
Subscribe to RSS
DOI: 10.1055/a-2225-5570
Simple use of Y-connector for proper positioning and contrast aspiration in biliary metal stent placement

Endoscopic biliary drainage for unresectable malignant hilar biliary obstruction often requires multiple metal stents, and stent-in-stent placement is an effective drainage method [1] [2]. Although multiple stent placement requires more cholangiograms for proper positioning, post-endoscopic retrograde cholangiopancreatography (ERCP) cholangitis remains a concern. Moreover, the over-injection of contrast medium and residual contrast medium increase post-ERCP cholangitis [3] [4] [5]. To overcome these issues, we introduced a simple method using a Y-connector attached to an existing metal stent ([Fig. 1]).
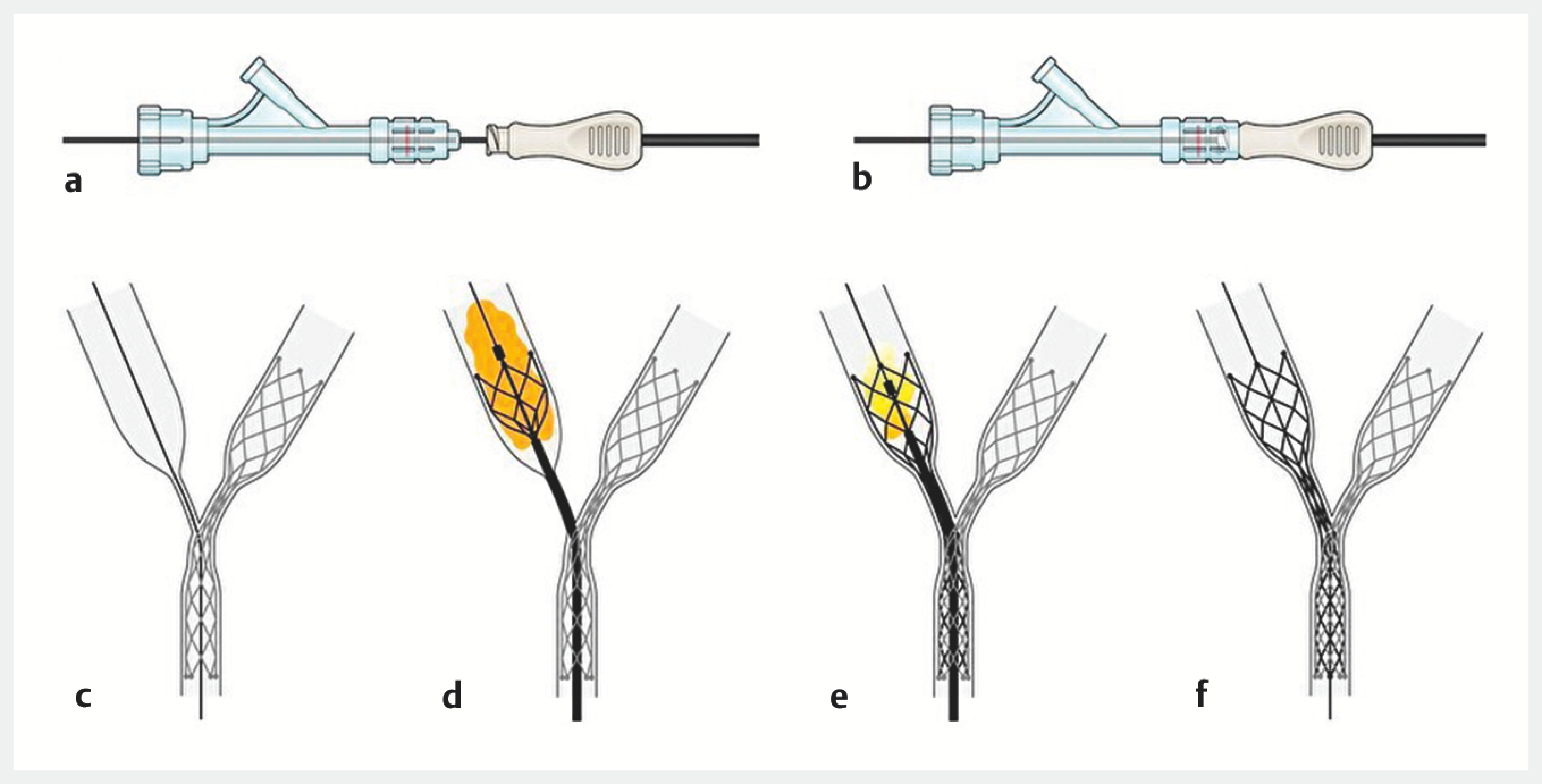
A 70-year-old woman undergoing chemotherapy for intrahepatic cholangiocarcinoma after a previous cholecystitis-associated endoscopic ultrasound-guided gallbladder drainage presented with obstructive jaundice for hilar biliary obstruction. Enhanced computed tomography revealed bilateral intra-bile duct dilation ([Fig. 2]). Stent-in-stent placement was performed. The first metal stent was placed, and a guidewire was inserted through the mesh gap into the bile duct, where the second stent placement was intended. By this point, most of the contrast medium had leaked out, making the length of the stenosis and the target placement position difficult to determine ([Fig. 3] a,b). A Y-connector (Access-9TM, Hemostasis Valve; SHEEN MAN Co., Ltd., Osaka, Japan) was attached to the proximal end of the guidewire lumen of the second stent device. The stent was inserted into the bile duct through a guidewire using a Y-connector. Because contrast using the Y-connector enabled visualization of the stenosis, it was easy to determine the position of the stent ([Fig. 3] c). Furthermore, to prevent postoperative cholangitis after deployment, the remaining contrast medium could be aspirated easily without switching to a catheter ([Fig. 3] d,e) ([Video 1]). No post-ERCP cholangitis or elevated hepatobiliary enzyme levels were observed in this patient.
