
Subscribe to RSS
DOI: 10.1055/s-0038-1669492
Recurrent Chronic Subdural Hematoma: Clinical and Imaging Risk Factors
Address for correspondence:
Publication History
Received: 10 March 2018
Accepted: 15 May 2018
Publication Date:
06 September 2018 (online)


Abstract
Background Chronic subdural hematoma (CSDH) is a major cause of neurosurgical emergencies in the elderly. Despite the use of routine surgical practices, recurrence of this condition is expected. This study was conducted to identify the risk factors (RF) for recurrent CSDH.
Methods Between January 2016 and July 2017, 103 consecutive patients suffering from CSDH were admitted to our department. The no-recurrence group (NRG) consisted of 91 patients, and the recurrence group (RG) consisted of 12 patients. To identify the RF involved in recurrent CSDH, we analyzed multiple factors, including patient comorbidities and imaging data.
Results Between the two groups, there were no statistical differences (p > 0.05) for head trauma, diabetes mellitus (DM), high blood pressure, heart diseases, anticoagulation agents, or seizures; however, DM was associated with one of the above-mentioned factors. In contrast, there were significant differences for antiplatelet agents (APA) (p < 10–6) and the right side of the hematoma location (p = 0.03).
Conclusion Although the literature highlights the controversy regarding RF for CSDH, we detected APA and the right side as RF, whereas DM alone or associated with another comorbidity does not affect the CSDH outcome.
#
Introduction
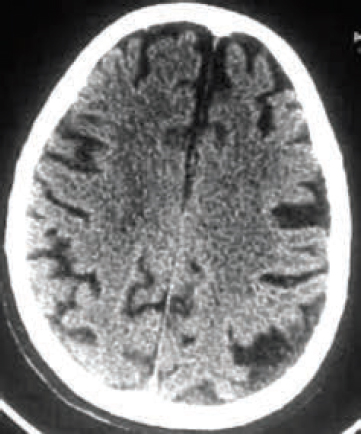
Chronic subdural hematoma (CSDH), a progressive spaceoccupying hematoma, is one of the most commonly encountered intracranial emergencies observed in the elderly and accounts for 15 to 20 new cases per 100,000 people in the United States per year. It is projected to reach 121.4 per 100,000 people by 2030, becoming the most common cranial neurosurgical condition among adults.[1] In the eastern world, a recent report[2] estimated that the CSDH incidence in Japan is 20.6 per 100,000 people per year for patients aged 70 to 79 years and is 127.1 per 100,000 people per year for patients older than 80 years. This is partially due to the wide availability of modern imaging, increased life expectancy, and use of anticoagulation and antiplatelet drugs for heart diseases. Today, patients often have multiple medical comorbidities. There is no consensus around the best surgical modality. Operative evacuation of the hematoma remains the gold standard of treatment for symptomatic CSDH. With appropriate and early treatment, the outcome is usually favorable with an improvement in clinical status and imaging restoration ([Figs. 1], [2]). However, in a significant number of cases, the patient outcome is complicated with persistent symptoms. Recurrences defined as the return of symptoms with reaccumulation of the hematoma are a real source of frustration for neurosurgeons and are not unique as reported by many authors. They require another operation after the initial surgery[3] [4] and must be differentiated from residual collections partially due to extensive brain atrophy. These are asymptomatic and do not typically require a second surgery. More rarely, no operative measures for unusual clinical and imaging presentations, such as hypertonic or hyperosmolar solutions, systemic glucocorticoids, or a therapeutic abstention policy, have been used with favorable results.[5] Prior reports show a recurrence rate of between 9.2 and 26%.[6] It is well established that risk factors (RF) play a central part in prediction and prevention. Their importance in the prevention of recurrent CSDH should be carefully considered. Although their findings are inconsistent, numerous studies have reported various potential RF.[4] [7] [8] [9] [10] [11] [12] [13] [14] [15] Three categories of factors have been recognized: patient comorbidities, imaging data, and surgical modalities. We performed this study to investigate the causal RF for CSDH and to determine whether there is a cumulative effect due to the association of diabetes mellitus (DM) with any other disease that would predict recurrence.

