
RSS-Feed abonnieren
DOI: 10.1055/s-2006-944523
Tako-Tsubo-Kardiomyopathie - was steckt dahinter?
Publikationsverlauf
Publikationsdatum:
31. Juli 2006 (online)

Einleitung
Die Tako-Tsubo-Kardiomyopathie wurde erstmals 1990 in Japan beschrieben. Das Krankheitsbild verläuft klinisch wie ein akutes Koronarsyndrom und ist gekennzeichnet durch eine reversible Wandbewegungsstörung des linken Ventrikels mit apikaler Akinesie und einer Hyperkontraktion der basalen Myokardabschnitte, wobei angiographisch im Unterschied zum Myokardinfarkt keine signifikanten Koronarstenosen nachweisbar sind [1] [2] [3] [4] [5] [6]. Bei der Ventrikulographie ähnelt die endsystolische Konfiguration des linken Ventrikels „Tako-Tsubo”, einem runden Tontopf mit engem Hals, der in Japan zum Fangen von Tintenfischen benutzt wird. Daher wurde die Erkrankung „Tako-Tsubo”- oder „Ampulla”-Kardiomyopathie genannt [1] [2] [3] [5] [7]. Wegen der ballonartigen systolischen Aufweitung des linksventrikulären Apex (Abb. [1]) findet sich in der Literatur auch die Bezeichnung „apical ballooning syndrome” [4] [6]. Nachdem die Tako-Tsubo-Kardiomyopathie zunächst fast ausschließlich bei japanischen Patienten beobachtet wurde, sind in den letzten Jahren mehrere Berichte auch in Europa und den USA erschienen, sodass die Erkrankung inzwischen relativ gut charakterisiert ist [8] [9] [10] [11] [12] [13] [14] [15].
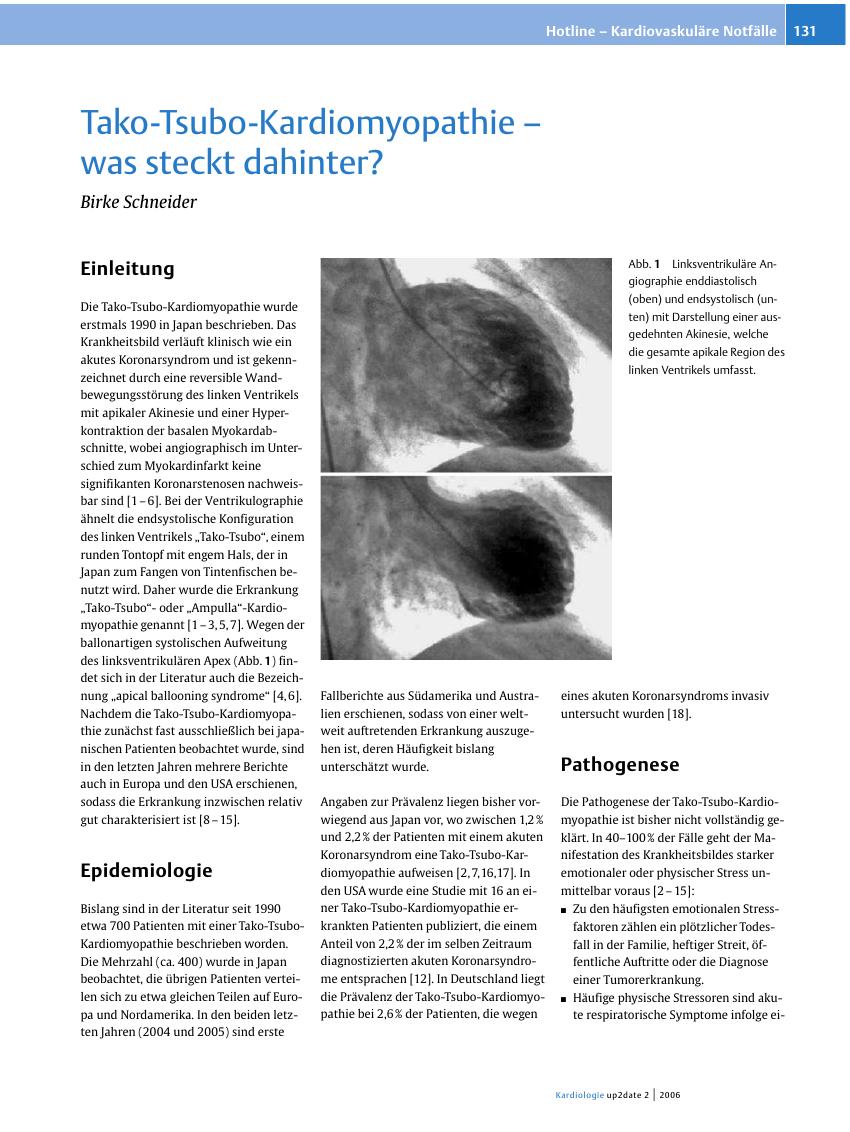
Abb. 1 Linksventrikuläre Angiographie enddiastolisch (oben) und endsystolisch (unten) mit Darstellung einer ausgedehnten Akinesie, welche die gesamte apikale Region des linken Ventrikels umfasst.
