

Subscribe to RSS
DOI: 10.1055/a-1158-8948
Endoscopic submucosal dissection by transnasal endoscope for esophageal cancer with pharyngoesophageal anastomotic stricture after total pharyngo-laryngo-esophagectomy
Authors

Patients with squamous cell carcinoma (SCC) of the head and neck often develop secondary esophageal carcinomas. We describe a successful case of endoscopic submucosal dissection (ESD) using a transnasal endoscope to treat a patient with esophageal cancer with a pharyngoesophageal anastomotic stricture after total pharyngo-laryngo-esophagectomy (TPLE).
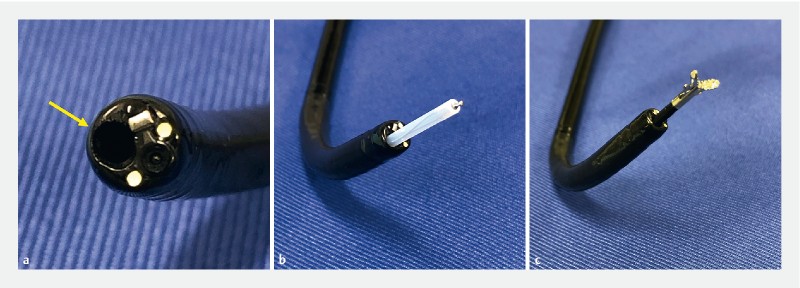
A 60-year-old man was referred to our division for treatment of esophageal cancer. The patient had undergone TPLE for advanced hypopharyngeal cancer 5 years previously, and endoscopy revealed a flat lesion in the lower third of the esophagus ([Fig. 1 a, b]). The patient had a pharyngoesophageal anastomotic stricture after the TPLE that could not be passed using a conventional endoscope ([Fig. 1 c]). Endoscopic balloon dilation was not possible because of the presence of a voice prosthesis ([Fig. 1 d]). Recently, an improved transnasal endoscope, the EG-L580NW (Fujifilm, Tokyo, Japan), has become available, with a 5.8-mm outer diameter and a 2.4-mm forceps diameter ([Fig. 2 a]) [1]. An ultrathin needle-type device (Souten; Kaneka Medics, Tokyo, Japan) and hemostasis forceps (Raicho; Kaneka Medics, Tokyo, Japan) can be used with this endoscope ([Fig. 2 b, c]) [2]. Thus, we performed ESD using a transnasal endoscope to treat the esophageal cancer ([Video 1]).

Video 1 Endoscopic submucosal dissection by transnasal endoscope for esophageal cancer with pharyngoesophageal anastomotic stricture after total pharyngo-laryngo-esophagectomy.
Circumferential incisions were made using the Souten with Endo Cut I mode (VIO 300D; Erbe, Tübingen, Germany; effect 2, duration 2, interval 2) ([Fig. 3 a, b]). To control bleeding, the Raicho forceps was used in soft coagulation mode at 50 W. Submucosal dissection was performed using the Souten and swift coagulation mode (effect 3, 30 W) ([Fig. 3 c]). Finally, en bloc resection was achieved without injury to the muscularis propria ([Fig. 3 d]). Histological examination revealed R0 resection of the squamous cell carcinoma, which was limited to the epithelium ([Fig. 4]).


Esophageal ESD using a transnasal endoscope was useful in treating esophageal cancer with an anastomotic stricture that could not be passed using a conventional endoscope.
Endoscopy_UCTN_Code_TTT_1AO_2AG
Endoscopy E-Videos is a free access online section, reporting on interesting cases and new techniques
in gastroenterological endoscopy. All papers include a high
quality video and all contributions are
freely accessible online.
This section has its own submission
website at
https://mc.manuscriptcentral.com/e-videos
Competing interests
The authors declare that they have no conflict of interest.
-
References
- 1 Suzuki T, Kitagawa Y, Nankinzan R. et al. Early gastric cancer diagnostic ability of ultrathin endoscope loaded with laser light source. World J Gastroenterol 2019; 25: 1378-1386
- 2 Minato Y, Sakai E, Ohata K. Conscious transnasal hybrid endoscopic submucosal dissection enables safe and painless en bloc resection in elderly patients with early gastric cancer. VideoGIE 2019; 4: 157-158
Corresponding author
Publication History
Article published online:
12 May 2020
© 2020. Thieme. All rights reserved.
Georg Thieme Verlag KG
Rüdigerstraße 14, 70469 Stuttgart, Germany
-
References
- 1 Suzuki T, Kitagawa Y, Nankinzan R. et al. Early gastric cancer diagnostic ability of ultrathin endoscope loaded with laser light source. World J Gastroenterol 2019; 25: 1378-1386
- 2 Minato Y, Sakai E, Ohata K. Conscious transnasal hybrid endoscopic submucosal dissection enables safe and painless en bloc resection in elderly patients with early gastric cancer. VideoGIE 2019; 4: 157-158