

RSS-Feed abonnieren
DOI: 10.1055/s-0032-1306287
Is Circulating Osteocalcin Related to Adipokines and Overweight/Obesity in Children and Adolescents?
Autor*innen
Correspondence
Publikationsverlauf
received 06. Oktober 2011
first decision 10. Februar 2012
accepted 13. Februar 2012
Publikationsdatum:
22. März 2012 (online)

Abstract
Background:
Osteocalcin (OC) has recently been described to be involved in the regulation of glucose and energy metabolism. We aimed to evaluate whether or not OC serum levels were related to parameters of overweight and serum adipokine levels of healthy children and adolescents in dependence on gender and pubertal stage.
Methods:
In a cross sectional study (Leipzig Schoolchildren Project) 497 healthy, caucasian children and adolescents of all pubertal stages were included. We measured anthropometric data height, weight, fat mass, waist-to-hip ratio, pubertal development and performed biochemical analyses of osteocalcin, leptin, adiponectin and resistin serum levels by immunoassay.
Results:
OC serum levels were associated with pubertal development achieving peak values at Tanner stage 3. There was no significant association of OC serum levels with overweight and obesity as measured by BMI and WHR. In addition, OC demonstrated no significant association with serum levels of leptin and adiponectin but a negative association with resistin in both genders independent of pubertal stages (r= − 0.329, p<0.0001).
Conclusion:
We conclude that there is no major relationship between OC and metabolism, but we can not exclude minor relations between OC and metabolism. The negative relationship with serum resistin levels might rather point to a link between OC and inflammatory states.
Introduction
Osteocalcin (OC), also known as bone Gla protein (BGP), is one of the very few osteoblast-specific proteins. It is synthesized by mature osteoblasts, odontoblasts and hypertrophic chondrocytes during the process of bone formation. However there was no clear correlation of OC serum concentration to bone mass. OC has several features of a hormone: it is synthesized as a prepromolecule, it is a cell-specific molecule, it is secreted into the circulation, but a receptor has not yet been identified. Posttranslationally, OC undergoes a vitamin K dependent carboxylation. In healthy adults a relatively large fraction (20–30%) of circulating OC is uncarboxylated, and this fraction in children is even larger (up to 60%) [1]. In mice it was shown, that the carboxylated part has a higher affinity to hydroxyapatite of the bone, whereas the uncarboxylated fraction of OC is possibly responsible for putative effects on glucose homeostasis [2].
OC deficient mice develop a phenotype marked by higher bone mass and improved quality of bone function, revealing OC as a determinant for bone formation [3]. Interestingly, these OC deficient mice had higher blood glucose levels, lower insulin levels and they were obese [2]. In normal mice continuous OC administration affected insulin secretion, insulin sensitivity and fat mass [4]. OC acts directly on pancreatic beta cells in culture and in vivo, leading to increased beta cell mass and increased insulin secretion, respectively OC can ameliorate the severity of obesity and type 2 diabetes in mice. In patients with type 2 diabetes several studies showed that OC serum levels were reduced. Children suffering from type 1 diabetes have been reported to have significantly lower OC levels than healthy control subjects at the same pubertal stage [5]. Hence, it appears from these studies that OC is decreased in states of reduced insulin secretion and resulting in hyperglycemia. On the other hand, in a recent study it was shown that OC levels were lower in obese children and that they were related to insulin resistance (IR) and leptin serum concentrations. It was therefore hypothesized that OC could represent a new link between obesity and IR [6]. Accordingly, our studies are aimed to evaluate whether or not OC serum levels are related to parameters of overweight and serum adipokine levels in a cross sectional study in children and adolescents.
Subjects and Methods
Study population
The study population consisted of 497 healthy Caucasian children and adolescents from the Leipzig Schoolchildren Project [7]. Informed consent was obtained from parents and subjects 12 years of age or older. Pubertal stages were determined according to Marshall and Tanner (as described in 1969 and 1970). Subjects were selected and grouped according to gender and pubertal stage; 45–54 individuals for each pubertal stage in each sex (Tanner stages, TS 1–5). We grouped patients according to TS in early pubertal (TS 1 and 2), mid pubertal (TS 3) and late pubertal (TS 4 and 5) groups. Clinical examination and blood withdrawing was performed between 0800 and 1 100 h. The study protocol was approved by the Ethical Committee of the Medical Faculty of the University of Leipzig, Germany, Numbers 781 and 782.
