

Subscribe to RSS
DOI: 10.1055/s-0034-1367732
Posttraumatic Cartilage Calcification of the Knee: A Case Report
Authors
Abstract
A 24-year-old woman presented with a calcium deposit within the articular cartilage of her knee after an antecedent minor trauma. Arthroscopic examination revealed the articular surface of the lateral tibial plateau yielded easily to pressure by probing. Calcium-containing crystals within the articular cartilage was identified and debrided. Magnetic resonance images taken 4 years after operation showed the articular cartilage was completely repaired. This is the first report that demonstrated a painful well-defined calcium deposit detected by conventional radiography within the articular cartilage of the knee.
Calcium deposits are often seen at tendon insertions around the joint and causes acute periarthritis mimicking gouty arthritis or pseudogout.[1] It is reported that calcium deposition other than monosodium urate or calcium pyrophosphate dihydrate occurs in articular cartilages or menisci of the knee with aging or progression of osteoarthritis.[2] [3] However, the size of the deposit of calcium-containing crystals is tiny and seldom detected by conventional radiography. Our case concerns a 24-year-old woman with a large calcium deposit in the articular cartilage of the tibial plateau. An antecedent minor trauma may have contributed to the calcium deposition. This is the first report that demonstrated how a painful well-defined calcium deposit was detected by conventional radiography within the articular cartilage.
Case Report
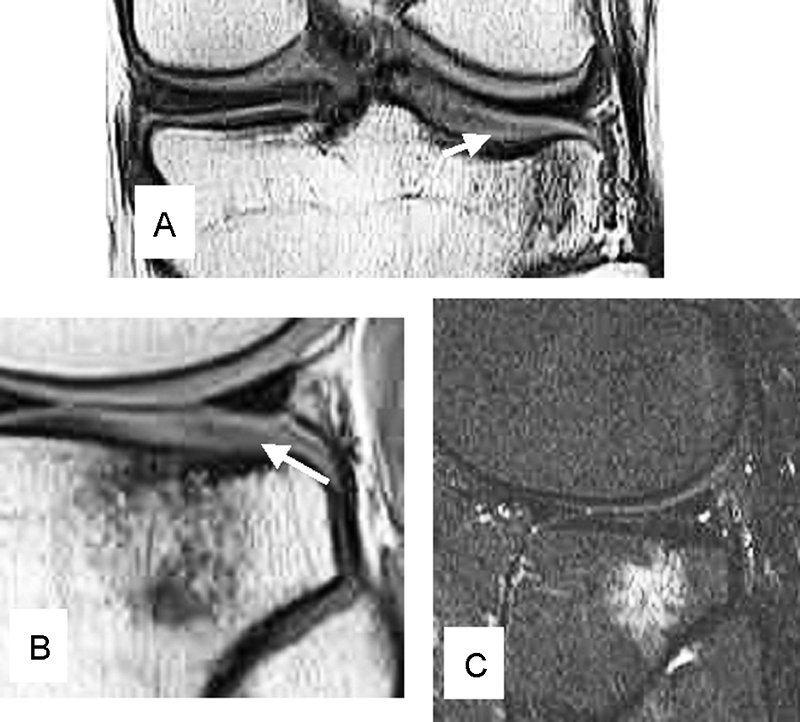
An otherwise healthy 24-year-old woman presented at our hospital with a 3-day history of sudden and severe left knee pain. She had fallen from stairs and twisted her left knee 3 months earlier but she had no symptoms about the knee thereafter. Her job was a nurse. Her body weight was 62 kg and was 172 cm tall, with negative findings from blood and urine examinations. Clinical examinations of the left knee revealed a full range of motion without anterior, posterior, or lateral instability. No swelling, warmness, erythema, tenderness (including the joint line), or hydrops were found around the knee. A McMurray test elicited pain over the lateral aspect of the joint line. Plain radiography and computed tomography (CT) of the left knee revealed a well-delineated homogeneous and amorphous cuboid free body measuring 5 × 5 × 5 mm without trabecular structures in the lateral femorotibial joint ([Fig. 1A–C]). Magnetic resonance images (MRIs) showed a cubic low signal intensity area on T2-weighted, proton, and short-T1 inversion recovery (STIR) images within the articular cartilage of the lateral tibial plateau and high signal intensity area in the bone marrow underneath on STIR image ([Fig. 2A–C]). The diagnosis of bone bruise with cartilage degeneration of the lateral tibial plateau or free body in the lateral femorotibial joint space was suspected. Arthroscopic surgery was performed after informed consent was obtained from the patient. Cartilage of the patella was soft by probing (grade 1 chondromalacia by Outerbridge classification[4] ([Fig. 3A]). The medial compartment including medial meniscus and cartilage was normal. Anterior cruciate ligament (ACL) was loose by probing with a superficial longitudinal tear of ACL ([Fig. 3B]). Lateral meniscus and cartilage of the lateral femoral condyle were intact. White chalk-like