#
Material and Methods
Patient Selection
The patient population consisted of 103 CSDH patients who were treated in our department from July 2015 to December 2016. There were 78 (75.7%) males and 25 (24.3%) females. The mean age at diagnosis was 71.1 years, with a range from 20 to 96 years; 31 patients were older than 80, and 7 patients were older than 90. The potential RF considered for recurrent CSDH included the following: patient age, sex, history of head trauma, presence of DM, hypertension, heart disease, shunt, seizure, ischemic stroke ([Table 1]), DM associated with another comorbidity ([Table 2]), and preoperative imaging factors, such as hematoma location, midline displacement, and hematoma density ([Table 3]). Statistical analysis was performed using the chi-squared test and Fisher's exact test. Statistical significance was defined as a p ≤ 0.05.
#
Clinical Patient Details
In 69 (67%) patients, the presenting symptoms or clinical findings included headaches and/or neurologic deficits. Thirty-three (32%) patients exhibited disturbed conscious level at the time of presentation ([Table 4]). Recent minor or mild head trauma was recorded in 55 (53.4%) patients without surgical indication, bitemporal decompression in particular. The mean duration between the trauma and the diagnosis (range: 2–24 weeks) was of 6.86 weeks in the no-recurrence group (NRG) and 7.6 weeks in the recurrence group (RG). No history of hemorrhagic complication before admission was detected in patients using antiplatelet agent (APA) or anticoagulant (AC) agent. The incidence of concomitant diseases was as follows: hypertension and DM were the most common antecedents and were encountered in 45 (43.69%) and 23 (22.33%) patients, respectively. None of the patients presented with renal insufficiency. One patient underwent prior shunting. APA (clopidogrel, aspirin) and AC (acenocoumarol) medications were being taken by 18 (17.48%) and 11 (10.68%) patients, respectively. In patients with an international normalized ratio (INR) value of > 1.2, the main goal before surgery was to restore the normal coagulation profile. Values mandatory for the surgical procedure were an INR < 1.2, a prothrombin time of > 70%, a platelet count of > 100,000, and a hemoglobin level of >10 g/dL. For fresh frozen plasma (FFP), 10 to 15 mL/kg body weight and a slow intravenous infusion of 10 mg of vitamin K were administered with interruption of the coagulation therapy just prior to the surgery. In emergency cases, patients were operated on while receiving this treatment, whereas surgery was delayed 1 day for stable patient without impairing consciousness. All the demographic and comorbidity characteristics of the 103 patients are summarized in [Table 2]. Some patients presented multiple comorbidities (16, 15.53%) who suffered from DM and high blood pressure ([Table 3]).
#
Imaging Findings
By axial computed tomography (CT) scanning (thin cut, 5-mm intervals), CSDH was diagnosed as a crescent-shaped subdural mass and was usually hypodense. It was unilateral and was located on the left side in 34 (33.01%) patients, was on the right side in 32 (31.07%) patients, and was bilateral in the remaining 37 (35.92%) patients. The midline displacement was superior or equal to 10 mm in 45 (43.69%) cases. The imaging appearance was based on the density changes and was classified into the following groups: homogeneous appearance (hypodense, isodense, or slightly hyperdense relative to the gray matter of the brain) for 55 (53.4%) cases, heterogeneous with a variable signal intensity for 11 (10.68%) cases, and trabecular with membranes for 14 cases (13.59%) cases. For the remaining 23 (22.33%) cases, a recent bleeding aspect was observed. Concerning the brain atrophy, it was present in 13.2% in the NRG and 8.3% in the RG. These data are summarized in [Table 3]. Of the103 patients with 140 hemispheric CSDH, 37 were bilateral with a thickness that was < 16 mm. It varied from 16 to 24 mm in 49 cases and was between 24 and 32 mm in 39 other cases. It was above 32 mm in 15 cases (see [Table 3]).
#
Surgical Procedure and General Management
Three (2.91%) patients were treated conservatively with corticoids because they presented with mild headaches during normal clinical examination. CT scans revealed small hematomas with no important mass effects. Their follow-up included clinical and imaging monitoring.