Measurement of anthropometric parameters
Height and weight were determined using precision stadiometers and scales to the nearest of 0.1 cm and 0.1 kg, respectively. For standardization of height and weight, reference percentiles for central Germany were applied [8]. The body mass index (BMI) was standardized referring to national reference data [9]. The waist to hip ratio (WHR) was calculated by measuring the waist at the smallest circumference between hip and chest, and hip circumference at the widest using a nonstretchable metric band.
Underweight, normal weight and overweight were defined as BMI below the 10th, between 10th and 90th and above the 90th percentile, respectively.
Biochemical analyses
Serum was separated by centrifugation and aliquots were stored at − 80°C for biochemical analyses. Levels of OC were determined by the fully automated immunoassay system Advantage (Nichols-Diagnostics). The sensitivity of the assay was calculated to be 0.1 ng/ml. Intra- and inter-assay coefficients of variation (CV) were less than 9.5%.
Leptin levels were measured as described previously [10] [11]. Adiponectin levels were determined by RIA (Linco Research, Inc., St. Louis, MO). The sensitivity of this assay was calculated to be 1 ng/ml. Intra- and inter-assay CVs were less than 14%. Resistin levels were determined by an ELISA (Mediagnost, Reutlingen) with a sensitivity of 12 pg/ml and intra- and inter-assay CVs between 2.4% and 6.8%.
Statistical analysis
Some investigated parameters did not adhere to the normal distribution. Comparison of variables was performed using Mann-Whitney U and Wilcoxon’s signed rank test. Spearman’s nonparametric correlations was utilized to determine relationships between variables. Multiple stepwise linear regression analysis was performed for OC with age, gender, pubertal stage, BMI standard deviation score (SDS), waist to hip ratio (WHR), fat free mass (FFM), leptin, adiponectin and resistin. Age entered the calculation as squared parameter, because the association of age and OC was non-linear. The selection of variables used for the final regression model was obtained by applying backward elimination to the initial multiple regression model. Repeatedly performing backward elimination and removing the least significant parameter in each step, yielded the removal of (in that order): FFM, WHR, BMI-SDS, adiponectin, resistin, leptin, waist circumference and hip circumference. So the risk for a possible multicolinearity was minimized. The threshold for statistical significance was set at p<0.05. Statistical analyses were performed using R (Development Core Team, http://www.R-project.org). The library quantreg version 4.48 by Roger Koenker was used to estimate the age dependent OC centiles as splines with 4 degrees of freedom (http://CRAN.R-project.org/package=quantreg).
If not otherwise mentioned values are given as mean ± standard deviation.
Results
We investigated OC serum levels and different anthropometric parameters in a large and well characterized population of children and adolescents ([Table 1]).
|
Age (years) |
Height (cm) |
Weight (kg) |
BMI-SDS |
WHR* (cm) |
||
|---|---|---|---|---|---|---|
|
Mean±SD |
Mean±SD |
Mean±SD |
Mean±SD |
Mean±SD |
||
|