deposits within the articular cartilage of the lateral tibial plateau were identified. The surface of the central and posterior area of the lateral tibial plateau yielded to pressure by probing ([Fig. 3C]). Cartilage overlying chalk-like deposits was excised, then the calcium crystals exploded ([Fig. 3D]). Calcium crystals were entirely excised until subchondral bone was exposed. On microscopic examination, the crystals of the chalk-like deposits were round in shape with irregular precipitates of various sizes and not birefringent ([Fig. 4]). However, the exact nature of the crystals was not identified. Passive and active range of motion of the knee was started immediately after the operation. Partial weight bearing gait was allowed from 1 day postoperatively and full weight bearing gait was allowed from 2 weeks after the operation. Abnormal intensity area under the lateral tibial plateau judged by MRI enlarged gradually postoperatively concomitant with knee pain maximizing at 1 year postoperation and then diminished gradually. Articular cartilage of the lateral tibial plateau was completely repaired although abnormal signal intensity in the bone marrow still remained on MRI taken 4 years after operation ([Fig. 5A–C]). The patient's knee pain completely disappeared and she has had no difficulty in her job during the 4-year follow-up period.




Discussion
It is well known that there are mainly three types of crystals that induce crystal-related arthropathies or periarthritis. Those are monosodium urate, calcium pyrophosphate dihydrate, and calcium hydroxyapatite.[5] Crystals in calcium deposits causing periarthritis are predominantly hydroxyapatite crystals. Calcium deposits other than calcium pyrophosphate dihydrate in articular cartilage are rarely reported and are associated with aging and osteoarthritis; however, the nature of the deposits has not been elucidated in the literature.[2] [3] Clinical presentations including sudden onset of severe knee pain and well-defined localized calcification on plain and CT radiographies in our case suggested that crystals within the articular cartilage might be hydroxyapatite.[1] Also, microscopic appearance of the crystals resembled hydroxyapatite crystals with respect to their round shape with irregular precipitates of various sizes.[5] [6] However, many crystals deposited within the articular cartilage other than the above three major crystals, such as octacalcium phosphate, calcium oxalate, and calcium carbonate, have been reported.[7] We could not conclude the exact nature of the crystals in our case since further analyses by electron microscopy, infrared, or chemical studies were not done.
Articular cartilage in the entire depth, except the surface of the lateral tibial plateau, was replaced by calcium crystals in this case. The calcium deposit was relatively large with a size of 5 × 5 × 5 mm. According to Suan et al, calcium deposits within the articular cartilages or menisci were detected as the small punctuate hypointensity regions using 4 T MRI in three cases aged between 54 and 68 years.[2] Mitsuyama et al demonstrated that 106 knees, provided by tissue banks or local hospitals, had some measurable calcification detected by using a Faxitron radiography system on 7- to 10-mm-thick condyle specimens.[3] And with aging or progression of osteoarthritis, calcium deposits within the articular cartilage are too tiny to be detected by conventional radiography, CT, or MRI.