The combination of the stent device and Y-connector is a convenient and an efficacious method for confirming the stent position and preventing post-ERCP cholangitis.


Quality:
Endoscopy_UCTN_Code_TTT_1AR_2AZ
E-Videos is an open access online section of the journal Endoscopy, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high-quality video and are published with a Creative Commons CC-BY license. Endoscopy E-Videos qualify for HINARI discounts and waivers and eligibility is automatically checked during the submission process. We grant 100% waivers to articles whose corresponding authors are based in Group A countries and 50% waivers to those who are based in Group B countries as classified by Research4Life (see: https://www.research4life.org/access/eligibility/).
This section has its own submission website athttps://mc.manuscriptcentral.com/e-videos.
#
Conflict of Interest
The authors declare that they have no conflict of interest.
Acknowledgement
Division of Innovative Medicine for Hepatobiliary and Pancreatology is an endowment department, supported with an unrestricted grant from HITO Medical Center. We would like to thank Editage (www.editage.jp) for English language editing.
-
References
- 1 Kaneko J, Yamada T, Fukita K. et al. Endoscopic four-branched stent-in-stent deployment of self-expandable metal stents in malignant hilar biliary obstruction. 2022; 54: E482-E483
- 2 Koshitani T, Nakagawa S, Konaka Y. et al. Endoscopic deployment of multiple (≥ 3) metal stents for unresectable malignant hilar biliary strictures. Endosc Int Open 2019; 7: E672-E677
- 3 Wan X, Chen S, Zhao Q. et al. The efficacy of temporary placement of nasobiliary drainage following endoscopic metal stenting to prevent post-ERCP cholangitis in patients with cholangiocarcinoma. Saudi J Gastroenterol 2018; 24: 348-354
- 4 Lee TH, Moon JH, Park SH. Biliary stenting for hilar malignant biliary obstruction. Dig Endosc 2020; 32: 275-286
- 5 Kawakami H, Itoi T, Kuwatani M. et al. Technical tips and troubleshooting of endoscopic biliary drainage for unresectable malignant hilar biliary obstruction. J Hepatobiliary Pancreat Sci 2015; 22: E12-E21
Correspondence
Publication History
Article published online:
09 January 2024
© 2024. The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Kaneko J, Yamada T, Fukita K. et al. Endoscopic four-branched stent-in-stent deployment of self-expandable metal stents in malignant hilar biliary obstruction. 2022; 54: E482-E483
- 2 Koshitani T, Nakagawa S, Konaka Y. et al. Endoscopic deployment of multiple (≥ 3) metal stents for unresectable malignant hilar biliary strictures. Endosc Int Open 2019; 7: E672-E677
- 3 Wan X, Chen S, Zhao Q. et al. The efficacy of temporary placement of nasobiliary drainage following endoscopic metal stenting to prevent post-ERCP cholangitis in patients with cholangiocarcinoma. Saudi J Gastroenterol 2018; 24: 348-354
- 4 Lee TH, Moon JH, Park SH. Biliary stenting for hilar malignant biliary obstruction. Dig Endosc 2020; 32: 275-286
- 5 Kawakami H, Itoi T, Kuwatani M. et al. Technical tips and troubleshooting of endoscopic biliary drainage for unresectable malignant hilar biliary obstruction. J Hepatobiliary Pancreat Sci 2015; 22: E12-E21