All values presented as mean and standard deviation. TS1/2 = prepubertal, TS3 = midpubertal, TS4/5 = late pubertal. BMI-SDS: body mass index – standard deviation score. WHR: waist to hip ratio. SD: standard deviation. Note in some categories limited information was present, thus the number of study subjects for the WHR was reduced (*) |
||||||
|
total |
Sum (n=497/*432) |
12.33±2.48 |
155.40±14.56 |
47.55±13.73 |
0.16±1.00 |
0.80±0.05 |
|
Boys (n=247/*221) |
12.77±2.57 |
158.99±15.74 |
50.27±14.77 |
0.12±1.08 |
0.82±0.05 |
|
|
Girls (n=250/*211) |
11.90±2.30 |
151.86±12.31 |
44.87±12.03 |
0.20±0.92 |
0.78±0.05 |
|
|
TS1/2 |
Sum (n=205/*184) |
10.20±1.52 |
143.30±10.64 |
37.60±10.66 |
0.18±1.03 |
0.82±0.04 |
|
Boys (n=103/*94) |
10.39±1.66 |
144.84±11.39 |
39.23±11.72 |
0.22±1.09 |
0.83±0.04 |
|
|
Girls (n=102/*90) |
10.01±1.35 |
141.15±9.47 |
35.95±9.19 |
0.15±0.96 |
0.81±0.04 |
|
|
TS3 |
Sum (n=99/*76) |
12.26±1.47 |
157.90±8.23 |
49.15±10.93 |
0.28±1.04 |
0.80±0.06 |
|
Boys (n=49/*40) |
13.04±1.53 |
161.91±8.15 |
53.79±12.20 |
0.33±1.21 |
0.82±0.06 |
|
|
Girls (n=50/*36) |
11.50±0.89 |
153.96±6.14 |
44.60±6.99 |
0.23±0.83 |
0.78±0.05 |
|
|
TS4/5 |
Sum (n=193/*172) |
14.63±1.45 |
167.30±9.12 |
57.31±10.09 |
0.07±0.95 |
0.78±0.05 |
|
Boys (n=95/*87) |
15.21±0.91 |
172.83±7.52 |
60.43±10.00 |
− 0.10±0.95 |
0.80±0.04 |
|
|
Girls (n=98/*85) |
14.06±1.65 |
161.93±7.12 |
54.28±9.21 |
0.24±0.92 |
0.76±0.05 |
In the total study population circulating OC increased during pubertal development reaching highest values in midpuberty (TS3) ([Fig. 1]). The peak in the cross-sectional 50th centile of OC occured in girls at 11.9 years and hence earlier than in boys with a peak at 13.2 years. However, the 3rd centile showed no distinct peak at all ([Fig. 2]).

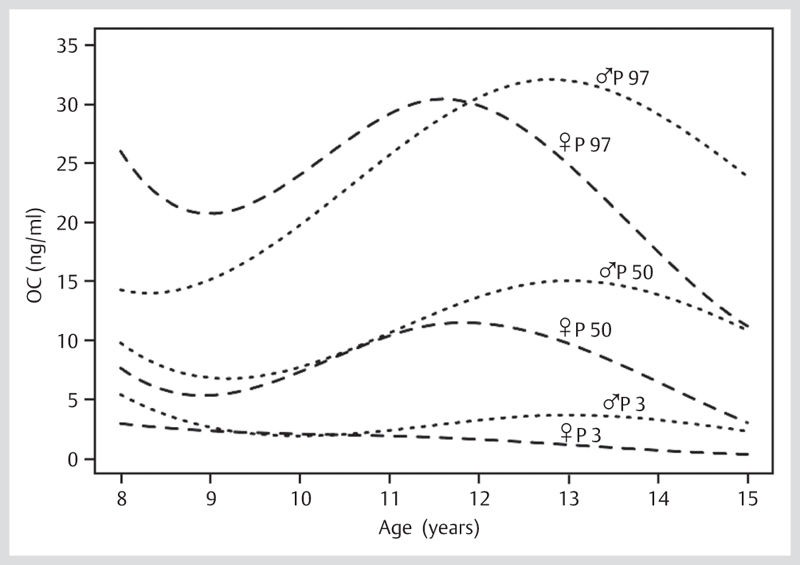
OC levels were significantly higher in boys compared to girls if subjects with pubertal stage 1, 4 and 5 were compared (p<0.05). If boys and girls were separately analyzed, all OC levels were significant different in adjacent TS ([Fig. 1]) with the exception of the comparison between TS 2 and 3. The resulting centiles for OC in boys and girls depending on age are shown in [Fig. 2].
This study did not reveal a strong linkage of OC to overweight/obesity or significantly higher values of OC in lean subjects. Only in early puberty OC levels were significantly lower in overweight (BMI>90th percentile) compared to normal weight peers (BMI 10–90th percentile) (p=0.01). If stratified for gender this was only significant for early pubertal boys (p=0.01) but not for girls ([Fig. 3]). Interestingly, in pubertal stage 3 underweight peers (BMI<10th percentile) demonstrated significant lower levels of OC if compared to the normal weight group. This was obviously detectable for the mid pubertal combined group of boys and girls (p=0.03) as well as for midpubertal boys alone (p=0.04) but not for girls (data not shown).

WHR, a marker for visceral fat in overweight subjects, showed a positive correlation to serum OC levels in the total study population (p<0.0001, r=0.202, n=432). But if stratified for pubertal stage there was only a significant correlation observed between serum OC and WHR in the late pubertal combined group of boys and girls (p<0.0001, r=0.297, n=172) as well as in girls alone (p=0.0008, r=0.358, n=85) but not in boys. As expected, there was a strong relation between WHR and BMI.