Literatur
-
1 Sato H, Tateishi H, Uchida T. et al .
Tako-tsubo-type cardiomyopathy due to multivessel spasm. In: Kodama K, Haze K, Han M (Hrsg.) Clinical aspect of myocardial injury: from ischemia to heart failure. Tokyo; Kagakuhyouronsya Co 1999: 56-64 - 2 Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases. J Cardiol. 1991; 21 203-214
- 3 Kawai S, Suzuki H, Yamaguchi H. et al . Ampulla cardiomyopathy („Takotsubo” cardiomyopathy). Reversible left ventricular dysfunction with ST segment elevation. Jpn Circ J. 2000; 64 156-159
- 4 Tsuchihashi K, Ueshima K, Uchida T. et al . , for the Angina Pectoris-Myocardial Infarction Investigations in Japan. Transient left ventricular apical ballooning without coronary artery stenosis: A novel heart syndrome mimicking acute myocardial infarction. J Am Coll Cardiol. 2001; 38 11-18
- 5 Kurisu S, Sato H, Kawagoe T. et al . Tako-tsubo like left ventricular dysfunction with ST-segment elevation: A novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J. 2002; 143 448-455
- 6 Abe Y, Kondo M, Matsuoka R, Araki M, Dohyama K, Tanio H. Assessment of clinical features in transient left ventricular apical ballooning. J Am Coll Cardiol. 2003; 41 737-742
- 7 Matsuoka K, Okubo S, Fujii E. et al . Evaluation of the arrhythmogenicity of stress-induced „Takotsubo cardiomyopathy” from the time course of the 12-lead surface electrocardiogram. Am J Cardiol. 2003; 92 230-233
- 8 Pavin D, Le Breton H, Daubert C. Human stress cardiomyopathy mimicking acute myocardial syndrome. Heart. 1997; 78 509-511
- 9 Desmet W JR, Adriaenssens B FM, Dens J AY. Apical ballooning of the left ventricle: first series in white patients. Heart. 2003; 89 1027-1031
- 10 Ibanez B, Navarro F, Farre J. et al . Tako-tsubo transient left ventricular apical ballooning is associated with a left anterior descending coronary artery with a long course along the apical diaphragmatic surface of the left ventricle. Rev Esp Cardiol. 2004; 57 209-216
- 11 Seth P S, Aurigemma G P, Krasnow J M, Tighe D A, Untereker W J, Meyer T E. A syndrome of transient left ventricular apical wall motion abnormality in the absence of coronary disease: A perspective from the United States. Cardiology. 2003; 100 61-66
- 12 Bybee K A, Prasad A, Barsness G W. et al . Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular apical ballooning syndrome. Am J Cardiol. 2004; 94 343-346
- 13 Sharkey S W, Lesser J R, Zenovich A G. et al . Acute and reversible cardiomyopathy provoked by stress in women from the United States. Circulation. 2005; 111 472-479
- 14 Wittstein I S, Thiemann D R, Lima J AC. et al . Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005; 352 539-548
- 15 Glöckner D, Dissmann M, Behrens S. Atypisches koronares Ischämiesyndrom mit ballonartiger passagerer Akinesie des linksventrikulären Apex („apical ballooning”) ohne Nachweis einer signifikanten koronaren Makroangiopathie. Z Kardiol. 2004; 93 156-161
- 16 Ito K, Sugihara H, Katoh S, Azuma A, Nakagawa M. Assessment of Takotsubo (ampulla) cardiomyopathy using 99mTc-tetrofosmin myocardial SPECT - comparison with acute coronary syndrome. Ann Nucl Med. 2003; 17 115-122
