

Subscribe to RSS
DOI: 10.1055/s-0034-1373795
What Is Too Big? Uterine Artery Embolization of a Large Fibroid Causing Abdominal Compartment Syndrome
Authors
Publication History
Publication Date:
21 May 2014 (online)


Case Report
A 39-year-old woman with a history of spastic cerebral palsy, mental retardation, and chronic worsening nausea and vomiting presented to the emergency department from a group home with complaints of hematemesis. The patient was admitted to the hospital and underwent an upper endoscopy, which revealed a nonbleeding ulcer that was treated medically. The patient was advanced to a liquid diet and promptly became symptomatic again with nausea and guaiac-positive emesis. After further discussion with her caregivers, it became clear that the patient's nausea and vomiting had been worsening before her admission. At this point, the patient's prior radiologic studies were reviewed for a possible etiology.
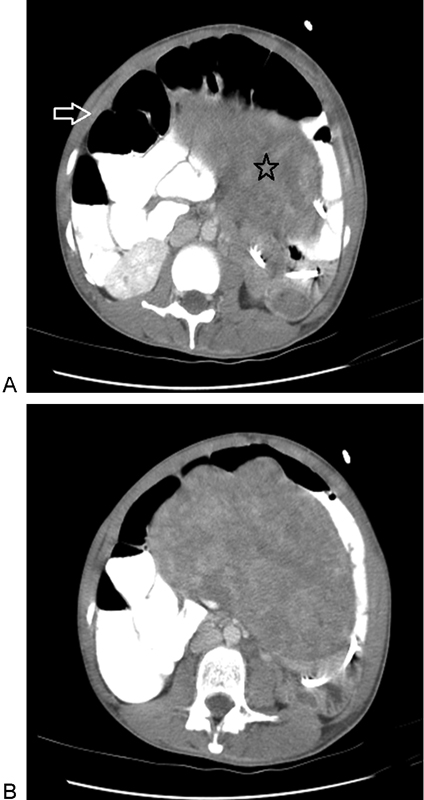
The patient had a computed tomographic (CT) scan of the abdomen and pelvis 5 months earlier that demonstrated multiple, large uterine fibroids, the largest measuring 16 cm × 10 cm × 10 cm ([Fig. 1]). After multiple studies including an upper endoscopy, the gastroenterologist concluded that the patient's hematemesis was likely due to reflux esophagitis from mass effect by the fibroids. The gynecologist was consulted regarding treatment for the large fibroids. A repeat CT of the abdomen and pelvis was performed that again demonstrated a multifibroid uterus with one prominent fibroid, unchanged from the previous study. Of note, the small bowel was unremarkable on this CT scan.

The patient's gynecologic workup was delayed, as the patient was transferred to the intensive care unit (ICU) for methicillin-resistant Staphylococcus epidermidis bacteremia, during which time the patient had a peripherally inserted central catheter placed and was started on total parenteral nutrition. Once the patient was medically stabilized, the gynecologist was again consulted and Lupron therapy was initiated for treatment of her fibroids. The patient's hospital stay was further confounded by a biopsy of a left breast mass noted on mammography, which turned out to be a phyllodes tumor; in addition, she was treated for an unrelated Clostridium difficile infection during her admission.
The patient's nausea and vomiting continued to progress, at which point gastroenterologist was again consulted. The gastroenterologist felt that a feeding gastrostomy tube was not indicated, as the patient's symptoms were likely related to small bowel obstruction from the uterine fibroids. Interventional radiologist placed a gastrojejunostomy tube, after which the patient was placed on wall suction due to continued symptoms and high gastric outputs. After improvement of her symptoms, tube feeds were initiated; this caused increased nausea and vomiting, again leading to the theory that her fibroids were causing mechanical obstruction. A repeat CT of the abdomen and pelvis was performed, which demonstrated a small bowel obstruction as a result of her uterine fibroids ([Fig. 2]).
The patient was scheduled for a hysterectomy and left mastectomy but developed a fever (temperature, 101.3°F) and became hypotensive to 77/46 mm Hg. Multiple blood cultures drawn at this time were positive for Candida parapsilosis, and the surgery was canceled. Further workup revealed a vegetation on the mitral valve; however, cardiothoracic surgery determined the patient was too cachectic to proceed with operative repair. After approximately 2-month hospital stay, the patient was discharged to her group home on tube feeds, Reglan, and Prevacid, and instructed to follow up with interventional radiologist for evaluation for uterine artery embolization (UAE), as she was deemed too poor a surgical candidate for hysterectomy.
Approximately 2 months later, the patient had a magnetic resonance imaging scan of the pelvis, again demonstrating the multifibroid uterus with a large pedunculated fibroid ([Fig. 3]). She subsequently underwent bilateral UAE. Upon initial aortic injection, markedly enlarged bilateral uterine arteries were seen, the right greater than the left, as well as a hypervascular enlarged fibroid uterus and a prominent right ovarian artery ([Fig. 4]). The left uterine artery was embolized with two vials of 355 to 500 μm of polyvinyl alcohol (PVA) particles; the right uterine artery was embolized with two vials of 355 to 500 μm, four vials of 500 to 710 μm PVA particles, and ½ packet of gel-foam made into a slurry. At the end of the procedure, minimal flow was seen in bilateral uterine arteries, although slightly more flow was seen in the right uterine artery when compared with the left ([Fig. 5]).



