
Subscribe to RSS
DOI: 10.1055/s-0029-1214707
© Georg Thieme Verlag KG Stuttgart · New York
Secondary sclerosing cholangitis after chemotherapy with bevacizumab and paclitaxel
H. KulaksizMD
Department of Internal Medicine I
University of
Ulm
Albert-Einstein-Allee 23
89081
Ulm
Germany
Fax: +49-731-50045226
Email: hasan.kulaksiz@uniklinik-ulm.de
Publication History
Publication Date:
19 June 2009 (online)

A 59-year-old woman was referred to our hospital by her gynaecologist because of progressive jaundice. She had been diagnosed as having left-sided breast cancer 18 months ago. Two months before admission, she had started chemotherapy with intravenous paclitaxel (90 mg/m2) and bevacizumab (10 mg/kg). [Fig. 1] summarizes the patient’s treatments and results of the liver function tests (LFTs).
On admission, blood tests revealed markedly elevated LFTs in a cholestatic pattern and raised levels of C-reactive protein. There was no evidence of underlying viral, metabolic, or autoimmune liver disease, and antibiotic therapy was initiated. A contrast-enhanced abdominal ultrasound and magnetic resonance (MR) scan revealed remarkably normal liver parenchyma ([Fig. 2]) but moderate intrahepatic cholestasis. Subsequently, endoscopic retrograde cholangioscopy (ERCP) was performed, which showed a completely stenosed, but negotiable, common bile duct (CBD) with prestenotic intrahepatic duct dilatation ([Fig. 3]). On the basis of the above findings, secondary sclerosing cholangitis (SSC) was diagnosed. Following the antibiotic therapy and endoscopic intervention, there was a substantial decrease in cholestasis ([Fig. 1]).

Fig. 1 Treatments received and liver function test (LFT) results before and after the patient’s admission. The previous chemotherapy treatments had not led to any changes in the LFTs. However, following initiation of chemotherapy consisting of bevacizumab and paclitaxel there was a dramatic increase in the LFTs. Antibiotic therapy and endoscopic retrograde cholangioscopy (ERCP) led to a substantial decrease in cholestatic parameters (alkaline phosphatase (AP)/gammaglutamyltranspeptidase/bilirubin) and aspartate aminotransferase (AST)/alanine aminotransferase (ALT). CHT, chemotherapy; AC, cyclophosphamide/doxorubicin.

Fig. 2 Diagnostic imaging of liver. a Contrast-enhanced ultrasound study of the liver showing normal appearing parenchyma with no signs of malignant infiltration of the liver. b T2-weighted magnetic resonance scan confirmed normal liver parenchyma with no evidence of compression of the common bile duct by intra-abdominal tumor. Moderate, centrally localized intrahepatic cholestasis was apparent (arrow). Note the perihepatic ascites.

