wedge high tibial osteotomy improves intraoperative correction angle compared with conventional method. Knee Surg Sports Traumatol Arthrosc 2012; 20 (03) 586-593
- 18 Ribeiro CH, Severino NR, Moraes de Barros Fucs PM. Opening wedge high tibial osteotomy: navigation system compared to the conventional technique in a controlled clinical study. Int Orthop 2014; 38 (08) 1627-1631
- 19 The Australian Orthopaedic Association National Joint Replacement Registry. Ad Hoc Report. Adelaide, Australia: AOA; 2019
- 20 Irrgang JJ, Anderson AF, Boland AL. et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 2001; 29 (05) 600-613
- 21 Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)–development of a self-administered outcome measure. J Orthop Sports Phys Ther 1998; 28 (02) 88-96
- 22 Saragaglia D, Chedal-Bornu B. Computer-assisted osteotomy for valgus knees: medium-term results of 29 cases. Orthop Traumatol Surg Res 2014; 100 (05) 527-530
- 23 Shivji FS, Foster A, Risebury MJ, Wilson AJ, Yasen SK. Ten-year survival rate of 89% after distal femoral osteotomy surgery for lateral compartment osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc 2020; DOI: 10.1007/s00167-020-05988-5.
Endereço para correspondência
Publication History
Received: 17 May 2020
Accepted: 06 July 2020
Article published online:
30 September 2020
© 2020. Sociedade Brasileira de Ortopedia e Traumatologia. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Revinter Publicações Ltda.
Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
-
Referências
- 1 Ekeland A, Nerhus TK, Dimmen S, Heir S. Good functional results of distal femoral opening-wedge osteotomy of knees with lateral osteoarthritis. Knee Surg Sports Traumatol Arthrosc 2016; 24 (05) 1702-1709
- 2 Chahla J, Mitchell JJ, Liechti DJ. et al. Opening-and closing-wedge distal femoral osteotomy: a systematic review of outcomes for isolated lateral compartment osteoarthritis. Orthop J Sports Med 2016; 4 (06) 2325967116649901
- 3 Dewilde TR, Dauw J, Vandenneucker H, Bellemans J. Opening wedge distal femoral varus osteotomy using the Puddu plate and calcium phosphate bone cement. Knee Surg Sports Traumatol Arthrosc 2013; 21 (01) 249-254
- 4 Jacobi M, Wahl P, Bouaicha S, Jakob RP, Gautier E. Distal femoral varus osteotomy: problems associated with the lateral open-wedge technique. Arch Orthop Trauma Surg 2011; 131 (06) 725-728
- 5 Thein R, Bronak S, Thein R, Haviv B. Distal femoral osteotomy for valgus arthritic knees. J Orthop Sci 2012; 17 (06) 745-749
- 6 Zarrouk A, Bouzidi R, Karray B, Kammoun S, Mourali S, Kooli M. Distal femoral varus osteotomy outcome: Is associated femoropatellar osteoarthritis consequential?. Orthop Traumatol Surg Res 2010; 96 (06) 632-636
- 7 Backstein D, Morag G, Hanna S, Safir O, Gross A. Long-term follow-up of distal femoral varus osteotomy of the knee. J Arthroplasty 2007; 22 (04, Suppl 1): 2-6
- 8 Finkelstein JA, Gross AE, Davis A. Varus osteotomy of the distal part of the femur. A survivorship analysis. J Bone Joint Surg Am 1996; 78 (09) 1348-1352
- 9 Sternheim A, Garbedian S, Backstein D. Distal femoral varus osteotomy: unloading the lateral compartment: long-term follow-up of 45 medial closing wedge osteotomies. Orthopedics 2011; 34 (09) e488-e490
- 10 Kosashvili Y, Safir O, Gross A, Morag G, Lakstein D, Backstein D. Distal femoral varus osteotomy for lateral osteoarthritis of the knee: a minimum ten-year follow-up. Int Orthop 2010; 34 (02) 249-254
- 11 Forkel P, Achtnich A, Metzlaff S, Zantop T, Petersen W. Midterm results following medial closed wedge distal femoral osteotomy stabilized with a locking internal fixation device. Knee Surg Sports Traumatol Arthrosc 2015; 23 (07) 2061-2067
- 12 Wang JW, Hsu CC. Distal femoral varus osteotomy for osteoarthritis of the knee. J Bone Joint Surg Am 2005; 87 (01) 127-133
- 13 Paccola CAJ. Pre-operative planning and surgical technique of the open wedge supracondylar osteotomy for correction of valgus knee and fixation with a fixed-angle implant. Rev Bras Ortop 2015; 45 (06) 627-635
- 14 Elattar O, Swarup I, Lam A, Nguyen J, Fragomen A, Rozbruch SR. Open wedge distal femoral osteotomy: accuracy of correction and patient outcomes. HSS J 2017; 13 (02) 128-135
- 15 Lee SH, Song EK, Seon JK. Navigation system provides better functional outcomes of total knee arthroplasty. Form J Musculoskel Dis 2016; 7 (01) 8-16
- 16 Reising K, Strohm PC, Hauschild O. et al. Computer-assisted navigation for the intraoperative assessment of lower limb alignment in high tibial osteotomy can avoid outliers compared with the conventional technique. Knee Surg Sports Traumatol Arthrosc 2013; 21 (01) 181-188
- 17 Akamatsu Y, Mitsugi N, Mochida Y. et al. Navigated opening wedge high tibial osteotomy improves intraoperative correction angle compared with conventional method. Knee Surg Sports Traumatol Arthrosc 2012; 20 (03) 586-593
- 18 Ribeiro CH, Severino NR, Moraes de Barros Fucs PM. Opening wedge high tibial osteotomy: navigation system compared to the conventional technique in a controlled clinical study. Int Orthop 2014; 38 (08) 1627-1631
- 19 The Australian Orthopaedic Association National Joint Replacement Registry. Ad Hoc Report. Adelaide, Australia: AOA; 2019
- 20 Irrgang JJ, Anderson AF, Boland AL. et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 2001; 29 (05) 600-613
- 21 Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)–development of a self-administered outcome measure. J Orthop Sports Phys Ther 1998; 28 (02) 88-96
- 22 Saragaglia D, Chedal-Bornu B. Computer-assisted osteotomy for valgus knees: medium-term results of 29 cases. Orthop Traumatol Surg Res 2014; 100 (05) 527-530
- 23 Shivji FS, Foster A, Risebury MJ, Wilson AJ, Yasen SK. Ten-year survival rate of 89% after distal femoral osteotomy surgery for lateral compartment osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc 2020; DOI: 10.1007/s00167-020-05988-5.


