

RSS-Feed abonnieren
DOI: 10.4103/ajns.AJNS_199_17
Ipsilateral two spontaneous chronic calcified epidural hematoma
Autor*innen

Sir,
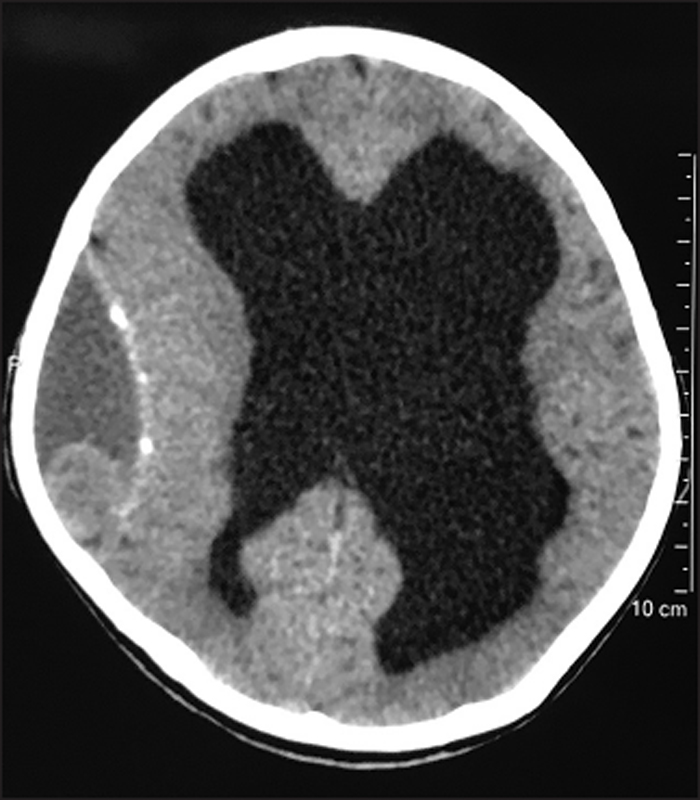
A 12-year-old child presented with a complaint of headache and vomiting following fall from bike, 2 days ago. Computed tomography (CT) head revealed acute on chronic calcified epidural hematoma (EDH) at the right frontal and parietal region with dilated ventricles and no midline shift [[Figure 1]]. The child improved on conservative treatment. His mental and neurological functions were normal, and there was no papilledema. He had a history of tubercular meningitis and hydrocephalus at the age of 4 years. Shunt surgery was advised then but refused by parents. There was no history of significant head injury or coagulation disorder. Magnetic resonance imaging brain confirmed the findings and showed blood of various stages [[Figure 2]]a, [[Figure 2]]b, [[Figure 2]]c, [[Figure 2]]d. The maximum thickness of hematoma was 4.7 cm. He has been on a regular follow-up. At follow-up after 1 month, he showed neither any recurrence of previous symptoms nor of neurological deterioration. At follow-up after 3 months, the patient was not harboring any symptoms. His NCCT head [[Figure 3]] head revealed disappearance of smaller EDH (frontal) and reduction in the size of parietal larger EDH (size 2.4 cm).


The patient's parents gave informed consent for patient's data publication. We took approval from ethical committee at our institute.
Chronic EDH is a rare type of bleed. It has been mostly reported in the younger age group.
The probable hypothesis is the presence of lax adhesions between the dura and the calvarium.[[1]] The blood products cause inflammatory reaction that may be the probable cause of calcification.[[1]] In children, EDH is mostly of venous origin, and venous blood takes longer time to accumulate in adequate volume to cause significant mass effect. That is, why children present with chronic EDH and symptoms of headache and seizures rather than acute deterioration in consciousness.[[2]] The probable mechanism of calcification in chronic subdural hematoma (CSDH) is the persistence of blood product leading to fibroblasts activity and secretion of local factors which cause calcification.[[3]] The calcification usually takes around 6 months to form in a CSDH.[[3]]
The occurrence of two or more EDHs on the same side is quite rare, and there is a single case report of two chronic EDHs on the same side.[[2]] Our case is second such case of multiple EDH on the same side.
Furthermore, expansion of an EDH may also result from repeated bleeding from the inner table of the skull or due to oozing from the dural surface veins.[[4]] In our case, rebleed occurred after trauma. Such episodes may cause deterioration and needs surgical decompression. This case had no midline shift. Observation trial showed significant radiological improvement.
The management guidelines for chronic EDH are not defined due to lack of large cohorts. According to Sinha and Borkar, conservative management of EDH is not always effective in children and serial CT head is mandatory if planning conservative management.[[5]] Urgent evacuation of EDH should be considered for children with progressive neurological deterioration.[[5]] We think that the management strategy should be similar to chronic calcified subdural hematoma as both are chronic and calcified and have a membrane separating from the brain. That's why surgery may be considered if there are acute deterioration, mass effect, and no resolution of hematoma on conservative management. The conservative treatment and observation may be tried if there is no mass effect.
Financial support and sponsorship
Nil.
Publikationsverlauf
Artikel online veröffentlicht:
09. September 2022
© 2019. Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/)
Thieme Medical and Scientific Publishers Pvt. Ltd.
A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
-
References
- 1 Jain SK, Sundar IV, Sharma V, Arora R, Prasanna KL. Chronic ossified extradural hematoma on the opposite side of the ventriculoperitoneal shunt procedure: A rare case report. Saudi J Health Sci 2012;1:159-61.
- 2 Kaye EM, Cass PR, Dooling E, Rosman NP. Chronic epidural hematomas in childhood: Increased recognition and non-surgical management. Pediatr Neurol 1985;1:255-9.
- 3 Pappamikail L, Rato R, Novais G, Bernardo E. Chronic calcified subdural hematoma: Case report and review of the literature. Surg Neurol Int 2013;4:21.
- 4 Dawar P, Phalak M, Sinha S, Sharma BS. Same side double chronic calcified epidural hematoma: Case report and review of literature. Neurol India 2013;61:195-7.
- 5 Sinha S, Borkar S. Chronic calcified extradural hematoma in a child: Case report and review of literature. IJNT 2008;5:51-2.