The present study demonstrated no significant correlation between serum OC levels and adiponectin or leptin, neither in the total study population nor in the subsets stratified for gender and BMI. As expected leptin serum levels were elevated in overweight children. Only, in late puberty the combined group of boys and girls showed a significant negative correlation between leptin and OC levels (p=0.005, r= − 0.20, n=193).
A significant negative correlation was detectable between OC and resistin serum levels within the total study population (p<0.0001, r= − 0.330, n=186). This correlation was also significant in each pubertal stage, but if stratified by gender it was only significant in early pubertal boys (p=0.008, r= − 0.424, n=38). The serum levels for OC and measured adipokines were summarized in [Table 2] dependent on gender and pubertal stage.
|
Osteocalcin (ng/ml) |
Leptin (ng/ml) |
Resistin* (ng/ml) |
Adiponectin** (ng/ml) |
||
|---|---|---|---|---|---|
|
Mean±SD |
Mean±SD |
Mean±SD |
Mean±SD |
||
|
All values are given as mean and standard deviation. TS1/2 = prepubertal, TS3 = midpubertal, TS4/5 = late pubertal. Note in some categories limited information was present, thus the number of study subjects for resistin (*) and adiponectin (**) serum levels was reduced |
|||||
|
total |
Sum (n=497/*186/**197) |
9.78±6.61 |
6.67±5.89 |
12.77±6.07 |
7.02±2.15 |
|
Boys (n=247/*92/**97) |
10.86±6.44 |
5.05±5.57 |
11.59±6.10 |
6.73±2.20 |
|
|
Girls (n=250/*94/**100) |
8.72±6.61 |
8.29±5.75 |
13.92±5.82 |
7.30±2.06 |
|
|
TS 1/2 |
Sum (n=205/*77/**80) |
9.40±5.30 |
6.42±6.14 |
12.65±7.07 |
7.71±1.92 |
|
Boys (n=103/*38/**40) |
9.96±5.29 |
6.05±6.49 |
11.15±6.88 |
7.96±1.85 |
|
|
Girls (n=102/*39/**40) |
8.83±5.24 |
6.81±5.74 |
14.12±6.94 |
7.47±1.96 |
|
|
TS 3 |
Sum (n=99/*37/**39) |
14.45±7.91 |
7.12±5.42 |
11.20±4.56 |
6.52±2.34 |
|
Boys (n=49/*20/**20) |
14.69±7.48 |
6.27±5.90 |
10.65 ±4.91 |
5.93±2.37 |
|
|
Girls |
(n=50/*17/**19) |
14.22±8.30 |
7.96±4.76 |
11.85±4.01 |
7.14±2.14 |
|
TS 4/5 |
Sum (n=193/*72/**78) |
7.80±5.94 |
6.71±5.83 |
13.70±5.39 |
6.56±2.09 |
|
Boys (n=95/*34/**37) |
9.86±6.24 |
3.34±3.48 |
12.64±5.65 |
5.83±1.80 |
|
|
Girls (n=98/*38/**41) |
5.80±4.87 |
9.97±5.79 |
14.65±4.96 |
7.22±2.11 |
Multiple stepwise linear regression analysis of OC with age, gender, pubertal stage, BMI-SDS, waist circumference, hip circumference, WHR, and adipokines revealed only gender, pubertal stage and age as independent predictors ([Table 3]). Thereby, age entered the calculation as squared parameter, because the association of age and OC was non-linear. This result was found if the whole study cohort but also if subsets of normal weight peers (BMI 10–90th percentile) and overweight peers (BMI > 90th percentile) were analysed.
|
ß coefficient |
standard error |
p-value |
|
|---|---|---|---|
|
TS = Tanner stage. TS1+2 = prepubertal, TS3 = midpubertal, TS4+5 = late pubertal |
|||
|
intercept |
9.524 |
0.644 |
<2e-16 |
|
TS 1+2 |
6.579 |
0.859 |
8.00e-14 |
|
TS 3 |
10.111 |
0.919 |
<2e-16 |
|
TS 4+5 |
4.943 |
1.145 |
1.87e-05 |
|
female |
− 2.544 |
0.501 |
5.20e-07 |
|
age (squared) |
− 0.026 |
0.006 |
7.27e-06 |
Discussion
Our study population demonstrated clearly that OC serum levels were correlated with pubertal development. This correlation is supported by the results of a couple of studies [12] [13], whereas other authors did not find such a link [6] [14]. The detected OC peak levels in TS3 were presumably due to the onset of growth spurt at this pubertal stage. Girls reached the OC peak level at a younger age compared to boys as they enter puberty earlier and onset of growth spurt starts at younger age. OC values were significantly higher in boys compared to girls if subjects with pubertal stage 1, 4 and 5 were compared. For this reason a higher bone mass in boys than in girls could be the explanation [14].