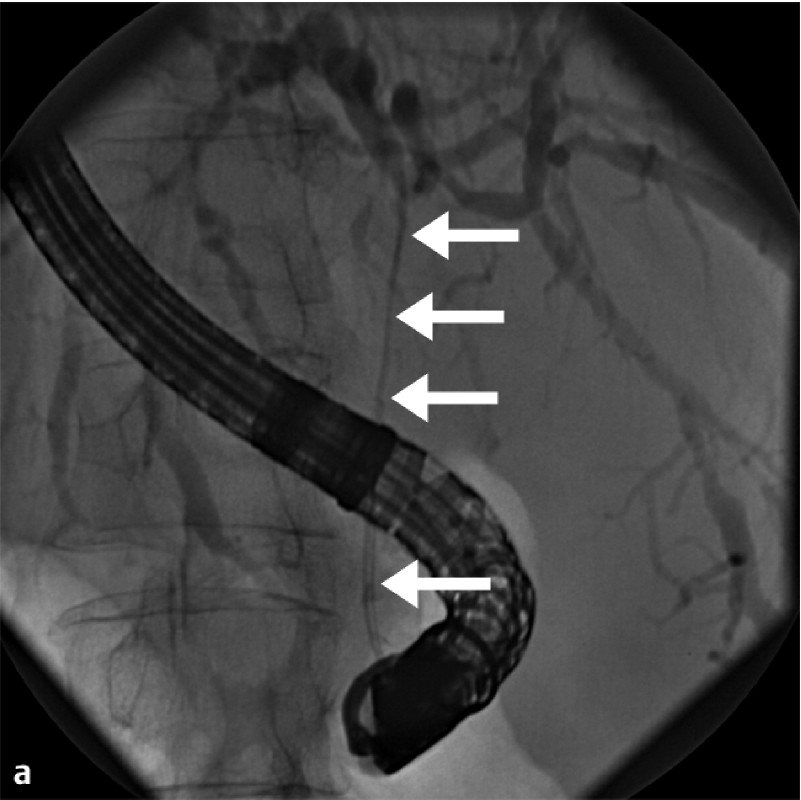

Fig. 3 Endoscopic retrograde cholangioscopy. a Nearly complete stenosis of the common bile duct (arrow), including the hilar region. The intrahepatic ducts are prestenotically dilated with no signs of strictures. b Negotiating the common bile duct stenosis with a wire.
SSC is a rare disease, characterized by bile duct inflammation, fibrosis, and strictures [1] [2]. It was recently reported that treatment with intravenous bevacizumab caused SSC in a patient with colorectal carcinoma after surgical treatment of liver metastases [3]. In our case, the time course of the disease suggests a link with the chemotherapy with paclitaxel and bevacizumab. Bevacizumab seemed more likely to be the causal agent, because the patient had previously well tolerated a synthetic analog of paclitaxel. Ischemic cholangitis – a known cause of SSC [4] – may be induced by the prothrombotic antibody bevacizumab by clot formation in the arterioles supplying the bile ducts. This may explain why in our patient the CBD and not the intrahepatic bile ducts was selectively affected, since both compartments are supplied by distinct vessels. The development of SSC in a previously normal liver underlines the importance of being aware of the hepatic adverse effects of bevacizumab.
Endoscopy_UCTN_Code_CCL_1AZ_2AJ
#References
- 1 Abdalian R, Heathcote E J. Sclerosing cholangitis: a focus on secondary causes. Hepatology. 2006; 44 1063-1074
- 2 Kulaksiz H, Heuberger D, Engler S. et al . Poor outcome in progressive sclerosing cholangitis after septic shock. Endoscopy. 2008; 40 214-218
- 3 Delis S, Triantopoulou C, Bakoyiannis A. et al . Sclerosing cholangitis in the era of target chemotherapy: a possible anti-VEGF effect. Dig Liver Dis. 2009; 41 72-77
- 4 Batts K P. Ischemic cholangitis. Mayo Clin Proc. 1998; 73 380-385
H. KulaksizMD
Department of Internal Medicine I
University of
Ulm
Albert-Einstein-Allee 23
89081
Ulm
Germany
Fax: +49-731-50045226
Email: hasan.kulaksiz@uniklinik-ulm.de
References
- 1 Abdalian R, Heathcote E J. Sclerosing cholangitis: a focus on secondary causes. Hepatology. 2006; 44 1063-1074
- 2 Kulaksiz H, Heuberger D, Engler S. et al . Poor outcome in progressive sclerosing cholangitis after septic shock. Endoscopy. 2008; 40 214-218
- 3 Delis S, Triantopoulou C, Bakoyiannis A. et al . Sclerosing cholangitis in the era of target chemotherapy: a possible anti-VEGF effect. Dig Liver Dis. 2009; 41 72-77
- 4 Batts K P. Ischemic cholangitis. Mayo Clin Proc. 1998; 73 380-385
H. KulaksizMD
Department of Internal Medicine I
University of
Ulm
Albert-Einstein-Allee 23
89081
Ulm
Germany
Fax: +49-731-50045226
Email: hasan.kulaksiz@uniklinik-ulm.de
Fig. 1 Treatments received and liver function test (LFT) results before and after the patient’s admission. The previous chemotherapy treatments had not led to any changes in the LFTs. However, following initiation of chemotherapy consisting of bevacizumab and paclitaxel there was a dramatic increase in the LFTs. Antibiotic therapy and endoscopic retrograde cholangioscopy (ERCP) led to a substantial decrease in cholestatic parameters (alkaline phosphatase (AP)/gammaglutamyltranspeptidase/bilirubin) and aspartate aminotransferase (AST)/alanine aminotransferase (ALT). CHT, chemotherapy; AC, cyclophosphamide/doxorubicin.
Fig. 2 Diagnostic imaging of liver. a Contrast-enhanced ultrasound study of the liver showing normal appearing parenchyma with no signs of malignant infiltration of the liver. b T2-weighted magnetic resonance scan confirmed normal liver parenchyma with no evidence of compression of the common bile duct by intra-abdominal tumor. Moderate, centrally localized intrahepatic cholestasis was apparent (arrow). Note the perihepatic ascites.
Fig. 3 Endoscopic retrograde cholangioscopy. a Nearly complete stenosis of the common bile duct (arrow), including the hilar region. The intrahepatic ducts are prestenotically dilated with no signs of strictures. b Negotiating the common bile duct stenosis with a wire.