

Subscribe to RSS
DOI: 10.1055/a-1934-8404
Improving Asthma Care Documentation with a Digital Tool–Experience in a Pediatric Institution
Authors
Funding None.

Abstract
Background Asthma affects approximately 10% of Australian children. Electronic medical record (EMR) systems and clinical decision support initiatives have been shown to improve the delivery of asthma care. Our institution implemented an EMR-based asthma “hub,” which collates asthma-related information to a central location within a patient's record, provides a template to collect relevant clinical information, allows clinicians to evaluate a patient's history and presentation in a systematic manner and prompts relevant actions.
Objective The aim of the study is to measure year-on-year improvement in asthma-related documentation and provide a key gold-standard aspects of asthma management after the introduction of an EMR asthma “hub” tool in the outpatient setting.
Methods The asthma “hub” was introduced in November 2020. A chart review was conducted of all patients who attended the Complex Asthma Clinic between January-April 2020 and January-April 2021. The provision and presence of documentation of core aspects of asthma care were described in percentages and comparisons of pre- and post-introduction of the asthma “hub” were assessed.
Results There was a significant increase in the documentation of asthma triggers, including smoking/smoker exposure, (47.5–92.6%, p <0.001), current asthma action plans (70.4–86.3%, p = 0.02), and severity scores (46.3–81%, p <0.001) post the introduction of the asthma “hub.” There was no significant difference in documentation of reliever (as required) or regular preventer medications.
Conclusion An evidence-based EMR intervention improved the documentation and provision of aspects of asthma care in an outpatient clinic setting at a tertiary pediatric hospital, suggesting replication in the inpatient and emergency settings would be worthwhile. Further research is required to understand the tool's impact on clinical outcomes and on clinical efficiency and workflow.
Background and Significance
Asthma is a common childhood illness affecting approximately 10% of all Australian children,[1] with recent data demonstrating that it is the leading cause of disease amongst Australian children aged 5 to 14 years.[2] While asthma in Australia is primarily managed in a primary health care setting, many children require hospital care for acute or long-term management of moderate to severe disease.[1]
In the hospital setting, childhood asthma is managed in the outpatient, inpatient, and emergency settings. Across these encounters, routinely addressing key aspects of asthma management has been shown to improve clinical outcomes.[3] [4] [5] [6] These include assessment of asthma triggers, evaluation of severity and control (including use of age-appropriate standardized asthma severity scores – Asthma Control Test [ACT], Asthma Control Questionnaire [ACQ] or the Test of Respiratory and Asthma Control in Kids [TRACK]), inhaler technique, appropriate medication dosing and adherence, asthma education and the provision of an asthma action plan, which forms the foundation of the Australian National Asthma Guidelines.[3] [4] [5] [7]
Although these core aspects of asthma care are well established and widely accepted, they are often either missed or duplicated during hospital-based patient consultations. An example of these gaps in routine asthma care is poor assessment and recognition of asthma control, which results in the under-recognition of suboptimal control.[8] [9] [10] Furthermore, a recent Australian survey showed that one in three children with asthma (aged between 0 and 14) did not have an up-to-date asthma action plan,[11] despite it being shown to be associated with both reduction in asthma-related acute presentations to hospital and overall risk of asthma-related morbidity.[6] [7]
Many hospitals have adopted targeted clinical decision support initiatives to address some of these gaps, which have been shown to improve the delivery of asthma care.[12] [13] [14] [15] However, there remains ongoing gaps in care affecting the accuracy of patient information collected as well as the efficiency of clinical workflow, which in turn can have a detrimental impact on clinical decision making and outcomes. This is primarily due to the bespoke nature of previously developed electronic tools, without the integration with a wider electronic medical record (EMR), which therefore does not allow the possibility of harnessing efficiency savings.
Our institution, The Royal Children's Hospital Melbourne (RCH), has an organization wide EMR system (Epic Systems, Verona, WI) which was introduced in 2016. However, like many EMR systems there was no dedicated asthma-related EMR tool or decision support system to aid clinicians, with most asthma documentation and care decisions completed without templates in an ad hoc manner as per clinician preference.
To address this, an integrated EMR-based asthma “hub” tool was developed for initial use in the outpatient clinic setting.
Objectives
The objective of this study was to measure year-on-year improvement in asthma-related documentation and provide a key gold-standard aspects of asthma management after the introduction of an EMR asthma “hub” tool in the outpatient setting. Specific focus was on key aspects of asthma management that have been demonstrated to improve clinical outcomes, such as documentation of asthma triggers, including smoke exposure, use of asthma severity scores, and provision of a new or updated asthma action plan.