However, there was no major relationship between OC and indicators of body weight, although we can not exclude a minor impact of OC on the very obese phenotype. The significant negative correlation between serum OC levels and indicators of body weight in underweight boys and girls in mid puberty may indicate a later onset of growth spurt in underweight adolescents.
Interestingly and opposite to our expectations, girls with increased WHR have higher OC serum levels than girls with normal WHR. This could be explained by the size of the study subgroups, particularly the low number of obese girls with an increased WHR.
These results are partially in contrast with other studies reporting that obese children had significantly lower OC levels compared with their normal weight peers [15] [16]. These findings in children was underlined by a recent study showing that substantial weight loss was also associated with an increase in OC [6]. Most of these studies that demonstrated a clear relation between OC and obesity investigated a larger number of overweight subjects with a broader range in the distribution of fat mass compared to our cohort. The presented cohort included subjects with a rather normal distribution of BMI and so the number of overweight subjects was distinctly lower than in other studies [6,] [] [15,16].
As adipokines are indicators of adipose tissue mass, we hypothesized to detect an association between OC and serum adipokine levels of adiponectin, leptin and resistin [17]. It is well known that obesity and parameters of the metabolic syndrome are associated with high leptin and low adiponectin serum levels [18]. Leptin produced by the adipose tissue could be the link between obesity and low OC serum levels observed in obesity. Moreover, leptin has important effects on bone metabolism [19] and leptin-deficient ob/ob and leptin-resistant mice have elevated OC serum levels [20]. In our study, only in late puberty, the combined group of boys and girls showed a significant negative correlation between leptin and OC levels. Thus, the relation of OC and leptin appears to be dependent on pubertal status.
In rodent models, it was additionally shown, that OC can influence insulin sensitivity and secretion. Thereby, the impact of OC on insulin sensitivity and visceral fat mass probably depends on an enhanced expression of adiponectin in adipocytes [2] [4]. However, in this study no correlation between OC and adiponectin serum levels was observed.
Resistin initially was studied as a possible link between adiposity and insulin resistance in humans. However, the association between circulating resistin levels and obesity and type 2 diabetes-related phenotypes is unclear [21] [22]. Currently, resistin is considered as a marker of inflammation processes related to obesity [23]. From the teleological point of view, low resistin should favor bone growth in the inflammation free status.
This study has a few potential limitations. First, BMI percentiles were used to classify overweight individuals, but BMI is considered to be only one surrogate marker of fat mass. Second, WHR is an acceptable marker for overweight adolescents, but the information in younger individuals is only very limited and somewhat questionable. Unfortunately, the collected data on fat mass, FFM and homeostasis model assessment (HOMA) was insufficient for gender and Tanner stage specific analyses. Third, a cross sectional study of subjects from a community was conducted and the number of overweight or obese subjects was distinctly lower than the number of lean ones. This “mismatch” between obese and normal weight subjects can cause a potential bias in the analysis.
We conclude that there is no major relationship between OC and metabolism, but we can not exclude minor relations between OC and metabolism. The negative relationship with serum resistin levels might rather point to a link between OC and inflammatory states. Longitudinal studies are needed for a better understanding of putative interactions between OC and fat tissue during the transition from normal weight to obesity.
Conflict of Interest:
None.