Soon after diagnosis, 100 (97.09%) patients underwent surgical treatment of their CSDH. The mean time between admission and surgery was 6 to 8 hours and was rarely > 24 hours. The surgical management strategy used at our institution included one standard burr hole performed under local anesthesia without saline irrigation for 63 patients with unilateral CSDH and for 24 other patients with bilateral CSDH ([Table 5]). The 13 remaining patients with bilateral CSDH had more significant thickness and were operated on both sides during the same surgical session. In all cases, we inserted closed-system drainage. The tube was placed below the head level. This drainage was left in place for 48 hours. The operation time varied between 20 and 30 minutes (average time: 25 minutes). Usually, appropriate hydration and postoperative bed rest was undertaken for 2 days. Afterward, a semisitting position, standing, and walking were recommended to avoid vein thrombosis in the lower limbs, and consequently, the risk of pulmonary embolism. On average, the estimated amount of dark reddish fluid drainage was 139.9 mL. The mean length of hospitalization was 2.75 days (range: 2–8 days). A craniotomy was performed on two patients as a third procedure following failure of the burr hole approach. The size was frontotemporoparietal in one case and frontoparietal in the other case. Postoperative intracranial pressure monitoring was not realized in our patients.
#
#
Results
Of the 100 patients with CSDH in 137 hemispheres that were treated surgically, 12 (11, 65%) with recurrences were readmitted because of symptom return. Imaging confirmed the recurrence. The average time after hospital discharge was 17.63 days. Two patients required more than one reoperation. The location of the hematoma recurrence was in the right hemisphere in seven patients, bilateral in four patients, and on the left side in one case ([Figs. 3], [4]). These figures show the bilateral hematoma at admission ([Fig. 3]) and the recurrence on the left side that required a second procedure ([Fig. 4]). The mean age of these nine men and three women was 73.25 years (range: 45–96). No significant differences between the NRG and the RG were observed regarding head trauma (p = 0.30), hypertension (p = 0.08), DM (p = 0.33), history of using anticoagulation agents p = 0.47), heart disease (p = 0.15), or seizures (p = 0.55). Of the 18 (17.48%) patients who were prescribed APA, warfarin, or aspirin, 6 (5.83%) required a second surgery. A significant difference (p < 10-6) was observed upon comparing this factor between the RG and NRG ([Table 1]). However, no significant differences were observed for the association of DM with any other comorbidity ([Table 2]). According to the imaging data (location, density, and thickness of the hematoma), there was no statistically significant difference between the two groups, except for the right location (p = 0.03) ([Table 3]).


Outcome
The morbidity in this study included one case of meningitis that was sufficiently treated with appropriate antibiotics, a wound infection in 1 patient, seizure in 5 patients, asymptomatic pneumocephalus 5 cases, and 12 cases of recurrence as mentioned previously. As for mortality, three patients died during the period of hospitalization. The first was a 91-year-old man with a history of hypertension, stroke, DM, and coagulation disorders who was operated on three times. His last procedure consisted of an evacuation through a craniotomy. He developed septicemia due to severe pneumonia. The second was 90 years old with medical records of impaired coagulation. After a slight clinical improvement during the first postoperative hours, his status worsened gradually via respiratory distress syndrome. His brain CT scan showed a fatal acute subdural hematoma. Diagnosis of associated pulmonary embolism was also suspected without confirmation via CT angiogram. The third patient, a 96-year-old man was admitted having a poor general health condition and altered mental status with stupor. The CT scan confirmed a bilateral CSDH. The procedure consisted of drainage through one right burr hole. The same clinical examination persisted after this surgery. A new CT scan showed a recurrent hematoma, which was evacuated via two right burr holes on the same side. Deterioration of his neurologic status, pneumonia, and postoperative renal insufficiency were the milestones of the inevitable outcome.
#
Discussion
According to D'Errico and German,[16] J. Johannes Wepfer was the first to describe an authentic report of CSDH in 1657. Gratifying clinical results corroborated by imaging are usually achieved ([Figs. 1], [2]). Morbidity and mortality are comparable with those observed for surgeries of other brain space-occupying lesions. In contrast, the rate of recurrence is relatively high at 26% ([Figs. 3], [4]). The issue of recurrence still is a matter of debate as illustrated by the following report titles: “Can Recurrence of Chronic Subdural Hematoma Be Predicted?”[17] and “Is the Recurrence Rate of Chronic Subdural Hematomas Dependent on the Duration of Drainage?”[18] In this report, 12 (11.65%) patients showed a recurrence of their hematoma. There were 18 (12%) recurrences among the 149 CSDH cases in the study by Kale et al,[18] nine (10%) recurrences in 90 patients in the study by Han[9] who identified 104 (13.8%) patients with recurrence after surgery for CSDH in a group of 756 patients. However, there is a large amount of variability in the literature concerning this second surgery (see [Table 6]). To understand this significant rate of recurrence, neurosurgeons continue to pay particular attention to factors that increase the likelihood of developing recurrent CSDH. RF has not been formally established; however, previous studies, which are sometimes dissimilar, have identified some RF in terms of patient characteristics, imaging data, and treatment. In this study, numerous factors, such as head trauma, hypertension, DM, history of using anticoagulation agents, APA, heart disease, seizures, hematoma location, midline displacement, and thickness of the hematoma, were considered.