Methods
Setting and Inclusion Criteria
RCH is a tertiary pediatric institution that has approximately 45,000 outpatient appointments per year. The complex asthma ambulatory care clinic is specifically for patients with moderate to severe asthma, who have multiple complex risk factors making them prone to high risk for repeat asthma exacerbations, failure of treatment, or admission to hospital. The clinic sees approximately 480 patients per year. This cohort was selected for evaluation as they are the group who would benefit the most from a pilot intervention that addressed routine provision of care for asthma.
A single-center retrospective chart review was conducted at RCH and included all patients who attended the outpatient Complex Asthma Clinic between January to April 2020 and January to April 2021 following the introduction of the asthma “hub” in November 2020. The same timeframe was compared between 2020 and 2021 to account for potential seasonal variation.
Asthma Hub Design
While the asthma “hub” has a bespoke design customized to suit organization-specific workflows, it harnesses native EMR functionality and tools for build. It has been designed to sit within the clinic visit workflow for clinicians, with content terminology that suits the Australian clinical context ([Figs. 1] and [2]).
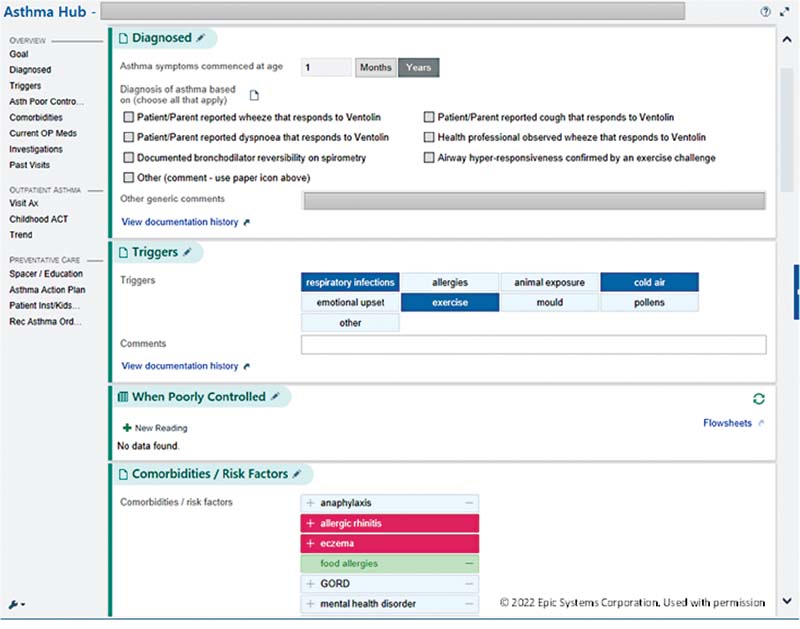

The hub has three main features ([Table 1]):
-
Collating relevant asthma-related clinical information from across a patient's chart into a single location for ease of review and evaluation.
-
Provision of a standardized template to document key asthma-related information that can either carry across all patient encounters (e.g., asthma triggers) or are specific to that patient visit (e.g., asthma assessment score).
-
Provision for clinicians to act on this information via various mechanisms within the same workflow (e.g., develop/print asthma action plan or order community-based education follow-up visits).
The hub was collaboratively developed over a 3 month period by a “hub working group” comprising clinicians working in the complex asthma clinic and health informaticians. Content development was established using clinical practice guidelines and stakeholder inputs and consensus from the broader organizational asthma working group. This was then translated into an informatics tool by informaticians. Three rounds of user acceptance testing (UAT) were conducted by the hub working group to ensure that the content matched organizational workflow and practice, and the tool was as efficient as it could be with user experience as streamlined as possible ([Fig. 3]).

Statistical Consideration
Presence of documentation of each aspect of asthma care was reviewed and described in percentages. Fisher's exact test was used to compare pre and post intervention data, with p <0.05 considered statistically significant.
Results
A total of 161 cases were reviewed, with 80 and 81 patients in the pre- and post-asthma “hub” groups, respectively.
After the introduction of the asthma “hub” there was a significant increase in the documentation of asthma triggers (e.g., smoking/smoker exposure), (47.5–92.6%, p <0.001), current asthma action plans (70.4–86.3%, p = 0.02), and severity scores (46.3–81%, p < 0.001). There was no significant difference in the documentation of reliever (as required) or regular preventer medications (93.8–95.1%, p = 0.75).