Superficial longitudinal tears of the ACL from arthroscopic examination and the bone bruise of the lateral tibial plateau detected by MRI on the initial visit suggested that valgus force was loaded to the affected knee at an antecedent trauma 3 months before the initial visit. The bone bruise was predominantly detected in the lateral tibial plateau as well as the lateral femoral condyle at the event of ACL injury.[8] [9] [10] [11] The lateral tibial plateau might be vulnerable to impaction more than the lateral femoral condyle. According to Theologis et al, chondral damage detected by quantitative T1ρ MRI of the lateral tibial plateau was prolonged more than that of the lateral femoral condyle in a 1-year cohort study on patients with ACL injuries.[11] Grade 1 chondromalacia patella was observed during arthroscopic surgery in the present patient. However, cartilage in the medial compartment and lateral femoral condyle was normal by probing. A large area of the lateral tibial plateau was extremely soft and yielded to pressure in the operative finding. The articular cartilage of the lateral tibial plateau might be so deformed by the impaction of the lateral femoral condyle that it could result in necrosis. It is uncertain if the chondromalacia patella was associated with the calcium deposit within the articular cartilage of the lateral tibial plateau.
As far as calcific periarthritis is concerned, calcifications developed in necrotic tissue in a zone of relatively avascularity, possibly secondary to local changes in pH according to Pedersen and Key.[12] The environment around the impacted articular cartilage might be the same as for the occurrence of periarthritic calcium deposition since cartilage is avascular tissue. Necrosis of the cartilage could be a trigger for calcium deposition although the exact etiology of calcium deposition within cartilage is uncertain.
Postoperative MRI revealed the area of bone bruise of the tibial plateau enlarged transiently and the bone bruise still remained after 4 years postoperatively. The bone bruise in the lateral compartment of the knee accompanied by ACL ruptures was resolved during a 2-year follow-up after successful ACL reconstruction surgery in 71% of 21 patients with acute ACL ruptures.[9] The majority of knees with persistent abnormality on MRI had disruption or depression of the normal contour of the cortical surface at the initial MRI as seen in this case. Weight bearing should not be allowed for a longer period until the cartilage repair is confirmed by MRI. Nevertheless, the full thickness defect of the cartilage completely recovered judged by MRI during the 4-year interval.
This case is an entirely different clinical entity from calcium deposition within cartilage that is commonly seen with aging or osteoarthritis. First, the patient's age (24 years old) is young with no evidence of osteoarthritis of the affected knee. Second, the size of calcification is relatively large to be detected by conventional plain radiography. Third, onset of knee pain was sudden and severe. Calcium deposits within articular cartilage due to aging or osteoarthritis are commonly asymptomatic. Comparing MRIs preoperatively with postoperatively, the width of the corresponding cartilage layer in the former expanded more than that in the latter. No breakage of surface of the lateral tibial plateau was observed during arthroscopic surgery. Thus, elevated pressure within the cartilage might have caused the sudden onset of symptoms, similar to cases of calcifying tendonitis. This is the first case report where a well-defined calcium deposit was detected by conventional radiography within the articular cartilage after a minor trauma; repair of the cartilage defect resulted in complete recovery over a long-term period. Foreign bodies, osteochondritis dissecans, meniscal ossicle, or osteochondromatosis should be differentiated from this clinical entity.