#
Patient Characteristics
Seventy-five patients were older than 60, 31 were older than 80, and 7 were older than 90. Age and sex were not statistically significant in our study. Some authors[9] [11] have suggested that advanced age is an independent factor for recurrence. Concerning the patient's memory of a slight head injury, this was observed in the disease history for only approximately one-half (53.4%) of the patients, and five were in the RG. This is in accordance with the data in the literature. In our study, underlying medical diseases, such as hypertension, heart diseases, and seizures, were also not related to the recurrence of CSDH. Given the increasing number of diabetic patients worldwide, current estimates of DM prevalence by 2030 is 439 million adults worldwide.[19] We were interested in the DM factor and the association of DM with other diseases, which has not been reported. In our study, we recorded 23 (22.33%) patients with DM, and 4 cases were in the RG. DM alone or associated with a concomitant disease was not an RF for recurrence in our study. The significance of DM as an independent RF for recurrence is still inconsistent.[11] In 2017, Abdelsadg et al[4] conducted a systematic review to evaluate the available literature that addresses the RF for CSDH recurrence and found that the role of persistent hyperglycemia in CSDH recurrence is controversial. Many authors have demonstrated that DM is an independent predictor of the recurrence of CSDH.[7] [13] The exudate of macrocapillaries in the outer membrane has shown to influence the recurrence of CSDH as mentioned by Song.[11] In contrast, Yamamoto et al[15] found that patients without DM had a higher recurrence rate than those with DM. They asserted that DM decreases rebleeding in CSDH patients because the blood of patients with DM has a hyperviscosity, high osmotic pressure, and increased platelet aggregation. Our results support a clear association between APA and recurrent CSDH (p < 10−6). This is consistent with the report by Rust et al[20] who reported that there is a 42.5 times higher possibility of developing CSDH when taking warfarin (APA) compared with those who are not taking this drug. Wang et al[21] performed meta-analysis of 10 studies and showed that thrombotic agents were RF for CSDH. For Wada et al,[14] preoperative oral APA administration was significantly associated with a higher level of recurrence. This relationship disappeared when this factor was associated with DM (p = 0.22). Other studies are not always consistent. Suarez and Kapinos[12] and Fujitani et al[8] found no relationship between the use of these medications and rebleeding.
#
Imaging Features
Concerning the location, our study is consistent with the literature data that show that the left predominance of CSDH is influenced by anatomical asymmetry of the cranium (being more flat on the right side). However, a significant difference was observed (p = 0.03) for the right side, which was more affected in the 7 (58.33%) patients in the RG than in the 25 (27.47%) patients in the NRG. To our knowledge, this is the first report of such findings. Further research will be required to confirm this result. It is well known that patients are advised, after their first intervention, not to sleep on the operated side of the head, which is commonly the left side. Residual fluid or recurrent hematoma may collect easier in the right side, especially in a lateral decubitus position according to the laws of physics and cerebrospinal fluid circulation. This explanation may be particularly relevant in the case of a CSDH with homogeneous appearance on the CT scan. According to our analysis of the literature data, controversial findings have been reported. In the study by Huang et al,[22] a recurrence rate of up to 28.00% was observed for the bilateral disease, which was higher than 9.59% for the unilateral disease (p = 0.042). Although it was not a statistically significant difference, unilateral CSDH has been more frequently related to recurrent CSDH in some studies.[12] Mixed-density hematoma and midline displacement are independent factors for unilateral CSDH recurrence.[8] Heterogeneous hematomas and bilaterality are significant RF as shown by preoperative CT findings.[11] Amirdjamshidi et al[23] and Oishi et al[24] showed that high-density hematoma was significantly associated with recurrence of CSDH. Septated hematomas are more difficult to drain because disruption of each compartment is necessary for complete drainage, and they are significantly related with recurrence.[11]
#
Treatment
From the surgical point of view, our procedure included the one burr hole drainage procedure without saline irrigation, which was performed in 63 cases of unilateral CSDH. Twenty-four cases of bilateral location were evacuated using this technique. Surgery on both sides was realized in the 13 remaining cases, which were associated with severe thickness of the hematoma; 11 of these were in the NRG and 2 were in the RG. In all cases, we inserted closedsystem drainage. This approach was dictated by our daily practice. No parameter seemed to us worthy of study. On the opposite, for Sundaravadhanan and Deb,[25] it is essential to excise the culprit membrane through craniotomy to prevent recurrences. Finally, larger amounts of residual air in the postoperative hematoma cavity were associated with recurrence of CSDH.[23] [24]
#
Limitations of the Study
The limitations of this study include the small sample size and the patient population in which all patients were from the same district and were managed according to the experience of one surgical team. Concerning the RF, other uncommon parameters, such as alcohol abuse, smoking, and residual air in the hematoma cavity were not evaluated in this study. Despite these limitations, our report provides new contingent RF for recurrent CSDH. Future studies are required to confirm or to invalidate the right location of the cranium as the predilection. Studies should be focused on possible causes, such as patient characteristics, especially skull anatomy, the outcome including the head position, duration of drainage, and presence or not of pneumocephalus.