Following the procedure, the patient continued to have nausea, vomiting, and abdominal pain. Three days post-UAE, the patient was noted to have increasing abdominal distension and pain; the following day, the patient deteriorated even further and was found to have free intraperitoneal gas on the abdominal radiographs ([Fig. 6]). General surgery was consulted for an acute abdomen and the patient was urgently transferred to the surgical ICU with hypotension, tachycardia, and dyspnea requiring intubation. After large volume resuscitation, the patient was taken urgently to the operating room.

In the operating room, the patient was found to have copious amounts of murky-free peritoneal fluid, a complete sigmoid colonic obstruction with a zone of transition in the region of the descending/sigmoid colon due to compression from the enlarged uterine fibroid, and several areas of ischemic small bowel. These findings were consistent with abdominal compartment syndrome (ACS). Intraoperatively, the gynecologist was consulted and performed a myomectomy to treat the obstructing fibroid which measured 17.5 cm × 14 cm × 9.2 cm, larger than the preprocedure imaging demonstrated, and pedunculated extending off the fundus of the uterus. The patient also underwent a total colectomy and partial small bowel resection to remove the ischemic segments. The surgeons were unable to primarily close the abdomen, so the patient was transferred to the ICU with an open abdomen. The patient subsequently underwent multiple abdominal washouts in the operating room, and further resection of small bowel with a new ileostomy created. The patient was ultimately able to undergo primary closure after multiple attempts.
After recovery, the patient was discharged to a skilled nursing facility. She continued to have severe intestinal paresis, ultimately making enteral nutrition impossible. The patient was readmitted several times for bacteremia and fungemia, and ultimately 1.5 years after her UAE the patient was provided comfort care only and died.
-
References
- 1 Goodwin SC, Spies JB. Uterine fibroid embolization. N Engl J Med 2009; 361 (7) 690-697
- 2 Ravina JH, Herbreteau D, Ciraru-Vigneron N , et al. Arterial embolisation to treat uterine myomata. Lancet 1995; 346 (8976) 671-672
- 3 Kitamura Y, Ascher SM, Cooper C , et al. Imaging manifestations of complications associated with uterine artery embolization. Radiographics 2005; 25 (Suppl. 01) S119-S132
- 4 Schirf BE, Vogelzang RL, Chrisman HB. Complications of uterine fibroid embolization. Semin Intervent Radiol 2006; 23 (2) 143-149
- 5 Smith SJ. Uterine fibroid embolization. Am Fam Physician 2000; 61 (12) 3601-3607 , 3611–3612
- 6 de Blok S, de Vries C, Prinssen HM, Blaauwgeers HL, Jorna-Meijer LB. Fatal sepsis after uterine artery embolization with microspheres. J Vasc Interv Radiol 2003; 14 (6) 779-783
- 7 Vashisht A, Studd J, Carey A, Burn P. Fatal septicaemia after fibroid embolisation. Lancet 1999; 354 (9175) 307-308
- 8 Lefebvre GG, Vilos G, Asch M ; Society of Obstetricians and Gynaecologists of Canada; Canadian Association of Radiologists; Canadian Interventional Radiology Association. Uterine fibroid embolization (UFE). J Obstet Gynaecol Can 2004; 26 (10) 899-911 , 913–928
- 9 Hamoda H, Tait P, Edmonds DK. Fatal pulmonary embolus after uterine artery fibroid embolisation. Cardiovasc Intervent Radiol 2009; 32 (5) 1080-1082
- 10 Lumsden MA. Embolization versus myomectomy versus hysterectomy: which is best, when?. Hum Reprod 2002; 17 (2) 253-259
- 11 Spies JB, Roth AR, Jha RC , et al. Leiomyomata treated with uterine artery embolization: factors associated with successful symptom and imaging outcome. Radiology 2002; 222 (1) 45-52
- 12 Smeets AJ, Nijenhuis RJ, van Rooij WJ , et al. Uterine artery embolization in patients with a large fibroid burden: long-term clinical and MR follow-up. Cardiovasc Intervent Radiol 2010; 33 (5) 943-948
- 13 Worthington-Kirsch RL, Popky GL, Hutchins Jr FL. Uterine arterial embolization for the management of leiomyomas: quality-of-life assessment and clinical response. Radiology 1998; 208 (3) 625-629
- 14 Goodwin SC, McLucas B, Lee M , et al. Uterine artery embolization for the treatment of uterine leiomyomata midterm results. J Vasc Interv Radiol 1999; 10 (9) 1159-1165
- 15 Pelage JP, Le Dref O, Soyer P , et al. Fibroid-related menorrhagia: treatment with superselective embolization of the uterine arteries and midterm follow-up. Radiology 2000; 215 (2) 428-431
- 16 Katsumori T, Nakajima K, Mihara T. Is a large fibroid a high-risk factor for uterine artery embolization?. AJR Am J Roentgenol 2003; 181 (5) 1309-1314
- 17 Spies JB, Ascher SA, Roth AR, Kim J, Levy EB, Gomez-Jorge J. Uterine artery embolization for leiomyomata. Obstet Gynecol 2001; 98 (1) 29-34
- 18 Vegar-Brozovic V, Stoic-Brezak J. Pathophysiology of abdominal compartment syndrome. Transplant Proc 2006; 38 (3) 833-835
- 19 Patel A, Lall CG, Jennings SG, Sandrasegaran K. Abdominal compartment syndrome. AJR Am J Roentgenol 2007; 189 (5) 1037-1043
- 20 Bailey J, Shapiro MJ. Abdominal compartment syndrome. Crit Care 2000; 4 (1) 23-29
- 21 Sugrue M. Abdominal compartment syndrome. Curr Opin Crit Care 2005; 11 (4) 333-338