Evaluation of patients' post-introduction of the asthma “hub” demonstrated documentation of inhaler and spacer technique assessments in 37.5% of patients, and documentation of the provision of asthma education via online links and videos in 25.0%. There was no documentation of these metrics in any cases prior to the introduction of asthma “hub.”
Discussion
This study demonstrated that an EMR-based asthma “hub” is effective at increasing the provision of key aspects of routine asthma management and documentation in a systematic manner. This supports previous studies demonstrating the utility of EMR-based asthma tools in influencing the provision of and improving the quality of asthma care.[12] [13] [14] [15] [16] [17]
Increasing evaluation of core aspects of asthma management and documentation directly improves clinical outcomes.[4] The recognition of asthma triggers, including allergens and tobacco smoke exposure can reduce disease severity and specifically avoiding tobacco smoke has been demonstrated to reduce early lung function decline.[18] [19] Further to this, the use of severity scores and asthma action plans have been shown to reduce associated morbidity and the use of acute and specialist health care services.[8] [9] [10]
The implementation of the asthma “hub” significantly increased these key elements – namely recognition and documentation of asthma triggers, including smoke exposure, use of asthma severity scores, and provision of a new or updated asthma action plan. This is likely due to a systematic standardized proforma which provided key information within the clinician's workflow and acted as an aid to prompt clinicians to ask or update key elements of asthma care.
In contrast, this study found no significant difference in documentation of reliever (as required) or regular preventer medications despite the introduction of the asthma “hub.” This is likely due the need of prescriptions for medications, which already required an active ordering process within an EMR setting. Thus, the hub served to streamline and collate a list of patient medications without the clinician needing to find this in other parts of the patient's medical record – but the overall documentation rates did not improve.
Importantly, the “hub” also enabled evaluation of the provision of asthma care by facilitating aspects of management that had not previously been routinely documented. There was minimal information or documentation of clinical items such as assessments of spacer and inhaler technique and the provision of asthma education through online and print resources prior to the introduction of the “hub,” which therefore made direct clinical impact difficult to measure. Although there was improved documentation after the “hub,” this provides an opportunity to engage other informatics solutions such as predictive ordering or clinical decision support tools to prompt clinicians and enhance uptake of these important asthma preventative care strategies.
Overall, the study highlights the importance and impact of the basic foundational benefit of using the EMR to provide appropriate and relevant data within a clinician's workflow. While additional informatics solutions and tools can assist and enhance asthma care, they rely first on appropriate and accurate data to be available for evaluation and analysis.
Further evaluation of impacts of this informatic solution on specific clinical outcomes including number of exacerbations and hospital attendances, would provide more comprehensive evaluation of its clinical utility. Evaluation of user experience will also allow understanding of the intervention on clinic efficiency and workflow. A more comprehensive understanding of the benefits, practicalities, and acceptability will enable planning for potential rollout into other settings such as inpatient and emergency settings, as well as how to synergize the “hub” with other potential interventions.
Limitations
The single center study was conducted at a tertiary level pediatric hospital and therefore conclusions may not be applicable to different environments where there are different resource availabilities. The study was conducted in a single asthma clinic with highly repetitive workflows. Application in other clinics where workflows are more sporadic may impact the effectiveness.
The tool was introduced during the COVID pandemic period which significantly affected the mode of care – culminating in a significant shift to telehealth after March 2020 due to COVID restrictions. Although this may have affected clinician–patient interaction, the study measures the impact of documentation rather than clinical outcomes or improvement, which is unlikely to be significantly altered by COVID-related changes.
Conclusion
The use of an EMR-based asthma “hub” improved the documentation and provision of asthma care in a pediatric outpatient setting, particularly in key areas which have been shown to improve clinical outcomes. Further evaluation of potential improvement in specific clinical outcomes, including impact on emergency attendance and admission frequency, and user experience will influence expansion of the “hub” into inpatient and emergency settings.
Clinical Relevance Statement
This study demonstrated that the use of an EMR tool, the asthma “hub,” in an outpatient setting, positively impacts core aspects of asthma management by boosting clinical provision of asthma care through improved documentation.
Multiple Choice Questions
-
This study demonstrated a dedicated EMR-based asthma tool, the asthma “hub,” can support and improve asthma management when using standardized data elements. Which of the following elements were not included in the asthma “hub”?
-
Co-morbidities.
-
Detailed family history of asthma.
-
Asthma-related investigations.
-
Influenza vaccination status.
Correct Answer: The correct option is b. While a family history of asthma predicts an increased risk of developing the disease, a family history of asthma has been demonstrated to have a low positive predictive value and has a limited role in guiding asthma management. The remainder of the options were elements included in the asthma “hub.”