#
#
Conclusion
Many published studies have attempted to identify the RF leading to recurrent CSDH. There is currently no consensus regarding these RF that could be implicated. Our results confirm, on the one hand, the results of other studies, APA are an RF for recurrent CSDH and invalidate, on the other hand, the association of DM with other concomitant diseases, which was our first postulation and has never been studied before. Moreover, our analysis indicates that the right side of the cranium appears to be more frequently affected than the left.
Note
Our study was conducted in accordance with the Helsinki Declaration. In June 2015, it was approved by the ethics committee, and informed consent was obtained from each patient or from a member of the patient's family.
#
#
#
Conflict of Interest
None.
Acknowledgments
This survey would not have been possible without the efforts of our colleagues Lila Mahfouf, Faycal Bouatta, Lakhdar Guenane, Magdouda Bouallegue, Faycal Aichaoui, Said Khider, Abderrahmane Tikanouine, Brahim Merouche, and Idir Moula, who also operated these patients.
-
References
- 1 Balser D, Farooq S, Mehmood T, Reyes M, Samadani U. Actual and projected incidence rates for chronic subdural hematomas in United States Veterans Administration and civilian populations. J Neurosurg 2015; 123 (05) 1209-1215
- 2 Karibe H, Kameyama M, Kawase M, Hirano T, Kawaguchi T, Tominaga T. Epidemiology of chronic subdural hematomas. [in Japanese] No Shinkei Geka 2011; 39 (12) 1149-1153
- 3 Stavrinou P, Katsigiannis S, Lee JH. et al. Risk factors for chronic subdural hematoma recurrence identified using quantitative computed tomography analysis of hematoma volume and density. World Neurosurg 2017; 99: 465-470
- 4 Abdelsadg M, Kanodia AK, Abbas A, Sheikh A. Chronic subdural haematoma: Systematic review highlighting risk factors for recurrent bleeds. Neuro Open J 2017; 4: 16-24
- 5 Soleman J, Nocera F, Mariani L. The conservative and pharmacological management of chronic subdural haematoma. Swiss Med Wkly 2017; 147: w14398
- 6 Torihashi K, Sadamasa N, Yoshida K, Narumi O, Chin M, Yamagata S. Independent predictors for recurrence of chronic subdural hematoma: a review of 343 consecutive surgical cases. Neurosurgery 2008; 63 (06) 1125-1129 discussion 1129
- 7 Chon KH, Lee JM, Koh EJ, Choi HY. Independent predictors for recurrence of chronic subdural hematoma. Acta Neurochir (Wien) 2012; 154 (09) 1541-1548
- 8 Fujitani S, Ishikawa O, Miura K, Takeda Y, Goto H, Maeda K. Factors predicting contralateral hematoma growth after unilateral drainage of bilateral chronic subdural hematoma. J Neurosurg 2017; 126 (03) 755-759
- 9 Han MH, Ryu JI, Kim CH, Kim JM, Cheong JH, Yi HJ. Predictive factors for recurrence and clinical outcomes in patients with chronic subdural hematoma. J Neurosurg 2017; 127 (05) 1117-1125
- 10 Qian Z, Yang D, Sun F, Sun Z. Risk factors for recurrence of chronic subdural hematoma after burr hole surgery: potential protective role of dexamethasone. Br J Neurosurg 2017; 31 (01) 84-88
- 11 Song DH, Kim YS, Chun HJ. et al. The predicting factors for recurrence of chronic subdural hematoma treated with burr hole and drainage. Korean J Neurotrauma 2014; 10 (02) 41-48
- 12 Suarez JI, Kapinos G. Thromboembolism prevention after chronic subdural hematoma in the elderly: a leap in the dark. Neurology 2017; 88 (20) 1880-1881