-
References
- 1 van Summeren M, Braam L, Noirt F et al. Pronounced elevation of undercarboxylated osteocalcin in healthy children. Pediatr Res 2007; 61: 366-370
- 2 Lee NK, Sowa H, Hinoi E et al. Endocrine regulation of energy metabolism by the skeleton. Cell 2007; 130: 456-469
- 3 Ducy P, Desbois C, Boyce B et al. Increased bone formation in osteocalcin-deficient mice. Nature 1996; 382: 448-452
- 4 Ferron M, Hinoi E, Karsenty G et al. Osteocalcin differentially regulates beta cell and adipocyte gene expression and affects the development of metabolic diseases in wild-type mice. Proc Natl Acad Sci USA 2008; 105: 5266-5270
- 5 Brandao FR, Vicente EJ, Daltro CH et al. Bone metabolism is linked to disease duration and metabolic control in type 1 diabetes mellitus. Diabetes Res Clin Pract 2007; 78: 334-339
- 6 Reinehr T, Roth CL. A new link between skeleton, obesity and insulin resistance: relationships between osteocalcin, leptin and insulin resistance in obese children before and after weight loss. Int J Obes (Lond) 2010; 34: 852-858
- 7 Reich A, Muller G, Gelbrich G et al. Obesity and blood pressure – results from the examination of 2 365 schoolchildren in Germany. Int J Obes Relat Metab Disord 2003; 27: 1459-1464
- 8 Kiess W, Gausche R, Keller A et al. Computer-guided population-based screening system for growth disorders (CrescNet) and on-line generation of normative data for growth and development. Horm Res 2001; 56 (Suppl. 01) 59-66
- 9 Kromeyer-Hauschild K, Wabitsch M, Kunze D et al. Percentiles of body mass index in children and adolescents evaluated from different regional German studies. Monatsschrift Kinderheilkunde 2001; 149: 807-818
- 10 Kratzsch J, Berthold A, Lammert A et al. A rapid, quantitative immunofunctional assay for measuring human leptin. Horm Res 2002; 57: 127-132
- 11 Kratzsch J, Lammert A, Bottner A et al. Circulating soluble leptin receptor and free leptin index during childhood, puberty, and adolescence. J Clin Endocrinol Metab 2002; 87: 4587-4594
- 12 Gundberg CM, Lian JB, Gallop PM. Measurements of gamma-carboxyglutamate and circulating osteocalcin in normal children and adults. Clin Chim Acta 1983; 128: 1-8
- 13 Yilmaz D, Ersoy B, Bilgin E et al. Bone mineral density in girls and boys at different pubertal stages: relation with gonadal steroids, bone formation markers, and growth parameters. J Bone Miner Metab 2005; 23: 476-482
- 14 Hui SL, Dimeglio LA, Longcope C et al. Difference in bone mass between black and white American children: attributable to body build, sex hormone levels, or bone turnover?. J Clin Endocrinol Metab 2003; 88: 642-649
- 15 Bini V, Igli Baroncelli G, Papi F et al. Relationships of serum leptin levels with biochemical markers of bone turnover and with growth factors in normal weight and overweight children. Horm Res 2004; 61: 170-175
- 16 Zamboni G, Soffiati M, Giavarina D et al. Mineral metabolism in obese children. Acta Paediatr Scand 1988; 77: 741-746
- 17 Koerner A, Kratzsch J, Kiess W. Adipocytokines: leptin – the classical, resistin – the controversical, adiponectin – the promising, and more to come. Best Pract Res Clin Endocrinol Metab 2005; 19: 525-546
- 18 Bottner A, Kratzsch J, Muller G et al. Gender differences of adiponectin levels develop during the progression of puberty and are related to serum androgen levels. J Clin Endocrinol Metab 2004; 89: 4053-4061
- 19 Reid IR, Cornish J, Baldock PA. Nutrition-related peptides and bone homeostasis. J Bone Miner Res 2006; 21: 495-500
- 20 Goldstone AP, Mercer JG, Gunn I et al. Leptin interacts with glucagon-like peptide-1 neurons to reduce food intake and body weight in rodents. FEBS Lett 1997; 415: 134-138
- 21 Azuma K, Katsukawa F, Oguchi S et al. Correlation between serum resistin level and adiposity in obese individuals. Obes Res 2003; 11: 997-1001
- 22 Silha JV, Krsek M, Skrha JV et al. Plasma resistin, adiponectin and leptin levels in lean and obese subjects: correlations with insulin resistance. Eur J Endocrinol 2003; 149: 331-335
- 23 Filkova M, Haluzik M, Gay S et al. The role of resistin as a regulator of inflammation: Implications for various human pathologies. Clin Immunol 2009; 133: 157-170