- 17 Akashi Y J, Nakazawa K, Sakakibara M, Miyake F, Musha H, Sasaka K. 123I-MIBG myocardial scintigraphy in patients with „takotsubo” cardiomyopathy. J Nucl Med. 2004; 45 1121-1127
- 18 Schneider B, Koch S, Stein J. Transient left ventricular dysfunction: differences between apical and mid-ventricular involvement. Circulation. 2005; 112 (Suppl II) 692
- 19 Shaw T RD, Rafferty P, Tait G W. Transient shock and myocardial impairment caused by phaechromocytoma crisis. Br Heart J. 1987; 57 194-198
- 20 Kono T, Morita H, Kuroiwa T, Onaka H, Takatsuka H, Fujiwara A. Left ventricular wall motion abnormalities in patients with subarachnoid hemorrhage: neurogenic stunned myocardium. J Am Coll Cardiol. 1994; 24 636-640
- 21 Ueyama T, Hano T, Kasamatsu K, Yamamoto K, Tsuruo Y, Nishio I. Estrogen attenuates the emotional stress-induced cardiac responses in the animal model of Tako-tsubo (Ampulla) cardiomyopathy. J Cardiovasc Pharmacol. 2003; 42 (Suppl 1) S117-S119
- 22 Pison L, De Vusser P, Mullens W. Apical ballooning in relatives. Heart. 2004; 90 e67
- 23 Mori H, Ishikawa S, Kojima S. et al . Increased responsiveness of left ventricular apical myocardium to adrenergic stimuli. Cardiovasc Res. 1993; 27 192-198
- 24 Merli E, Sutcliffe S, Gori M. et al . Tako-Tsubo cardiomyopathy: new insights into the possible underlying pathophysiology. Eur J Echocardiography. 2006; 7 53-61
- 25 Kurisu S, Inoue I, Kawagoe T. et al . Left ventricular apical thrombus formation in a patient with suspected tako-tsubo-like left ventricular dysfunction. Circ J. 2003; 67 556-558
- 26 Peraira Moral J R, Segovia Cubero J, Oteo Dominguez J F, Ortiz Oficialdegui P, Fuentes Manso R, MartinJudez V. A case of transient left ventricular apical ballooning with an unusual complication. Rev Esp Cardiol. 2002; 55 1328-1332
- 27 Akashi Y J, Tejima T, Sakurada H. et al . Left ventricular rupture associated with takotsubo cardiomyopathy. Mayo Clin Proc. 2004; 79 821-824
- 28 Sakai K, Ochiai H, Katayama N. et al . Ventricular septal perforation in a patient with takotsubo cardiomyopathy. Circ J. 2005; 69 365-367
- 29 Ogura R, Hiasa Y, Takahashi T. et al . Specific findings of the standard 12-lead ECG in patients with „Takotsubo” cardiomyopathy. Comparison with the findings of acute anterior myocardial infarction. Circ J. 2003; 67 687-690
- 30 Kurisu S, Inoue I, Kawagoe T. et al . Time course of electrocardiographic changes in patients with tako-tsubo syndrome. Comparison with acute myocardial infarction with minimal enzymatic release. Circ J. 2004; 68 77-81
- 31 Owa M, Aizawa K, Urasawa N. et al . Emotional stress-induced „ampulla cardiomyopathy”. Discrepancy between the metabolic and sympathetic innervation imaging performed during the recovery course. Jpn Circ J. 2001; 65 349-352
- 32 Kyuma M, Tsuchihashi K, Shinshi Y. et al . Effect of intravenous propranolol on left ventricular apical ballooning without coronary artery stenosis (ampulla cardiomyopathy). Three cases. Circ J. 2002; 66 1181-1184
Dr. med. Birke Schneider
Klinik für Kardiologie
Sana Kliniken Lübeck GmbH · Kronsforder Allee 71 - 73 · 23560 Lübeck
eMail: b.schneider@sana-luebeck.de