- 13 Tokmak M, Iplikcioglu AC, Bek S, Gökduman CA, Erdal M. The role of exudation in chronic subdural hematomas. J Neurosurg 2007; 107 (02) 290-295
- 14 Wada M, Yamakami I, Higuchi Y. et al. Influence of antiplatelet therapy on postoperative recurrence of chronic subdural hematoma: a multicenter retrospective study in 719 patients. Clin Neurol Neurosurg 2014; 120: 49-54
- 15 Yamamoto H, Hirashima Y, Hamada H, Hayashi N, Origasa H, Endo S. Independent predictors of recurrence of chronic subdural hematoma: results of multivariate analysis performed using a logistic regression model. J Neurosurg 2003; 98 (06) 1217-1221
- 16 D'Errico AP, German WJ. Chronic subdural hematoma. Yale J Biol Med 1930; 3 (01) 11-20
- 17 Tugcu B, Tanriverdi O, Baydin S. et al. Can recurrence of chronic subdural hematoma be predicted? A retrospective analysis of 292 cases. J Neurol Surg A Cent Eur Neurosurg 2014; 75 (01) 37-41
- 18 Kale A, Öz İİ, Gün EG, Kalaycı M, Gül Ş. Is the recurrence rate of chronic subdural hematomas dependent on the duration of drainage?. Neurol Res 2017; 39 (05) 399-402
- 19 Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010; 87 (01) 4-14
- 20 Rust T, Kiemer N, Erasmus A. Chronic subdural haematomas and anticoagulation or anti-thrombotic therapy. J Clin Neurosci 2006; 13 (08) 823-827
- 21 Wang Y, Zhou J, Fan C. et al. Influence of antithrombotic agents on the recurrence of chronic subdural hematomas and the quest about the recommencement of antithrombotic agents: a meta-analysis. J Clin Neurosci 2017; 38: 79-83
- 22 Huang YH, Yang K-Y, Lee T-C, Liao C-C. Bilateral chronic subdural hematoma: What is the clinical significance?. Int J Surg 2013; 11: 544-548
- 23 Amirjamshidi A, Abouzari M, Eftekhar B. et al. Outcomes and recurrence rates in chronic subdural haematoma. Br J Neurosurg 2007; 21 (03) 272-275
- 24 Oishi M, Toyama M, Tamatani S, Kitazawa T, Saito M. Clinical factors of recurrent chronic subdural hematoma. Neurol Med Chir (Tokyo) 2001; 41 (08) 382-386
- 25 Sundaravadhanan S, Deb P. Chronic subdural hematoma: role of vascular endothelial growth factor and craniotomy in pathophysiology and prevention of recurrence. Indian J Neurotrauma 2017; 14 (01) 1-5
Address for correspondence:
-
References
- 1 Balser D, Farooq S, Mehmood T, Reyes M, Samadani U. Actual and projected incidence rates for chronic subdural hematomas in United States Veterans Administration and civilian populations. J Neurosurg 2015; 123 (05) 1209-1215
- 2 Karibe H, Kameyama M, Kawase M, Hirano T, Kawaguchi T, Tominaga T. Epidemiology of chronic subdural hematomas. [in Japanese] No Shinkei Geka 2011; 39 (12) 1149-1153
- 3 Stavrinou P, Katsigiannis S, Lee JH. et al. Risk factors for chronic subdural hematoma recurrence identified using quantitative computed tomography analysis of hematoma volume and density. World Neurosurg 2017; 99: 465-470
- 4 Abdelsadg M, Kanodia AK, Abbas A, Sheikh A. Chronic subdural haematoma: Systematic review highlighting risk factors for recurrent bleeds. Neuro Open J 2017; 4: 16-24
- 5 Soleman J, Nocera F, Mariani L. The conservative and pharmacological management of chronic subdural haematoma. Swiss Med Wkly 2017; 147: w14398
- 6 Torihashi K, Sadamasa N, Yoshida K, Narumi O, Chin M, Yamagata S. Independent predictors for recurrence of chronic subdural hematoma: a review of 343 consecutive surgical cases. Neurosurgery 2008; 63 (06) 1125-1129 discussion 1129