Correspondence
-
References
- 1 van Summeren M, Braam L, Noirt F et al. Pronounced elevation of undercarboxylated osteocalcin in healthy children. Pediatr Res 2007; 61: 366-370
- 2 Lee NK, Sowa H, Hinoi E et al. Endocrine regulation of energy metabolism by the skeleton. Cell 2007; 130: 456-469
- 3 Ducy P, Desbois C, Boyce B et al. Increased bone formation in osteocalcin-deficient mice. Nature 1996; 382: 448-452
- 4 Ferron M, Hinoi E, Karsenty G et al. Osteocalcin differentially regulates beta cell and adipocyte gene expression and affects the development of metabolic diseases in wild-type mice. Proc Natl Acad Sci USA 2008; 105: 5266-5270
- 5 Brandao FR, Vicente EJ, Daltro CH et al. Bone metabolism is linked to disease duration and metabolic control in type 1 diabetes mellitus. Diabetes Res Clin Pract 2007; 78: 334-339
- 6 Reinehr T, Roth CL. A new link between skeleton, obesity and insulin resistance: relationships between osteocalcin, leptin and insulin resistance in obese children before and after weight loss. Int J Obes (Lond) 2010; 34: 852-858
- 7 Reich A, Muller G, Gelbrich G et al. Obesity and blood pressure – results from the examination of 2 365 schoolchildren in Germany. Int J Obes Relat Metab Disord 2003; 27: 1459-1464
- 8 Kiess W, Gausche R, Keller A et al. Computer-guided population-based screening system for growth disorders (CrescNet) and on-line generation of normative data for growth and development. Horm Res 2001; 56 (Suppl. 01) 59-66
- 9 Kromeyer-Hauschild K, Wabitsch M, Kunze D et al. Percentiles of body mass index in children and adolescents evaluated from different regional German studies. Monatsschrift Kinderheilkunde 2001; 149: 807-818
- 10 Kratzsch J, Berthold A, Lammert A et al. A rapid, quantitative immunofunctional assay for measuring human leptin. Horm Res 2002; 57: 127-132
- 11 Kratzsch J, Lammert A, Bottner A et al. Circulating soluble leptin receptor and free leptin index during childhood, puberty, and adolescence. J Clin Endocrinol Metab 2002; 87: 4587-4594
- 12 Gundberg CM, Lian JB, Gallop PM. Measurements of gamma-carboxyglutamate and circulating osteocalcin in normal children and adults. Clin Chim Acta 1983; 128: 1-8
- 13 Yilmaz D, Ersoy B, Bilgin E et al. Bone mineral density in girls and boys at different pubertal stages: relation with gonadal steroids, bone formation markers, and growth parameters. J Bone Miner Metab 2005; 23: 476-482
- 14 Hui SL, Dimeglio LA, Longcope C et al. Difference in bone mass between black and white American children: attributable to body build, sex hormone levels, or bone turnover?. J Clin Endocrinol Metab 2003; 88: 642-649
- 15 Bini V, Igli Baroncelli G, Papi F et al. Relationships of serum leptin levels with biochemical markers of bone turnover and with growth factors in normal weight and overweight children. Horm Res 2004; 61: 170-175
- 16 Zamboni G, Soffiati M, Giavarina D et al. Mineral metabolism in obese children. Acta Paediatr Scand 1988; 77: 741-746
- 17 Koerner A, Kratzsch J, Kiess W. Adipocytokines: leptin – the classical, resistin – the controversical, adiponectin – the promising, and more to come. Best Pract Res Clin Endocrinol Metab 2005; 19: 525-546
- 18 Bottner A, Kratzsch J, Muller G et al. Gender differences of adiponectin levels develop during the progression of puberty and are related to serum androgen levels. J Clin Endocrinol Metab 2004; 89: 4053-4061
- 19 Reid IR, Cornish J, Baldock PA. Nutrition-related peptides and bone homeostasis. J Bone Miner Res 2006; 21: 495-500
- 20 Goldstone AP, Mercer JG, Gunn I et al. Leptin interacts with glucagon-like peptide-1 neurons to reduce food intake and body weight in rodents. FEBS Lett 1997; 415: 134-138
- 21 Azuma K, Katsukawa F, Oguchi S et al. Correlation between serum resistin level and adiposity in obese individuals. Obes Res 2003; 11: 997-1001
- 22 Silha JV, Krsek M, Skrha JV et al. Plasma resistin, adiponectin and leptin levels in lean and obese subjects: correlations with insulin resistance. Eur J Endocrinol 2003; 149: 331-335
- 23 Filkova M, Haluzik M, Gay S et al. The role of resistin as a regulator of inflammation: Implications for various human pathologies. Clin Immunol 2009; 133: 157-170