-
-
Which of the following was the main feature of the EMR-based asthma “hub” assessed in this current study?
-
Making available and summarizing asthma relevant clinical information for general practitioners and community health care providers.
-
Providing asthma medication recommendations based on relevant clinical information available.
-
Providing links to relevant clinical asthma guidelines.
-
Allowing clinicians to evaluate and act on the collated relevant asthma information from a patient's electronic medical record.
Correct Answer: The correct option is d. The other options were not features of the current study but are important features to consider for future development of the asthma “hub.”
-
Conflict of Interest
None declared.
Acknowledgments
The authors thank Dr. Shivanthan Shantikumar for contributions to the manuscript.
Protection of Human and Animal Subjects
The study was approved by the RCH Human Research and Ethics Committee (Ethics approval number QA/69208/RCHM-2020).
-
References
- 1 Australian Institute of Health and Welfare (AIHW) Cat No. . ACM 33 Asthma; 2020
- 2 Asher I, Pearce N. Global burden of asthma among children. Int J Tuberc Lung Dis 2014; 18 (11) 1269-1278
- 3 National Asthma Council Australia. . Australian Asthma Handbook – Management in Children. Accessed December 15, 2021 at: https://www.asthmahandbook.org.au/management/children
- 4 Pijnenburg MW, Fleming L. Advances in understanding and reducing the burden of severe asthma in children. Lancet Respir Med 2020; 8 (10) 1032-1044
- 5 Gibson PG, Powell H. Written action plans for asthma: an evidence-based review of the key components. Thorax 2004; 59 (02) 94-99
- 6 Zemek RL, Bhogal SK, Ducharme FM. Systematic review of randomized controlled trials examining written action plans in children: what is the plan?. Arch Pediatr Adolesc Med 2008; 162 (02) 157-163
- 7 Abramson MJ, Bailey MJ, Couper FJ. et al; Victorian Asthma Mortality Study Group. Are asthma medications and management related to deaths from asthma?. Am J Respir Crit Care Med 2001; 163 (01) 12-18
- 8 Cicutto L, Dingae MB, Langmack EL. Improving asthma care in rural primary care practices: a performance improvement project. J Contin Educ Health Prof 2014; 34 (04) 205-214
- 9 Chapman KR, Boulet LP, Rea RM, Franssen E. Suboptimal asthma control: prevalence, detection and consequences in general practice. Eur Respir J 2008; 31 (02) 320-325
- 10 FitzGerald JM, Boulet LP, McIvor RA, Zimmerman S, Chapman KR. Asthma control in Canada remains suboptimal: the Reality of Asthma Control (TRAC) study. Can Respir J 2006; 13 (05) 253-259
- 11 Australian Bureau of Statistics (ABS). Australian Institute of Health and Welfare (AIHW) Microdata: National Health Survey, 2017 -2018, detailedmicrodata, DataLab. ABS cat. no. 4324.0.55.001. Canberra: ABS. Findings based on AIHW analysis of ABS microdata 2019; Accessed December 15, 2021 at: https://www.abs.gov.au/statistics/microdata-tablebuilder/available-microdata-tablebuilder/national-health-survey
- 12 Gupta S, Price C, Agarwal G. et al. The Electronic Asthma Management System (eAMS) improves primary care asthma management. Eur Respir J 2019; 53 (04) 1802241
- 13 Bender BG. Electronic health record–generated interventions to reduce asthma risk: seeing the glass half full. J Allergy Clin Immunol 2014; 2 (04) 457-458
- 14 Zeiger RS, Schatz M, Li Q, Solari PG, Zazzali JL, Chen W. Real-time asthma outreach reduces excessive short-acting β2-agonist use: a randomized study. J Allergy Clin Immunol Pract 2014; 2 (04) 445-456
- 15 Taite A, Podgers D, Olajos-Clow J. et al. Enabling asthma management and outcomes monitoring through standardized EMR data and eTools. Eur Respir J 2017; 50 (Suppl. 61) PA2778
- 16 Tiase VL, Wawrzynski SE, Sward KA. et al. provider preferences for patient-generated health data displays in pediatric asthma: a participatory design approach. Appl Clin Inform 2021; 12 (03) 664-674
- 17 Farzandipour M, Nabovati E, Sharif R, Arani MH, Anvari S. Patient self-management of asthma using mobile health applications: a systematic review of the functionalities and effects. Appl Clin Inform 2017; 8 (04) 1068-1081