- 7 Chon KH, Lee JM, Koh EJ, Choi HY. Independent predictors for recurrence of chronic subdural hematoma. Acta Neurochir (Wien) 2012; 154 (09) 1541-1548
- 8 Fujitani S, Ishikawa O, Miura K, Takeda Y, Goto H, Maeda K. Factors predicting contralateral hematoma growth after unilateral drainage of bilateral chronic subdural hematoma. J Neurosurg 2017; 126 (03) 755-759
- 9 Han MH, Ryu JI, Kim CH, Kim JM, Cheong JH, Yi HJ. Predictive factors for recurrence and clinical outcomes in patients with chronic subdural hematoma. J Neurosurg 2017; 127 (05) 1117-1125
- 10 Qian Z, Yang D, Sun F, Sun Z. Risk factors for recurrence of chronic subdural hematoma after burr hole surgery: potential protective role of dexamethasone. Br J Neurosurg 2017; 31 (01) 84-88
- 11 Song DH, Kim YS, Chun HJ. et al. The predicting factors for recurrence of chronic subdural hematoma treated with burr hole and drainage. Korean J Neurotrauma 2014; 10 (02) 41-48
- 12 Suarez JI, Kapinos G. Thromboembolism prevention after chronic subdural hematoma in the elderly: a leap in the dark. Neurology 2017; 88 (20) 1880-1881
- 13 Tokmak M, Iplikcioglu AC, Bek S, Gökduman CA, Erdal M. The role of exudation in chronic subdural hematomas. J Neurosurg 2007; 107 (02) 290-295
- 14 Wada M, Yamakami I, Higuchi Y. et al. Influence of antiplatelet therapy on postoperative recurrence of chronic subdural hematoma: a multicenter retrospective study in 719 patients. Clin Neurol Neurosurg 2014; 120: 49-54
- 15 Yamamoto H, Hirashima Y, Hamada H, Hayashi N, Origasa H, Endo S. Independent predictors of recurrence of chronic subdural hematoma: results of multivariate analysis performed using a logistic regression model. J Neurosurg 2003; 98 (06) 1217-1221
- 16 D'Errico AP, German WJ. Chronic subdural hematoma. Yale J Biol Med 1930; 3 (01) 11-20
- 17 Tugcu B, Tanriverdi O, Baydin S. et al. Can recurrence of chronic subdural hematoma be predicted? A retrospective analysis of 292 cases. J Neurol Surg A Cent Eur Neurosurg 2014; 75 (01) 37-41
- 18 Kale A, Öz İİ, Gün EG, Kalaycı M, Gül Ş. Is the recurrence rate of chronic subdural hematomas dependent on the duration of drainage?. Neurol Res 2017; 39 (05) 399-402
- 19 Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010; 87 (01) 4-14
- 20 Rust T, Kiemer N, Erasmus A. Chronic subdural haematomas and anticoagulation or anti-thrombotic therapy. J Clin Neurosci 2006; 13 (08) 823-827
- 21 Wang Y, Zhou J, Fan C. et al. Influence of antithrombotic agents on the recurrence of chronic subdural hematomas and the quest about the recommencement of antithrombotic agents: a meta-analysis. J Clin Neurosci 2017; 38: 79-83
- 22 Huang YH, Yang K-Y, Lee T-C, Liao C-C. Bilateral chronic subdural hematoma: What is the clinical significance?. Int J Surg 2013; 11: 544-548
- 23 Amirjamshidi A, Abouzari M, Eftekhar B. et al. Outcomes and recurrence rates in chronic subdural haematoma. Br J Neurosurg 2007; 21 (03) 272-275
- 24 Oishi M, Toyama M, Tamatani S, Kitazawa T, Saito M. Clinical factors of recurrent chronic subdural hematoma. Neurol Med Chir (Tokyo) 2001; 41 (08) 382-386
- 25 Sundaravadhanan S, Deb P. Chronic subdural hematoma: role of vascular endothelial growth factor and craniotomy in pathophysiology and prevention of recurrence. Indian J Neurotrauma 2017; 14 (01) 1-5