-
References
- 1 Hayes CW, Conway WF. Calcium hydroxyapatite deposition disease. Radiographics 1990; 10 (6) 1031-1048
- 2 Suan JC, Chhem RK, Gati JS, Norley CJ, Holdsworth DW. 4 T MRI of chondrocalcinosis in combination with three-dimensional CT, radiography, and arthroscopy: a report of three cases. Skeletal Radiol 2005; 34 (11) 714-721
- 3 Mitsuyama H, Healey RM, Terkeltaub RA, Coutts RD, Amiel D. Calcification of human articular knee cartilage is primarily an effect of aging rather than osteoarthritis. Osteoarthritis Cartilage 2007; 15 (5) 559-565
- 4 Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br 1961; 43-B: 752-757
- 5 Schumacher HR. Crystal-induced arthritis: An overview. Am J Med 1996; 100 (2) 46-52
- 6 Paul H, Reginato AJ, Schumacher HR. Alizarin red S staining as a screening test to detect calcium compounds in synovial fluid. Arthritis Rheum 1983; 26 (2) 191-200
- 7 Boskey AL. Pathogenesis of cartilage calcification: mechanisms of crystal deposition in cartilage. Curr Rheumatol Rep 2002; 4 (3) 245-251
- 8 Snearly WN, Kaplan PA, Dussault RG. Lateral-compartment bone contusions in adolescents with intact anterior cruciate ligaments. Radiology 1996; 198 (1) 205-208
- 9 Costa-Paz M, Muscolo DL, Ayerza M, Makino A, Aponte-Tinao L. Magnetic resonance imaging follow-up study of bone bruises associated with anterior cruciate ligament ruptures. Arthroscopy 2001; 17 (5) 445-449
- 10 Nishimori M, Deie M, Adachi N , et al. Articular cartilage injury of the posterior lateral tibial plateau associated with acute anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 2008; 16 (3) 270-274
- 11 Theologis AA, Kuo D, Cheng J , et al. Evaluation of bone bruises and associated cartilage in anterior cruciate ligament-injured and -reconstructed knees using quantitative t(1ρ) magnetic resonance imaging: 1-year cohort study. Arthroscopy 2011; 27 (1) 65-76
- 12 Pedersen HE, Key JA. Pathology of calcareous tendinitis and subdeltoid bursitis. Arch Surg 1951; 62: 50-63
Address for correspondence
-
References
- 1 Hayes CW, Conway WF. Calcium hydroxyapatite deposition disease. Radiographics 1990; 10 (6) 1031-1048
- 2 Suan JC, Chhem RK, Gati JS, Norley CJ, Holdsworth DW. 4 T MRI of chondrocalcinosis in combination with three-dimensional CT, radiography, and arthroscopy: a report of three cases. Skeletal Radiol 2005; 34 (11) 714-721
- 3 Mitsuyama H, Healey RM, Terkeltaub RA, Coutts RD, Amiel D. Calcification of human articular knee cartilage is primarily an effect of aging rather than osteoarthritis. Osteoarthritis Cartilage 2007; 15 (5) 559-565
- 4 Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br 1961; 43-B: 752-757
- 5 Schumacher HR. Crystal-induced arthritis: An overview. Am J Med 1996; 100 (2) 46-52
- 6 Paul H, Reginato AJ, Schumacher HR. Alizarin red S staining as a screening test to detect calcium compounds in synovial fluid. Arthritis Rheum 1983; 26 (2) 191-200
- 7 Boskey AL. Pathogenesis of cartilage calcification: mechanisms of crystal deposition in cartilage. Curr Rheumatol Rep 2002; 4 (3) 245-251
- 8 Snearly WN, Kaplan PA, Dussault RG. Lateral-compartment bone contusions in adolescents with intact anterior cruciate ligaments. Radiology 1996; 198 (1) 205-208
- 9 Costa-Paz M, Muscolo DL, Ayerza M, Makino A, Aponte-Tinao L. Magnetic resonance imaging follow-up study of bone bruises associated with anterior cruciate ligament ruptures. Arthroscopy 2001; 17 (5) 445-449
- 10 Nishimori M, Deie M, Adachi N , et al. Articular cartilage injury of the posterior lateral tibial plateau associated with acute anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 2008; 16 (3) 270-274
- 11 Theologis AA, Kuo D, Cheng J , et al. Evaluation of bone bruises and associated cartilage in anterior cruciate ligament-injured and -reconstructed knees using quantitative t(1ρ) magnetic resonance imaging: 1-year cohort study. Arthroscopy 2011; 27 (1) 65-76
- 12 Pedersen HE, Key JA. Pathology of calcareous tendinitis and subdeltoid bursitis. Arch Surg 1951; 62: 50-63