- 18 Fleming L, Murray C, Bansal AT. et al; U-BIOPRED Study Group. The burden of severe asthma in childhood and adolescence: results from the paediatric U-BIOPRED cohorts. Eur Respir J 2015; 46 (05) 1322-1333
- 19 Guerra S, Stern DA, Zhou M. et al. Combined effects of parental and active smoking on early lung function deficits: a prospective study from birth to age 26 years. Thorax 2013; 68 (11) 1021-1028
Address for correspondence
Publication History
Received: 28 April 2022
Accepted: 17 August 2022
Accepted Manuscript online:
31 August 2022
Article published online:
19 October 2022
© 2022. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Australian Institute of Health and Welfare (AIHW) Cat No. . ACM 33 Asthma; 2020
- 2 Asher I, Pearce N. Global burden of asthma among children. Int J Tuberc Lung Dis 2014; 18 (11) 1269-1278
- 3 National Asthma Council Australia. . Australian Asthma Handbook – Management in Children. Accessed December 15, 2021 at: https://www.asthmahandbook.org.au/management/children
- 4 Pijnenburg MW, Fleming L. Advances in understanding and reducing the burden of severe asthma in children. Lancet Respir Med 2020; 8 (10) 1032-1044
- 5 Gibson PG, Powell H. Written action plans for asthma: an evidence-based review of the key components. Thorax 2004; 59 (02) 94-99
- 6 Zemek RL, Bhogal SK, Ducharme FM. Systematic review of randomized controlled trials examining written action plans in children: what is the plan?. Arch Pediatr Adolesc Med 2008; 162 (02) 157-163
- 7 Abramson MJ, Bailey MJ, Couper FJ. et al; Victorian Asthma Mortality Study Group. Are asthma medications and management related to deaths from asthma?. Am J Respir Crit Care Med 2001; 163 (01) 12-18
- 8 Cicutto L, Dingae MB, Langmack EL. Improving asthma care in rural primary care practices: a performance improvement project. J Contin Educ Health Prof 2014; 34 (04) 205-214
- 9 Chapman KR, Boulet LP, Rea RM, Franssen E. Suboptimal asthma control: prevalence, detection and consequences in general practice. Eur Respir J 2008; 31 (02) 320-325
- 10 FitzGerald JM, Boulet LP, McIvor RA, Zimmerman S, Chapman KR. Asthma control in Canada remains suboptimal: the Reality of Asthma Control (TRAC) study. Can Respir J 2006; 13 (05) 253-259
- 11 Australian Bureau of Statistics (ABS). Australian Institute of Health and Welfare (AIHW) Microdata: National Health Survey, 2017 -2018, detailedmicrodata, DataLab. ABS cat. no. 4324.0.55.001. Canberra: ABS. Findings based on AIHW analysis of ABS microdata 2019; Accessed December 15, 2021 at: https://www.abs.gov.au/statistics/microdata-tablebuilder/available-microdata-tablebuilder/national-health-survey
- 12 Gupta S, Price C, Agarwal G. et al. The Electronic Asthma Management System (eAMS) improves primary care asthma management. Eur Respir J 2019; 53 (04) 1802241
- 13 Bender BG. Electronic health record–generated interventions to reduce asthma risk: seeing the glass half full. J Allergy Clin Immunol 2014; 2 (04) 457-458
- 14 Zeiger RS, Schatz M, Li Q, Solari PG, Zazzali JL, Chen W. Real-time asthma outreach reduces excessive short-acting β2-agonist use: a randomized study. J Allergy Clin Immunol Pract 2014; 2 (04) 445-456
- 15 Taite A, Podgers D, Olajos-Clow J. et al. Enabling asthma management and outcomes monitoring through standardized EMR data and eTools. Eur Respir J 2017; 50 (Suppl. 61) PA2778
- 16 Tiase VL, Wawrzynski SE, Sward KA. et al. provider preferences for patient-generated health data displays in pediatric asthma: a participatory design approach. Appl Clin Inform 2021; 12 (03) 664-674
- 17 Farzandipour M, Nabovati E, Sharif R, Arani MH, Anvari S. Patient self-management of asthma using mobile health applications: a systematic review of the functionalities and effects. Appl Clin Inform 2017; 8 (04) 1068-1081
- 18 Fleming L, Murray C, Bansal AT. et al; U-BIOPRED Study Group. The burden of severe asthma in childhood and adolescence: results from the paediatric U-BIOPRED cohorts. Eur Respir J 2015; 46 (05) 1322-1333
- 19 Guerra S, Stern DA, Zhou M. et al. Combined effects of parental and active smoking on early lung function deficits: a prospective study from birth to age 26 years. Thorax 2013; 68 (11) 1021-1028